Ureterolithiasis is a type of urolithiasis and is characterized by the presence of stones in the ureter, which are an accumulation of oxalates, calcium salts and phosphates.
Stones in the urinary canal appear due to their migration from the renal pelvis. This pathology is diagnosed in the male population, but in women it occurs in a more severe form.
Location in relation to organs and peritoneum
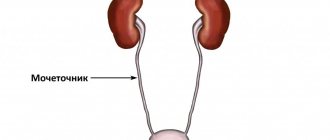
The exit from the kidney is formed by the narrowed opening of the pelvis. The orifice of the ureter is located inside the bladder. It passes through the wall and forms bilateral slit-like openings on the mucous membrane of the bladder. At the confluence of the upper part, a fold is formed, covered with a mucous membrane.
It is customary to distinguish 3 sections of the ureter.
Abdominal - passes through the retroperitoneal tissue in the posterior wall of the abdomen, then goes along the lateral surface to the small pelvis, adjoining the psoas major muscle in front. The initial part of the right ureter lies behind the duodenum, and closer to the pelvic region - behind the mesentery of the sigmoid colon.
The reference point for the left is the posterior wall of the bend between the duodenum and jejunum. In the zone of transition to the pelvic part, the right ureter lies behind the base of the mesentery.
Pelvic - in women it is located behind the ovary, bending around the cervix from the side, runs along the broad ligament of the uterus, and fits between the wall of the bladder and the vagina. In men, the ureteric tube passes outward and anterior to the vas deferens, passing through it, enters the bladder almost under the upper edge of the seminal vesicle.
Distal section (farthest from the kidney) - passes through the thickness of the bladder wall. It is up to 1.5 cm in length. It's called intramural.
In clinical practice, it is more convenient to divide the ureter along its length into three equal parts:
- top;
- average;
- bottom.
SURGICAL ANATOMY OF THE URETER
SURGICAL ANATOMY OF THE URETER
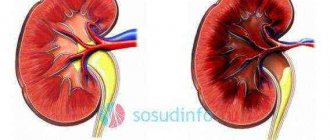
The renal pelvis, narrowing, passes into the ureter (ureter), which is a long, cylindrical tube connecting the renal pelvis with the bladder (Fig. 1, 2, 3). There are almost equal two sections: abdominal (pars abdominalis) and pelvic (pars pelvina).
The length of the ureter in men is 30-32 cm, in women - 27-29 cm. The right ureter is slightly shorter than the left. About 2 cm of its length falls on the intravesical part. Its diameter is not the same throughout and ranges from 0.5 to 1 cm.
Along the ureter, it alternates between dilated (ampullae) and narrowed areas (isthmus) (cystoids). There are three narrowings: 1) at the junction of the pelvis and the ureter; 2) at the intersection of the ureter with the iliac vessels; 3) above the site of perforation by the ureter of the bladder. In places of physiological narrowing, the diameter of the ureter does not exceed 3-4 mm.
The ureter is located retroperitoneally, surrounded by fiber and a fascial sheath, which is a continuation of the outer capsule of the kidney, formed by the layers of the retroperitoneal fascia. The ureter is closely connected to the parietal layer of the peritoneum by connective tissue bridges. Both ureters lie on the anterior surface of the m. psoas major (Fig. 16), crossing it from top to bottom and from outside to inside. Approximately in the middle of the iliacus muscle, the ureter crosses the vasa testicularia with its anterior surface (in women - v. ovarica), and somewhat lower - with its posterior wall the genito-femoralis. At linea terminalis, the right ureter crosses the external iliac artery (a. iliac externa) in front, and the left ureter crosses the common iliac artery (a. iliaca communis). In the pelvic cavity, the ureter, being under the parietal layer of the peritoneum, is directed downward, medially to the bladder under the ductus deferens; in women, it passes through the tissue of the broad ligament of the uterus, crosses posteriorly and inferiorly a. uterina and along the anterolateral wall of the vaginal fundus approaches the bladder (Yu. L. Zolotko). In the bladder, the ureter with its upper wall forms a fold lined on both sides with mucous membrane, which is capable of contracting and closing its lumen. This valve under normal conditions prevents urine from flowing from the bladder into the pelvis. Inward from the right ureter is the inferior vena cava, outward is the inner edge of the ascending colon and cecum. Inward from the left ureter is the aorta, outward is the inner edge of the descending colon (D.N. Lubotsky).
Dimensions
In an adult, the length of the ureter is 28-34 cm. It depends on growth and is determined by the height of the kidneys when they are laid in the embryo. In women, the length of the organ is 2-2.5 cm shorter than in men. The right ureter is one centimeter shorter than the left one, since the location of the right kidney is slightly lower.
The lumen of the tube is not the same: narrowings alternate with areas of expansion. The narrowest parts are:
- next to the pelvis;
- at the border of the abdominal and pelvic sections;
- when entering the bladder.
Here the diameter of the ureter is 2-4 mm and 4-6 mm, respectively.
Segments are distinguished between the narrowed areas:
- above – pyelourethral segment;
- area of intersection with iliac vessels;
- lower – vesicoureteral segment.
The abdominal and pelvic sections of the ureter differ in lumen:
- in the area of the abdominal wall it is 8-15 mm;
- in the pelvis – uniform expansion of no more than 6 mm.
However, it should be noted that due to the good elasticity of the wall, the ureter is capable of expanding up to 8 cm in diameter. This ability helps to withstand urinary retention and congestion.
Definition: what is a ureter in biology
In the human body, the ureters play an important role and are an integral paired organ of the reproductive system. Their main function is to connect the kidneys and bladder. To put it simply, the ureter is a kind of tube, the diameter of which is 6-8 millimeters and the length is 25-30 centimeters.
To understand what ureters are, it is enough to imagine a medical catheter designed to collect urine. This is roughly what this organ looks like, to put it simply.
There are three natural narrowings in the ureter - this is the exit from the pelvis, at the beginning of the small pelvis and in the cystic wall. Urine moves through the ureter due to contractions of the cystoids. The functioning of organs is controlled by the autonomic nervous system. Calcium has a great influence on the functioning of the ureters. The strength of contraction depends on how much it is contained in muscles and tissues.
Sources used:
- https://labuda.blog/193308
- https://urohelp.guru/anatomy/mochetochnik.html
- https://tesisnet.ru/otdely-mochetochnika-stroenie-i-bolezni-mochetochnika-u-muzhchin.html
- https://simptom.info/urologiya/mochetochnik-eto
- https://pochkam.ru/mochevoj-puzyr-i-mocheispuskanie/mochetochnik-u-muzhchin.html
- https://4prostatit.com/urinary-system/urethra/kamni-v-mochetochnike-u-muzhchin.html
- https://fb.ru/article/469807/chto-takoe-mochetochniki-opisanie-funktsii-zabolevaniya
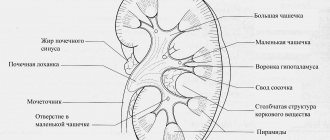
Histological structure
The structure of the ureter is supported by:
- from the inside - the mucous membrane;
- in the middle layer - muscle tissue;
- outside – adventitia and fascia.
The mucous membrane consists of:
- transitional epithelium located in several rows;
- plate containing elastic and collagen fibers.
The inner shell forms longitudinal folds throughout its entire length, which protect its integrity when stretched. Muscle fibers grow into the mucous layer. They allow you to close the lumen from the reverse flow of urine from the bladder.
The muscle layer is formed by bundles of cells running in the longitudinal, oblique and transverse directions. The thickness of muscle cells varies. The upper part includes two muscle layers:
- longitudinal;
- circular.
The lower part is reinforced with three layers:
- 2 longitudinal (internal and external);
- the average between them is circular.
Antegrade stenting
The antegrade method of stenting the kidney involves introducing the stent not from the bladder, but percutaneously. A puncture of the skin and underlying tissues is performed, then the kidneys, and urine is drained not through the bladder, but into an external reservoir.
This manipulation is indicated in cases where:
- Retrograde stenting failed;
- The bladder has been previously removed or is of insufficient size (microcystis);
- There is a strong narrowing of the urethra, making it impossible to insert instruments and a catheter into it;
- The cystoscope fails to localize the ureteral orifice;
- There are wall defects in the ureters.
If antegrade stenting is performed correctly, it provides adequate urine flow and access to the upper urinary tract, but a serious drawback of the procedure is the need to wear an external urine reservoir. For those patients in whom retrograde stenting could not be performed, and for some reason it is better not to use percutaneous stenting, a combined procedure is performed, when the bladder is entered antegradely, and then a stent is inserted retrogradely from there.
Antegrade, or percutaneous, stenting involves the introduction of a stent after kidney puncture, and it is better to divide the manipulation into two stages - kidney puncture (nephrostopia) and stenting a week later. This approach minimizes the risk of bleeding, stent thrombosis, or nephrostomy displacement.
Antegrade nephrostomy is performed under x-ray control in several stages:
- Treatment of the skin in the lumbar region, puncture of the kidney and providing access to the lower or middle renal calyx (nephrostomy);
- Injection of contrast into the calyces, pelvis, ureter, installation of a conductor;
- Implantation of JJ stent and removal of nephrostomy.
Blood supply
The tissues of the ureter receive nutrition from arterial blood. The vessels lie in the adventitial (outer) membrane and accompany it along its entire length, penetrating deep into the wall with small capillaries. Arterial branches arise in the upper part from the ovarian artery in women and the testicular artery in men, as well as from the renal artery.
The middle third receives blood from the abdominal aorta, internal and common iliac arteries. In the lower section - from the branches of the internal iliac artery (uterine, vesical, umbilical, rectal branches). The vascular bundle in the abdominal part passes in front of the ureter, and in the small pelvis - behind it.
Venous blood flow is formed by veins of the same name, located parallel to the arteries. From the lower section, blood flows through them into the branches of the internal iliac vein, and from the upper section into the ovarian (testicular) vein.
Lymph drainage goes through its own vessels to the internal iliac and lumbar lymph nodes.
Endoscopic method
The endoscopic treatment option is an alternative to procedures to get rid of existing stones. In this case, a transurethral endoscope is inserted into the urethral opening. The kidney can also be punctured using an endoscope. The stages of the intervention are similar to abdominal surgery. It is performed under general anesthesia.
But the difference between this treatment is a shorter adaptation period; recovery is quick and relatively without complications. In some situations, this method is the only possible option for getting rid of stones.
Reduction mechanism
The main task of the ureters is to push urine from the pelvis to the bladder. This function is provided by the autonomous contractility of muscle cells. In the ureteropelvic segment there is a pacemaker (pacemaker), which sets the required rate of contractions. The rhythm may vary depending on:
- horizontal or vertical body position;
- rates of filtration and urine formation;
- “indications” of nerve endings;
- condition and readiness of the bladder and urethra.
The direct effect of calcium ions on the contractile function of the ureters has been proven. The strength of contractions depends on the concentration in the smooth muscle cells of the muscle layer. A pressure is created inside the ureter that exceeds that in the pelvis and bladder. In the upper section it is equal to 40 cm of water. Art., closer to the bladder – reaches 60.
This pressure is capable of “pumping” urine at a rate of 10 ml per minute. The common innervation of the ureter with the adjacent part of the bladder creates conditions for coordinating the muscular efforts of these organs. The pressure in the bladder “adjusts” to the ureteral pressure, so under normal conditions the reverse reflux of urine (vesicoureteral reflux) is prevented.
Symptoms
Due to overstretching of the renal capsule, intense pain occurs. At the initial stage, these pains are constant, but tolerable. Complete obstruction mimics all symptoms resembling renal colic. If immediate measures are not taken, stagnation of urine provokes the formation of stones. If such complaints arise, you should immediately contact a specialist.
Diagnosis of this pathology is carried out on the basis of excretory urography. This method allows you to see the ability of the kidneys to excrete using a contrast agent.
Treatment of this pathology is carried out using a cystoscope, which allows you to restore the patency of the urinary tube. If this method fails, then surgical treatment is resorted to. In this case, the urinary tube is opened, the valve is removed, and the surgical wound is sutured layer by layer. If it is not possible to perform an operation, then resort to puncture of the pelvis. Under the control of an ultrasound machine, a catheter is inserted into the pelvis, thus allowing the outflow of urine.
If the pathology is identified in time, urosepsis is prevented, and treatment is carried out, then this pathology can be cured. The prognosis for recovery is always favorable.
Patients who are faced with problems of the urinary system have a number of questions about the disease. They want to know all aspects: from the features of their pathology to the variants of the norm. Let's consider the structure of the ureter and bladder, their functions and sizes.
Structural features in childhood
In a newborn baby, the length of the ureter is 5-7 cm. It has a convoluted shape in the form of “knees”. Only at the age of four does the length grow to 15 cm. The intravesical part also gradually grows from 4-6 mm in infants to 10-13 mm by the age of 12.
The muscle layer in the wall is poorly developed. Elasticity is reduced due to thin collagen fibers. However, the contraction mechanism provides a fairly large evacuation of urine, the rhythm of contractions is constantly frequent.
Congenital malformations are considered:
- atresia - complete absence of the ureteric tube or outlet;
- megaloureter – pronounced expansion of the diameter along the entire length;
- ectopia - disturbed location or connection of the ureter, includes communication with the intestines, entry into the urethra, bypassing the bladder, connection with the internal and external genitalia.
Questions
Question: How much urine does the bladder hold and hold?
Answer: According to some reports, up to 1-1.5 liters, but the capacity of the bladder is an individual indicator.
Question: How many ureters are normal?
Answer: A healthy person has two ureters - one from each kidney. With developmental anomalies, there are double or triple ureters or the absence of a ureter on one side.
Question: What is the diameter of the ureter in mm and how long is it?
Answer: The average diameter of the ureter in a healthy person is within 5-6 mm, the length depends on gender and individual structure, on average it is 200-300 mm.
The ureters are paired organs that connect the renal pelvis to the bladder. The diameter of the ureter depends on the location of the latter. This organ serves as a kind of connecting link of the urinary system: urine flows through it from the kidneys to the bladder, from where it will be released from the body to the outside.
Methods for studying the structure of the ureter
To identify pathology, methods are needed that reveal the characteristic picture of the lesion. For this use:
- clarification of medical history, complaints;
- palpation of the abdomen;
- X-ray examinations;
- instrumental techniques.
Most often, pathology of the ureters is accompanied by symptoms of pain. Typical for them:
- character – constant aching or paroxysmal colic;
- irradiation - to the lower back, lower abdomen, groin and external genitalia, and in children to the navel area.
By distribution one can judge the localization of the pathological process:
- if the disorders lie in the upper third of the ureter, then the pain goes to the iliac region (in the hypochondrium);
- from the middle section - to the groin;
- from the lower third - into the external genitalia.
By palpation, an experienced doctor will determine muscle tension in the anterior abdominal wall along the ureter. For more detailed palpation of the lower section, a bimanual approach (two-handed) is used. One hand with two fingers is inserted into the rectum, vagina in women, the other makes counter movements.
In a laboratory urine test, many leukocytes and red blood cells are found, which may indicate a lesion in the lower urinary tract.
Cystoscopy - by inserting a cystoscope through the urethra into the bladder, you can examine the openings (orifices) of the ureters from the inside. What matters is the shape, location, release of blood and pus.
Using chromocystoscopy with preliminary injection of a dye into the vein, the rate of release from each opening is compared. Thus, one can suspect the presence of a unilateral blockage (stone, pus, tumor, blood clot).
Catheterization of the ureter is carried out with a thin catheter through the hole in the bladder to the level of detection of the obstacle. A similar approach to retrograde ureteropyelography allows you to check the x-ray anatomy of the ureters, the presence of patency of bottlenecks, and tortuosity.
A survey urogram does not show the ureters, but in the case of an existing stone (shadow of stones), its localization can be suspected.
The most indicative is excretory urography. A series of images after intravenous administration of contrast allows us to trace the course of the ureters and identify pathology. The shadow has the appearance of a narrow ribbon with clear, smooth boundaries. The radiologist determines the location in relation to the vertebrae. In the pelvic cavity, 2 bends are observed: first to the side, then on the approach to the bladder to the center.
Urotomography is performed when doubts arise about the significance of lesions from neighboring organs and tissues. Layer-by-layer images allow them to be separated from the ureter.
Motor skills are studied using lessonography. The method allows you to identify decreased or increased tone of the wall muscles. Modern devices make it possible to see on the screen the contraction of different parts of the ureter and to study the electrical activity of cells.
Knowledge of the structure and location of the ureters is necessary for diagnosing diseases of the urinary system, comparative pathology accompanied by urinary retention. Each surgical intervention in operative urology needs to take into account anatomical, age-related features, and the approach of the neurovascular bundles. In medical language they are called topography.
2pochki.com
Structure, location and functions of the bladder
The bladder is an organ for the accumulation and temporary storage of urine, which is excreted at regular intervals through the urethra. Its main role is to store and release urine into the urethra.
Its volume ranges from 500-800 ml and varies depending on the individual characteristics of the person.
The shape and position in relation to other organs and tissues depend on the degree of its fullness with urine and the gender of the patient.
- Location in women. When the bladder is empty, in women it lies in the pelvic cavity. It is separated from the rectum by the vagina and uterus. When filled with urine, it changes shape and, in cases of severe stretching, reaches the level of the navel. The wide part (bottom) is directed towards the vagina, and the narrow part goes into the urethra. The anterior surface of the uterus is adjacent to the anterior surface in women.
- Location in men. An empty bladder is found in the pelvic cavity; in men, it is separated from the rectum by the seminal vesicles and a section of the vas deferens. The bottom or wide part of the bladder in men faces the rectum. The lower part is fused with the prostate gland, and the upper part remains mobile. In men, intestinal loops are adjacent to the upper surface.
- Location in newborns. The ureter is different in newborns. In newborn children, the bladder is located much higher than in an adult. Immediately after birth, it begins to gradually descend downwards, and by six months of the child’s life it is determined at the level of the upper edge of the fusion of the pubic bones.
Internal structure and blood supply
The bladder consists of three layers: muscular, mucous and serous.
The muscle layer includes three types of fibers that stretch and contract as needed. Where the bladder passes into the urethra, the muscle layer forms a sphincter (sphincter), which contracts involuntarily (regardless of the patient’s wishes).
The mucous membrane is pink and covered with folds. It contains small mucous glands and lymphatic follicles.
This organ is supplied with blood from the superior and inferior cystic arteries, which belong to the basin of the large iliac arteries. Lymph flows to nearby inguinal lymph nodes.
Every few minutes, the openings of the ureters involuntarily open into the cavity of the bladder and throw out a small amount of urine. Having reached a certain position and size, it performs its functions and expels urine into the urethra, from where it is discharged.
Possible anomalies
Common developmental anomalies include:
- diverticulum It is a bag-like protrusion of the wall. There are single and multiple options. Urine stagnates in such diverticula, which contributes to the development of cystitis;
- non-closure and fistulas of the duct, which connects the bladder through the umbilical cord with amniotic fluid during intrauterine development;
- its absence or underdevelopment is rare. A vice incompatible with life;
- doubling. In the cavity of the bladder there is a septum that divides it into two parts; it prevents the bladder from fully performing its functions. Treatment is surgical.
Features of the structure of the ureters
Thanks to the anatomy of the genitourinary system, it is possible to trace the muscle layer in the ureters, which contributes to the normal movement of urine to the bladder. This layer also serves as protection against the reverse process. The inner part of the ureters is lined with epithelium; on the outside, a sheath of fascia is visible.
Where the depression is visible, smooth muscle fibers can be seen in large quantities. When they contract, they prevent the outflow of urine into the kidney organs in the opposite way.
According to their structure, the ureters are characterized by three narrowings:
- Transition of the pelvis to the ureter;
- the middle third, that is, the place that smoothly passes into the small pelvis;
- the third narrowing is the mouth.
Stone formations tend to get stuck in these parts. It is worth describing each narrowing in more detail and characterizing each one.
- This segment is also called the ureteropelvic segment. If the stone is more than two centimeters in diameter, there is a high probability that it will get stuck in this very place.
- The area when crossed becomes narrower to 4 mm.
- This segment is called the vesicoureteral segment. Its diameter becomes narrower to 1-5 mm. Most stones get stuck in this narrow area.
The place where stones form is called the renal pelvis. This is where they get stuck. They occur with the same frequency of formation in both the left and right sides of the ureter.
Most often, ureteral stones form in the kidney area. Accordingly, their composition is identical. The most common stones are composed of calcium oxalates.
Diseases of the ureter and approaches to their treatment
There are congenital and acquired pathologies of the ureters. Congenital diseases occur under the influence of damaging factors on the fetus.
Hypoplasia often occurs when the corresponding kidney is underdeveloped. The diameter of the ureter decreases and in some places it can become obliterated. A narrowing, or stenosis, most often forms in the vesicoureteral segment. In these cases, surgical treatment of the ureter with plastic surgery of the affected segment is possible.
Ureteral valves are a doubling of the inner lining of the organ in the form of a fold; they are quite rare.
Congenital atony is one of the most severe pathologies. Due to the lack of contractions, the ureter expands greatly. Clinically, this may not manifest itself in any way, but persistent pyuria is detected in the urine.
Acquired diseases are mainly the result of obstruction. This may be a consequence of external compression or the presence of an obstruction in the lumen.
From the outside, compression is most often caused by prolonged constipation, kinks of the ureter, gynecological pathology, cancer of the bladder, prostate, and cervix.
With urolithiasis, small stones from the renal pelvis can enter the ureter, disrupting the outflow of urine. The surgical operation ureterolithotomy is performed to remove stones from the ureter if other methods have been ineffective.
In addition to stones, organ obstruction can be caused by a cancerous tumor or a chronic inflammatory process (for example, tuberculosis, schistosomiasis). Treatment of ureters will consist of removing the obstruction or surgically removing the ureter and draining the renal pelvis.
With fibrous lesions in the area of retroperitoneal tissue, fibrous polyureteritis occurs. In this case, the ureter is covered from the outside by fibrous tissue in the form of a coupling, which compresses it from the outside. This pathology can also only be corrected surgically.
Factors for stone passage
When planning an effective course of treatment, it is worth considering two main factors: the size and location of the stones. If the size of the stone does not exceed 4 mm, almost always (90% of cases), surgical intervention will not be required; the formations will leave the body on their own. If the stone diameter reaches 9 mm, then such successful predictions are reduced to 50%. There is practically no chance of independent exit from the proximal part. This is where surgery will most often be needed.
Experts identify a characteristic term that sounds like “stone path.” Its significance lies in the collection of fragments of stones that formed over time, perhaps got stuck, or provoked the development of ureteral obstruction in men.
Types of operations to remove stones
In medical practice, there are various types of operations to remove stones from the ureter:
- Remote and contact lithotripsy.
- Ureterolithoextraction.
- Nephrolithotomy
- Endoscopic ureterolithotomy.
- Surgical abdominal operation.
There are different types of operations to remove stones from the ureter
Only a doctor can select a specific procedure for stone removal based on the research performed.
Diagnostics
The urethra (urethra) is an important ally in the diagnosis of this manifestation. In this case, the data obtained after palpation, as well as additional measures, are taken into account.
Stones in the ureter in men are diagnosed by palpation in the part of the urethra that hangs, in the perineal part. Rectal examination is necessary in cases where stones are located in the posterior compartments.
Ultrasound of the bladder is used, which makes it possible to detect an acoustic shadow in the urethra. A urine test is required, which will help in determining the inflammatory process.
Another method is to insert a metal bougie into the urethra. There may be a feeling of obstruction or slight friction.
To diagnose the differential type, urography and urethroscopy are used.
Functions in the human body
The urinary ducts perform the function of transporting urine from the renal collecting system to the urinary tract. The paired organ has motor function. Its middle layer, the smooth muscle layer, stimulates the wave-like contraction of the canal. Peristalsis is provided by a pacemaker (pacemaker), which is located in the pelvis zone of the duct.
The rhythm frequency and cyclicity of contractions depend on several factors:
- volume of urine excreted by the kidneys;
- human physical activity;
- presence of pathologies;
- body position;
- correct functioning of the nervous system.
The urge to contract the walls occurs when a sufficient amount of calcium accumulates in the muscle layer.
Stones in the prostate (prostate gland)
According to statistical studies, about 40% of men experience this disease from 8 to 10 years from diagnosis of the disease. The cause of this disease is the chronic nature of prostate diseases. This process is accompanied by stagnant manifestations in the prostatic secretion. In addition, with constant overwork, stressful situations, hypothermia and the presence of addictions, stones begin to form in this place over time in men. In addition, violation of personal hygiene rules, an inactive lifestyle and irregular sex life are identified. It is also important to minimize the occurrence of formations to undergo examinations for the presence of inflammatory diseases in the urinary system.
Diseases
Based on the symptoms, certain categories of ureteral disease can be distinguished, including:
- Congenital type (dilation, ureteral hypoplasia, ureterocele).
- Inflammatory (ureteritis).
- Obstructive (obstruction).
- Tumor nature (fibroepithelial polyp, various tumors).
- Traumatic (rupture of the ureter).
The size of the ureter is an imprecise value, since not only the difference in the structure of the body of each individual individual plays a role here, but also differences in diameter as the organ moves forward.
You can also learn about the ureter from this video.
Action tactics
First of all, it is necessary to clearly know the size of the stone and its location. If the diameter of the formations does not exceed five mm, do not worry, they will come out on their own. The doctor may prescribe an increase in the volume of fluid you drink per day, in particular pure water. Analgesics are prescribed.
It is necessary to carry out review procedures and urograms every two weeks, which show the dynamic development of stone movements. The patient needs to filter the urine to preserve the analysis for stones. Individually, the patient should monitor himself for the presence or absence of the following symptoms:
- Fever;
- infectious diseases in the urinary system;
- strong, sharp pain;
- uncontrolled attacks of vomiting, severe feeling of nausea.
Methods for removing stones
To remove stones, 2 areas of treatment are used, depending on the complexity of the situation and the size of the formations, namely:
- Conservative expectant therapy.
- Active.
The first direction is used in the presence of stones with a diameter of 2-3 mm that do not block the ducts. Such stones can come out on their own, so medications such as:
- "Nifedipine" or "Tamsulosin" - to speed up the passage of stones.
- “No-shpa”, “Drotaverine” - to ease spasms.
- Ibuprofen - to relieve pain and inflammation.
You can use traditional medicine and drink diuretic decoctions, which include herbs such as horsetail, dill and corn silk.
This therapy involves attending physiotherapy and exercise therapy, as well as following a special diet that limits the consumption of foods with oxalic acid (cabbage, spinach, nuts, currants and legumes).
In the presence of large stones, active therapy is used, using a method such as lithotripsy (removal of stones by crushing). It comes in the following types: remote, contact, pneumatic, laser, ultrasound and percutaneous.
In the most severe cases, surgical intervention is necessary.
Treatment
If an infectious disease begins to develop against the background of formations, then it is necessary to begin a course of treatment as soon as possible. In cases where there are no discomfort, pronounced pain, or infections, then the doctor prescribes treatment depending on how the patient feels. If complete obstruction is observed, then the kidney is damaged within 24 hours. In a period of up to two weeks, changes in the kidney organs are irreversible. It is recommended to seek help from specialists as early as possible, undergo high-quality diagnostics and decide on a course of treatment.
Symptoms and examinations
Typically, the examination of patients begins with an examination of their complaints. Most often, patients complain of pain. In this case, the pain can be different - aching, stabbing, paroxysmal, often radiating to the lower abdomen. Sometimes urination problems occur. Pain is also noted on palpation. Changes in urine analysis are also usually noticeable. Studies such as cystoscopy to examine the orifice of the ureters, chromocystoscopy to determine the blockage of urine movement, catheterization, and urography are often performed. During urography, the ureters themselves are usually not noticeable, but radiopaque stones in them can be seen. Sometimes excretory urography, x-ray cinematography, and electroureterography are used. Timely contact with a urologist and properly performed examinations often help to avoid the worst - removal of the ureter.
Clinical picture
The main symptom of the disease is severe pain, which intensifies with physical exertion and fast walking. The attack can last from two to twenty-four hours. If a stone is stuck in the ureter, a symptom such as frequent urge to urinate appears, and when it does not come out, the consequence is problems with urination. In addition, the disease is often accompanied by other manifestations:
- abdominal pain radiating to the lower back,
- headache,
- nausea and vomiting,
- bloating,
- mucus and blood in urine,
- fever, high temperature.
If the stone comes out, relief comes and the pain disappears. But it happens that it gets stuck in one place, injuring the mucous membrane, which causes new symptoms and serious complications. If you suspect urolithiasis, it is impossible to empty the bladder and there is severe pain, you should immediately call a medical team and do not try to solve the problem on your own. Before the specialists arrive, you can take No-shpa and a painkiller.
Sand and small salt crystals are able to come out without outside intervention, without causing any pain. If there is a large stone of 8 mm or more in the ureter, you need to know how to remove it at home. To do this, you will have to take specialized medications that crush the stones and ensure their removal from the body.
Diet after surgery
In connection with the development of modern medicine, surgical intervention in its classical manifestation has lost its meaning and, accordingly, popularity. Removing a stone from the ureter endoscopically is now much easier than performing abdominal surgical manipulation.
Kidney surgery also requires large incisions to achieve the optimal width of the surgical field, which results in the formation of a large postoperative scar.
Each of them is different and they are carried out differently.
Moving Stones
Ureters
When a stone enters the ureter, it begins to gradually move towards the bladder. The diameter of the stone is 3–15 mm. The uneven shape contributes to retention in certain areas of the urinary canal, which leads to blockage.
With small sizes (up to 0.5 mm), it can be removed independently. If the stone is large, you cannot do without surgery. If there is a stone in the ureter, the specialist must determine the optimal method of surgery.
Ways to get rid of stones:
- lithotripsy (remote and contact);
- surgical intervention to open the ureter.
Any of these methods requires additional drug treatment. The patient takes painkillers, antispasmodic medications, is treated with diuretics and restores water balance.
The urinary tract can become infected when stones move, so the patient is prescribed mandatory antibiotics. The supervising doctor determines which pills to take.
In some cases, in the presence of particularly large stones in the urinary canal, surgical opening is resorted to. An operation is performed to remove stones under general anesthesia; an incision is made below the ribs, about 10 cm in size. The doctor performs manipulations through the hole.
DETAILS: Erotic urological massage for men
The urinary canal is opened, a stone is removed from it, after which the tubular organ is sutured. The operation is quite complex, the outcome directly depends on the experience and professional training of the surgeon. Before opening the ureter, the patient must undergo a set of diagnostic tests:
- general analysis (blood, urine);
- glucose level;
- determination of platelet concentration in the blood.
Given the need for deep anesthesia, an examination by an anesthesiologist will be required. It is also necessary to find out whether the patient has an individual intolerance to any drugs. The patient’s lifestyle, addiction to alcohol or drugs is clarified.
Rehabilitation lasts 14–21 days, recovery after lithotripsy takes 3 days.
After the operation, the patient will need to adhere to the following principles of rehabilitation:
- control of the amount of fluid consumed (its volume should be at least 2 liters per day);
- use of medications that stimulate diuresis;
- compliance with postoperative dietary nutrition;
- use of diuretics;
- compliance with bed rest in the first days after surgery;
- stopping drinking alcohol.
Tea and coffee are contraindicated for urate stones.
After surgery, specialists prescribe the patient a special diet, which is compiled based on the individual characteristics of the patient and the type of stones in the ureter. Dietary nutrition is aimed at regulating urine output and preventing the appearance of new stones.
- Urate. They are formed due to an increased concentration of purine substances and uric acid salts. These substances are found in liver, legumes, cabbage, tea and coffee.
- Phosphate. Appear in cases of failures in phosphate-potassium metabolism, due to which the acidic environment of urine becomes alkaline. Calcium and phosphate are found in abundance in seeds, dairy products, nuts and fish.
- Oxalate. They develop due to the high accumulation of oxalic acid contained in spinach, sorrel, zucchini, tomatoes, lemons, gooseberries and oranges.
To prevent lithotripsy from causing dangerous consequences, you should follow the recommendations of doctors. They relate to both preparation for the intervention and the postoperative period.
Before the operation, the following is done:
- Initially, a full examination is carried out. All tests are taken, a urine culture is done, and a cardiogram is reviewed. In addition, an X-ray examination of the kidneys, ureter and other organs is carried out;
- The decision on which method to use is made by the urologist. He bases his opinion on all the analyzes and examinations performed;
- seven days before the scheduled operation, the patient must stop taking medications that contain acetylsalicylic acid;
- the day before surgery, the patient should not eat. Only drinking is allowed.
Do not think that removing stones from the ureter is a complete solution to the problem. Such an intervention only removes the pain component. Conglomerates may form again and return to the ureter. Therefore, treatment with medications must be continued, following all the doctor’s recommendations.
After extraction, the stones are sent to the laboratory. Here they undergo research to determine their composition. Knowing this, it is possible to identify the reason for their formation. Depending on the composition of the conglomerates, a specific diet is prescribed.
To choose the optimal method for removing kidney stones, you need to find out their type and size. Then the following solutions to the problem are proposed:
- dissolution of stones with medications;
- crushing stones to smaller sizes without surgery;
- operation.
In some cases, drug therapy does not contribute to the dissolution of salt residues. Phosphate and oxalate deposits are practically impossible to change due to their composition.
If these methods are unsuccessful, the patient is offered surgical intervention.
Surgical removal of kidney stones is indicated if:
- It is not possible to relieve pain with medications.
- Kidney failure is increasing.
- Ureteral obstruction was detected.
- Purulent inflammation develops.
- Kidney carbuncle was diagnosed.
- The patient expresses a desire to undergo surgery.
In case of serious complications of the disease that threaten the patient's life, urgent surgical intervention is indicated.
Medications prescribed in the postoperative period normalize blood circulation in the organ and tissues located near it. During antibiotic therapy, it is also recommended to take medications that prevent disruption of the microflora in the intestines.
Special care is required for patients with a catheter installed. Particular attention is required to maintain drainage in an appropriate condition to prevent infection.
Patients are prescribed a special diet. The nutrition recommended by experts is balanced to restore kidney function and partially relieve the urinary system during the rehabilitation period.
The diet for the first two days includes liquid foods - low-fat broths, jelly, non-concentrated juices. Food is taken frequently - seven or eight times a day.
On the second and third days, the diet is expanded by adding ground food. You can eat boiled food. It is recommended to eat five to six meals once a day.
Starting from the fifth day, you are allowed to return to your normal diet, but exclude fatty and fried foods. The number of meals per day is at least four to five times.
After determining the composition of the stones, the doctor gives further recommendations regarding nutrition.
Features of stenting with metal stents
Restoring the patency of the ureter and urine outflow is possible with metal self-expanding stents, which represent a good alternative to soft stents and nephrostomy if the patient’s urinary tract is closed by a tumor or has scar adhesions, as well as if there are contraindications to surgical interventions.
The insertion of a metal stent is carried out under X-ray control using a special cannula and guidewire, which help guide the end of the stent behind the narrowed fragment of the ureter. After implantation, the metal stent expands and allows urine to flow out.