Types of daily urine output tests
Why is it necessary to study daytime diuresis and nighttime diuresis? What does it give? Urine is tested to calculate the concentrations of certain substances in the body:
- Protein (called daily proteinuria analysis). The loss of protein is not taken into account, but its increase should be considered a sign of life-threatening diseases.
- Collecting test material for sugar is often prescribed to patients with diabetes.
- Control of oxalate content is carried out in diseases of the gastrointestinal tract.
- Urine is checked for the presence of cortisol inclusions in it. If they are elevated, then we can talk about the presence of Itsenko-Cushing syndrome.
- Metanephrines (called analysis: urine for salturesis). Donation is necessary if a benign tumor is suspected, which progresses slowly and does not have obvious manifestations.
When and to whom is it done?
If you have diabetes, it is mandatory to take a urine sample to determine kidney disease.
It is necessary to submit urine for daily analysis when checking the functioning of the kidneys, to control the substances released during the day. A daily urine test is required if:
- diabetes mellitus, then 24-hour urine analysis will help control the patient’s glucose level;
- kidney diseases (when water balance is disturbed, diuresis outflow or failures occur in the performance of their functions);
- pregnancy, then a daily urine test helps determine how a woman’s body copes with stress.
Proportion of daytime and nighttime diuresis
The volume of urine excreted during the day and night can be defined as 3:1 or 4:1. This proportion is considered normal.
Violation of the proportion towards an increase in nocturnal diuresis is called “nocturia”. This condition is accompanied by a disruption in the process of blood flow to the kidneys. Most often, diabetics, people with diagnosed glomurelonephritis, pyelonephritis and nephrosclerosis get up to go to the toilet at night.
The Zimnitsky test is an algorithm for measuring diuresis that helps calculate indicators of kidney activity. The patient collects urine into different containers every three hours throughout the day. Urine collected from 6 to 6 o'clock is called daytime diuresis, and urine collected from 18 to 6 o'clock is called night diuresis.
During the analysis, the laboratory technician will calculate the density of urine. A healthy body is able to secrete 40-300 ml of biological fluid at a time. Along with the Zimnitsky test, the doctor often prescribes a general urine test to clarify other important indicators.
Preparation: how not to distort the results
No special training is required to collect urine. The collection rules will be explained by a medical professional, focusing the patient’s attention on the fact that urine collection requires care and correct actions. There are several requirements that the analysis takes into account:
- It is necessary to maintain an acceptable drinking regime so that the level of water balance is normal.
- The use of diuretics and certain medications (for example, aspirin) is prohibited.
- It is not recommended to eat beets, carrots and other natural dyes that affect the color of urine for analysis.
- Alcoholic beverages are prohibited.
- For women, urine collection for daily diuresis during menstruation is contraindicated.
- It is not recommended to have sexual intercourse 12 hours before collecting material.
Why does a doctor need to know the patient's hourly urine output?
In severely ill patients who are unable to void on their own, hourly urine output is measured using a urinary catheter. The volume of urine excreted per hour allows you to monitor the patient’s condition in a coma. The normal amount of urine is 30-50 ml every hour. If this indicator is less than 15 ml, this may indicate that the intensity of infusions should be increased. If blood pressure is normal with a simultaneous decrease in diuresis, the doctor makes an intravenous injection of Salnikov's drug, which stimulates urination.
Normal values for daily diuresis are relative and vague, as they depend on a combination of various factors, including the patient’s drinking regimen, his weight, gender, age, diet and medications. Therefore, the daily urine rate in women and men can be approximately the same, regardless of gender.
How to collect from children and adults: collection rules
To ensure the accuracy of the analysis, urine must be collected following the collection rules.
How to properly collect urine for analysis? The research will be correct if you adhere to the following actions:
- to check daily diuresis in children and adults, urine is collected in a sterile container with divisions to calculate the volume;
- for collection, it is necessary to wash the external genitalia so that unnecessary substances do not get out of them;
- collection of daily urine begins without the first portion; determination of daily urine output does not require its infusion;
- Urine should be stored in the refrigerator;
- the entire container is not needed in the laboratory, you can estimate at home how much the daily norm is;
- from the total mass, up to 200 ml are poured, which are delivered to the laboratory, indicate the time (no hourly clarification is required), from when and at what time the urine was collected and the total volume (determine it yourself), how old the patient is;
- sometimes you need an indicator such as weight, sometimes height is also measured.
Performance standards: within what limits are they assessed?
In the table for assessing urine per day, the state of water balance and calculating daily diuresis, laboratory assistants can find all the standard values. The correct results are recorded on a special sheet and sent to the doctor for subsequent diagnosis or the appointment of additional diagnostic examination methods. The algorithm of actions for assessment includes the following basic indicators, the value of which determines the conclusion:
- total volume of urine excreted per day: the normal change in daily diuresis for an adult man is 1-2 liters, for women - 1-1.6, the normal daily diuresis for children is no more than 1 liter;
- rate of diuresis (hourly control);
- color, transparency, density (normally, in adults and children, urine should be without turbidity);
- in a healthy person, hemoglobin should be absent in a urine test per day;
- measurement of glucose when submitting material for sugar (norm - 1.6 mmol/day);
- creatinine count (if it is elevated, this indicates acute infections, hypothyroidism, etc.), the value of which should fluctuate between 5.3-16 mmol/day. for females and 7−18 for males;
- pH is a characteristic whose change affects the pH of the blood;
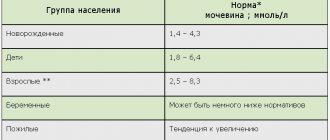
- measuring urea levels (the normal value for all categories of the population is 250-570 mmol, deviations are a signal of disease);
- measure oxalates, the normal value of which ranges from 228−626 µmol/day;
- check for the presence of protein (daily proteinuria): acceptable excretion is 0.08-0.24 g/day;
- daily urine is checked for bilirubin, which indicates blood or liver diseases;
- human diuresis is examined for the presence of urobilinogen (no more than 10 µmol).
Daily diuresis is one of the criteria for proper kidney function. Urine excreted per day is usually counted. Normally, in an adult, the amount of urine excreted is ¾ or 70-80% of the fluid consumed. In this case, the amount of moisture that enters the body along with food is not taken into account. Therefore, if a person should drink about two liters of liquid per day, then the volume of urine excreted is at least 1500 ml.
In order to completely remove decay products from the body, at least half a liter of urine must be released. Determining daily diuresis is also important for studying renal function by calculating clearance. To do this, the patient must collect all urine during the day into a special container with graduated walls.
However, he should not take diuretics during the procedure and three days before it. It is also important to record not only the volume of urine excreted, but also the volume of liquid drunk (water, tea, coffee). Measuring daily diuresis usually begins from 6 a.m. to the same time the next day.
Preventive measures
Prevention is the key to bladder health. Doctors point out the following as preventive measures:
- Normalization of diet.
- Reduce consumption of foods that cause increased urine production.
- Control of daily urine volume (normally it is 1.5-2 liters).
- Refusal of alcoholic drinks.
- Refusal of various products with artificial colors.
- Timely contact a doctor if signs of illness appear.
- Periodic medical examination 2 times a year.
By following simple rules, you can not only reduce the risk of the disease, but also eliminate it altogether.
An important issue is nutrition during illness. To relieve your bladder, you should exclude the following foods from your diet:
- alcohol;
- spices;
- chocolate;
- carbonated drinks with dyes.
Knowing what polyuria is, you can not only find out the cause of the disease, but also cope with the disease painlessly and in the shortest possible time. To do this, it is enough to visit the doctor on time, and then adhere to his instructions.
Types of diuresis
Depending on the amount of urine excreted, there are:
- polyuria – the amount of fluid excreted exceeds 3 liters. This may be due to disruption of the hormone vasopressin, also called antidiuretic hormone. Sometimes this condition occurs when the concentrating ability of the kidneys is impaired, with diabetes mellitus;
- oliguria – the amount of fluid secreted has sharply decreased to 500 ml or less;
- anuria, in which urine output in an adult does not exceed 50 ml in the entire 24 hours.
Urine flow occurs unevenly throughout the day. Therefore, daytime and nighttime diuresis are distinguished, the ratio of which is normally 4:1 or 3:1. If nocturnal diuresis prevails over daytime diuresis, then this condition is called nocturia.
It is also important for patients to evaluate not only the amount of fluid secreted, but also its composition. If the concentration of osmotically active substances in the urine exceeds the norm, then such diuresis is called osmotic. This condition indicates an overload of nephrons with substances such as glucose, uric acid, bicarbonate and others. Their increase in the blood is associated with other organic pathology.
The daily amount of urine with a reduced concentration of osmotically active substances is called water diuresis. In a healthy person, this condition can be observed with an increase in fluid intake.
Polyuria in diabetes
Diabetes is an endocrine disease, the causes and pathogenesis of which are different. There are sugar and non-sugar types of pathology. Diabetes mellitus is of types 1 and 2:
Diabetes mellitus type I
Characterized by absolute insulin deficiency, it is a hereditary disease, therefore it manifests itself at an early age of 3-20 years. The first symptoms of the disease are polyuria, polydipsia, acidosis, and sudden weight loss. A laboratory test will reveal glucose and ketone bodies in the urine. People with this pathology need to keep a constant record of carbohydrates consumed and, depending on their quantity, independently inject insulin.
The disease reduces the quality of life, but with a responsible attitude towards one’s disease, the level of modern medicine allows people to lead a normal lifestyle. The life expectancy of such patients is not inferior to the average life expectancy in the population.
Diabetes mellitus type II
Acquired disease with hereditary predisposition. It is detected for the first time in adults aged 45 to 50 years. Risk factors for the disease are controllable, so the disease can be prevented. It is necessary to control body weight, consumption of carbohydrates, alcohol and avoid bad habits. Polyuria may also be the first symptom, although patients may not pay attention to it.
Diabetes insipidus
Glucose levels do not play a role in diabetes insipidus. It all depends on the antidiuretic hormone, the synthesis of which can be disrupted under various circumstances: head injury, encephalitis, heredity, medications, Sheehan syndrome, brain tumors. In the absence of the hormone, daily diuresis can reach 20 liters when the norm is 1.5 liters.
The mechanism of polyuria in both types of diabetes is the same. There is an increase in blood glucose levels, which leads to decreased reabsorption and increased excretion of glucose in the urine. Water is excreted along with glucose. Clinically, this is manifested by an increase in the volume of urine excreted.
mypochka.ru
Decreased urine output
A decrease in the daily amount of urine in a healthy person can be observed during the hot season, when most of the liquid is excreted through sweat. This condition also occurs when working in high temperatures, loose stools or vomiting.
But a decrease in urination to 500 ml per day or less is a poor prognostic sign for many diseases. The development of oliguria or anuria occurs with a sharp decrease in circulating blood volume and a drop in blood pressure. They develop with heavy bleeding, uncontrollable vomiting, profuse loose stools, and various states of shock.
Oliguria occurs with the development of acute renal failure. This life-threatening complication occurs with nephritis, acute massive hemolysis, and damage to the renal parenchyma. With a massive infectious process, kidney damage is possible due to bacteremia.
Differential diagnosis of oliguria must be carried out with ischuria. This condition develops due to mechanical blockage of any part of the urinary system. This can be caused by the growth of a tumor process, blockage of the lumen of the ureter with a stone, or narrowing of the urinary tract. In men, a common cause of ischuria is prostate adenoma, especially in older people.
Increased urine output
Polyuria is an important diagnostic criterion for a number of endocrine, cardiac or metabolic diseases.
There are renal and extrarenal polyuria. The first is caused directly by kidney disease, which affects the distal parts of the nephron. This symptom can occur with pyelonephritis and renal failure.
There are many more reasons for the development of extrarenal polyuria. Increased urine production occurs in diabetes mellitus. This occurs when glucose enters the urine, which draws fluid onto itself, since it is an osmotically active substance.
In diabetes insipidus, the genesis of polyuria is a violation of the production of vasopressin, which is responsible for retaining the required amount of fluid. Daily diuresis also increases with Conn's syndrome (hyperaldosteronism).
Extrarenal polyuria also occurs when there is an increase in fluid in the vascular bed. For example, with intravenous drip administration of solutions with diuretics, that is, forced diuresis. The doctor prescribes diuretic medications to reduce swelling. Excess fluid from the tissues returns to the bloodstream, and its excess is excreted along with urine.
How to treat polyuria
Pathology therapy is aimed at eliminating the cause. To restore normal concentrations of calcium, sodium, chloride and potassium, the patient is prescribed an individual nutrition plan. Additionally, the doctor calculates the amount of fluid consumed. If the body experiences severe dehydration, rehydration is necessary. It is carried out in two ways:
- Infusion of sterile solutions into a vein. Ready-made products are used that contain a certain proportion of electrolytes and carbohydrates, for example, Oralit, Regidron.
- Parenteral rehydration is indicated for more severe degrees of dehydration. Such patients are given intravenous saline, the amount being calculated taking into account their weight.
As soon as the water balance is restored, droppers and injections are canceled. Increased nighttime diuresis is eliminated by limiting drinking and avoiding diuretics in the afternoon. If the cause of the pathology is weakening of the pelvic floor muscles, then special exercises are prescribed to strengthen them. Gymnastics, which was developed by the famous doctor Kegel, brings good results.
Diet food
With an increase in daily diuresis, electrolytes - solutions of necessary chemical elements - are excreted from the human body in large quantities. Following a special diet helps restore their levels. It is necessary to exclude coffee, confectionery, preserves containing vinegar, fatty foods, and spices from the diet. Table salt is limited to 5-6 g per day.
You also need to reduce your intake of carbohydrate foods, including pasta, potatoes, and baked goods. To restore the level of a specific microelement, the menu includes:
- Potassium. It contains nuts, spinach, legumes, and dried fruits.
- Calcium. Found in cheese, dairy products, buckwheat, greens, and nuts.
- Sodium. Contained in lamb, beef, dill, beets, carrots, garlic, white beans.
Drug treatment
Medicines are prescribed taking into account the etiology of increased diuresis. If a patient is diagnosed with a bacterial infection of the genitourinary system, then antibiotics such as Amoxiclav, Ciprofloxacin, Cefepime can be used. They destroy the pathogen, thereby eliminating the symptoms of the disease itself. In addition to antibiotics, depending on the diagnosis, the following are prescribed:
- Electrolyte infusion solutions (calcium chloride, magnesium sulfate). Administered through droppers to restore the acid-base balance of the blood, eliminate the effects of intoxication and dehydration.
- Cardiac glycosides (Digoxin, Verapamil). Indicated for diseases of the cardiovascular system. Used to increase myocardial strength, reduce heart rate, and improve blood supply to weakened cardiomyocytes.
- Thiazide diuretics (Chlortiside, Indapamide). Prescribed to patients with diabetes insipidus. Thiazide diuretics cause less harm to the body compared to loop diuretics. The main effect of the drugs is to stabilize the specific density of urine.
- Diuretics of plant origin (Canephron). Used for cystitis, pyelonephritis, glomerulonephritis, to prevent the development of urolithiasis.
- Hormonal therapy for endocrine pathologies. It can be prescribed to women during menopause to restore hormonal levels. For this purpose, estrogen and progestogen preparations are used.
- Antidiabetic agents (Glibenclamide, Siofor, Glucophage). Used for diabetes. Necessary for normalizing glucose levels, which helps retain water and reduce its excretion in the form of urine.
Surgery
Surgical methods of treatment are resorted to if a patient is diagnosed with malignant tumors, large numerous cysts in the kidneys, or urolithiasis. In severe cases of diabetes, a pancreas transplant may be performed. A timely visit to the doctor will help avoid surgical intervention. Most patients get rid of urinary problems using conservative methods.
Urine formation during pregnancy
A change in the amount of daily urine is prescribed when there is a suspicion of hidden edema or a threat of developing preeclampsia or eclampsia. For pregnant women, daily diuresis is prescribed according to indications; the analysis is not included in the list of mandatory ones for expectant mothers.
Diuresis
(diuresis; Greek diureō to excrete urine) - the amount of urine excreted over a certain period of time (day, hour, minute).
In a healthy adult, daily D. is up to 75% of the amount of fluid drunk. The minimum volume of urine required for the kidneys to excrete the entire amount of metabolic products formed during the day is 500 ml
.
Thus, the volume of fluid consumption should be at least 800 ml
per day.
Under standard water conditions (consumption of 1 1/2 -2 liters
of liquid per day), D. is approximately 1200-1500
ml
per day (for men 1000-2000
ml
, for women 1000-1600
ml
).
In children, D. depends on the age of the child. A newborn's bladder typically contains a small amount of urine, which is released immediately after birth. In the next 2-3 days, daily D. is 20-40 ml
of urine.
Sometimes in the first 2-3 days of a newborn’s life, anuria is observed due to insufficient fluid intake. Lack of urination in these cases is not a pathological condition. Starting from the 4th day of life, the daily amount of urine gradually increases, reaching an average of 150 ml
ml
by the end of the 2nd week .
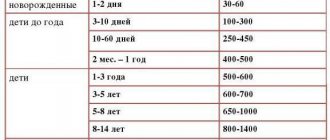
By the end of the first year of life, a child’s daily D. averages 450 ml
, from 1 to 5 years - 750
ml
, from 5 to 10 years - 950
ml
, from 10 to 15 years - 1200
ml
. This indicator in children over 1 year of age can be approximately calculated using the formula:
600 + 100× (X
- 1)
ml
per 24
hours
,
where x
— the child’s age in years.
Under pathological conditions, the amount of urine excreted can vary significantly. D. in an adult is considered pathological below 500 ml
and above 2000
ml
against the background of a normal drinking regime.
Excretion of less than 400-500 ml
of urine is considered oliguria, less than 200
ml
of urine is considered anuria.
Daily D. exceeding 2000 ml
of urine is characterized as polyuria.
The latter may be due to the lack of circulating vasopressin - antidiuretic hormone (ADH) and (or) impaired renal concentrating ability. In clinical practice, polyuria due to insufficient production of ADH is most often detected in diabetes insipidus,
less often in electrolyte disorders (hypokalemia, hypercalcemia) and prolonged
polydipsia.
Polyuria due to impaired concentrating ability of the kidneys is observed in a number of hereditary kidney diseases (renal diabetes insipidus, renal tubular acidosis, Fanconi syndrome); excessive fluid consumption (with psychogenic polydipsia, sugar e); chronic kidney diseases; electrolyte disturbances (hypokalemia, hypercalcemia and hypercalciuria); osmotic diuresis (for chronic renal failure, glucosuria, after eliminating urinary tract obstruction).
For the listed diseases and pathological conditions, there are 2 types of urinary disorders - moderate and severe polyuria. Moderate polyuria - excretion of no more than 3-4 liters
urine per day against the background of impaired nitrogen excretion function of the kidneys, for example, in chronic renal failure, hypokalemia, hypercalcemia, Fanconi syndrome.
Severe polyuria with the release of about 5 liters
of urine (maximum 10-12
liters
) against the background of preserved nitrogen excretion function of the kidneys is detected,
as a rule, in diabetes insipidus, psychogenic polydipsia and familial renal insipidus.
In addition to the quantitative characteristics of D., the rhythm of urine excretion and content are also important. it contains osmotically active substances. Throughout the day, urine excretion in a healthy person occurs unevenly, which depends mainly on the drinking regime and physical activity. In clinical practice, the daily rhythm of urine excretion and the concentrating ability of the kidneys are assessed using the Zimnitsky test, which is carried out under standard food and water conditions with the patient’s normal physical activity. 3 days before the test, diuretics are discontinued. When assessing the sample, the total amount of urine in all 8 portions is taken into account, which is the daily D.; daytime and nighttime D. are calculated separately and fluctuations in the relative density of urine in the collected portions are analyzed. Normally, the amount of urine excreted per day corresponds to the average values (1200-1500 ml
); daily diuresis is 60-80% of the daily amount of urine. The relative density of urine during the day ranges from 1005 to 1025.
Signs of renal dysfunction are changes in the amount (decrease or increase) of urine excreted, increased urination at night (nocturia), and a decrease in the amplitude of fluctuations in the relative density of urine. The latter can be manifested by a state of hyposthenuria, in which the maximum relative density of urine is less than 1020; a state of hypersthenuria, characterized by an increase in the minimum relative density of urine to 1010 or more; a state of isosthenuria, when the relative density of urine in samples is fixed at the level of 1008-1010. To clarify the nature of the disorders, additional research is needed under the conditions of using stress tests to concentrate and dilute urine.
Depending on the amount of osmotically active substances excreted in the urine and the volume of urine, antidiuresis, water and osmotic diuresis are distinguished. Antidiuresis is characterized by the release of a small volume of urine 0.5-0.7 l
/day (0.35-0.5
ml/min
) with a high concentration of osmotically active substances; the ratio of urine osmolality to plasma osmolality approaches 4. Antidiuresis develops when there is a high concentration of ADH in the blood. The distal tubules and collecting ducts are completely permeable to water under these conditions. At a high concentration of osmotically active substances in the renal interstitium, intense reabsorption of water occurs. In healthy individuals, antidiuresis can be observed during the transition from prolonged hypokinesia to normal physical activity. Antidiuresis is detected with blood loss, after surgical interventions on the organs of the chest and abdominal cavity, with loss of fluid due to vomiting and diarrhea; with heart failure, development of nephrotic syndrome, acute eitis, cirrhosis of the liver.
Water diuresis is characterized by the release of a large volume of urine with a low content of osmotically active substances. Minute D. reaches 12-14 ml
, the osmolality of urine can decrease to 50
mOsmol/kg
H 2 O, the ratio of urine osmolality to plasma osmolality is less than 1. With aqueous D., the release of ADH is blocked, the distal tubules and collecting ducts are impermeable to water, the osmolarity of the renal interstitium is low.
In healthy individuals, water diarrhea develops after consuming a large amount of liquid, during the transition from normal physical activity to strict bed rest, to a state of weightlessness. It is also observed with diabetes insipidus, hypokalemia, hypercalcemia, chronic sugar, with polydipsia, acute renal failure, during the period of swelling.
Osmotic D. is characterized by the release of a large volume of urine - up to 10 l
/day (up to 7
ml/min
) and high daily excretion of osmotically active substances (sodium concentration in urine 50-70
mmol/l
); the ratio of urine osmolality to plasma osmolality is higher than 1. The development of osmotic D. is associated with the entry into the proximal nephron of large quantities of endogenous (glucose, urea, bicarbonate) or exogenous (mannitol, simple sugars) osmotically active substances. According to the nature of these substances, endogenous and exogenous osmotic D. are distinguished. Endogenous osmotic D. is detected with decompensated sugar e, exogenous - with the use of osmotic diuretics.
The so-called anionic diuresis has development mechanisms similar to osmotic D., which is observed with a high load of proximal tubules with unreabsorbed anions, such as the anions of keto acids at
In a routine urine test, unless specifically indicated, the amount delivered is not significant and is not noted in the analysis, except in cases where very little urine is delivered, as a result of which some data (for example, specific gravity) cannot be identified.
The amount of morning urine (usually 150 - 250 ml) does not give an idea of daily diuresis and measuring its volume is only advisable for interpreting its relative density. Measuring the amount of urine is important primarily for assessing daily diuresis.
Classification
Doctors distinguish several types of diuresis:
- day. The amount of urine excreted during the period 9–21 hours;
- night. Volume of urine excreted from 21:00 to 9:00;
- minute. With an average rate of fluid consumption, the indicators range from 0.5 to 1 ml;
- daily. Total volume of urine per day. Most of the fluid and dissolved substances are excreted during the day. For this reason, doctors consider the following indicators to be optimal: nighttime diuresis - 1 part, daytime diuresis - 3 or 4 parts;
- forced diuresis. In case of poisoning with signs of acute intoxication, active removal of fluid with dissolved toxins is required. For this purpose, the victim consumes a large volume of water and diuretics, which enhance (force) the outflow of urine from the body.
Classification of diuresis according to the concentration of osmotic substances in urine and the volume of urine:
- water. With an increase in the volume of fluid drunk, the production and excretion of urine increases. The density and concentration of osmotic substances is lower than with normal drinking regimen. In some cases, an increased volume of excreted fluid appears against the background of such pathologies and disorders as the early stages of chronic renal failure, potassium deficiency, increased calcium levels in the blood, polydipsia, decreased tissue swelling;
- antidiuresis. A dangerous condition develops against the background of active loss of fluid due to diarrhea, uncontrollable vomiting, fever, and other problems that provoke dehydration. With a low urine volume, a high concentration of dissolved substances is noted;
- osmotic. The increased volume of urine contains a large percentage of osmotic substances. Causes: diabetes mellitus, chronic renal failure, taking osmotic diuretics.
Method for determining the amount of urine
To determine the amount of urine (daily or collected over a certain time, taken with a catheter, etc.), it is poured into measuring cylinders and, holding the vessel at eye level, the amount is noted. The narrower the diameter of the measuring vessel, the more accurate the quantity measurement. Therefore, small graduated cylinders are used to measure small quantities. In cases where it is necessary to carry out a microscopic examination of urine, the quantity is measured after collecting the sediment.
The normal amount of urine excreted during the day with a normal mixed diet depends on the age and gender of the patient.
Age norms for daily diuresis
| Age | Daily diuresis (in ml) |
| newborn | 0 — 60 |
| 1 day | 0 — 68 |
| Day 2 | 0 – 82 |
| Day 3 | 0 – 96 |
| 4 day | 5 — 180 |
| 5 day | 20 — 217 |
| Day 6 | 42 — 268 |
| Day 7 | 40 — 302 |
| Day 8 | 59 — 330 |
| Day 9 | 57 — 355 |
| 10 day | 106 — 320 |
| Day 11 | 120 — 217 |
| 12 day | 207 — 246 |
| 15 years | 600 — 900 |
| 5 – 10 years | 700 — 1200 |
| 10 – 14 years | 1000 — 1500 |
| Adult women | 1000 — 1600 |
| Adult men | 1000 — 2000 |
Premature babies and bottle-fed babies have slightly higher diuresis.
The largest amount of urine is excreted during the daytime with a peak from 15 to 18 hours, and the smallest amount is excreted at night with a minimum from 3 to 6 hours. The ratio of daytime to nighttime diuresis is 3:1 - 4:1.
Violations
The normal minimum daily diuresis is 500 ml. In this case, drink at least 800 ml of liquid. This volume is necessary for the kidneys to eliminate processed products. If any disturbances occur in the body, the indicators change.
Based on the ratio of fluid produced to active substances, diuresis disorders are divided into several types:
Even more interesting:
Sores around the head
Mouth ulcers hiv
Clinical significance of daily diuresis
Under various physiological and pathological conditions, daily diuresis can either increase or decrease.
Polyuria
An increase in the daily amount of urine is called polyuria
.
Physiological polyuria
may be related to:
- increased drinking regime,
- eating foods that increase urine output (watermelons, melons, etc.).
Pathological polyuria
observed when:
- resorption of edema, transudates and exudates,
- after feverish conditions,
- primary aldosteronism,
- hyperparathyroidism,
- diabetes mellitus and diabetes insipidus (up to 4 - 6 l),
- hydronephrosis (intermittent polyuria),
- in nervous, mentally excitable children (paroxysmal polyuria),
- polyuric phase of acute renal failure,
- after taking certain medications (diuretics, cardiac glycosides).
Oliguria
Oliguria
- This is a decrease in the amount of daily urine. Usually we should talk about oliguria when diuresis decreases below 1/3 - 1/4 of the age norm.
Physiological oliguria
According to the mechanism of occurrence, it is prerenal and is observed:
- in the first 2 - 3 days after birth due to insufficient lactation,
- with limited drinking regime,
- when losing fluid through sweat in hot weather or when working in hot shops, during physical exertion.
Pathological oliguria
According to the mechanism of occurrence, it can be prerenal, renal and postrenal.
Prerenal oliguria
The basis of prerenal oliguria
there is insufficient blood supply to the kidneys due to hypovolemia, which can be caused by:
- excessive loss of fluid extrarenally (vomiting, diarrhea, increased perspiration at high fever, shortness of breath),
- blood loss,
- loss of fluid through the renal route during an overdose of diuretics,
- insufficient blood circulation in the kidneys, associated with a decrease in cardiac output in patients with heart diseases (myocarditis, heart defects, etc.).
Renal oliguria
Renal oliguria
occurs when the kidneys themselves are damaged. Moreover, it may be due to involvement in the pathological process:
- glomeruli (various variants of glomerulonephritis),
- tubulointerstitium (interstitial nephritis),
- renal vessels (systemic vasculitis, hemolytic-uremic syndrome, embolism).
Postrenal oliguria
Postrenal oliguria
occurs when:
- bilateral obstruction of the urinary tract (urolithiasis, formation of blood clots during renal bleeding, tumor process in the retroperitoneum or in the bladder),
- obstruction of the urethra (stricture, stenosis, tumor).
What are the causes of the disease?
Polyuria occurs due to a number of both physiological and pathological reasons; it can be either a normal reaction of the body or a consequence of serious metabolic disorders.
Physiological causes of polyuria:
- Significant water consumption due to habits, cultural traditions, excessively salty foods. Water loss bypassing the bladder per day is about 0.5 liters. If you drink more than 3.5 liters, the concentration of salts in tissues and blood density decrease. These changes are temporary; the kidneys immediately strive to restore balance, removing large volumes of fluid. Urine in this condition is diluted, with reduced osmolarity.
- Drinking large amounts of liquid due to mental disorders. If it reaches 12 liters per day, the osmolarity of the blood drops significantly, the body tries to get rid of moisture in all possible ways, vomiting and diarrhea occur. If the patient denies increased water consumption, it is quite difficult to diagnose him.
- Intravenous fluid intake in the form of saline or parenteral nutrition in inpatients.
- Treatment with diuretics. Diuretics are prescribed to remove excess fluid and salts. When they are used, the amount of intercellular fluid decreases slightly and swelling disappears.
Pathological causes of polyuria include an increase in urine volume due to diseases:
- Central diabetes mellitus occurs when the functions of the pituitary gland or hypothalamus are impaired. In this case, polyuria results from a decrease in the production of antidiuretic hormone.
- Nephrogenic diabetes insipidus is a disorder in the nephrons' perception of antidiuretic hormone. As a rule, it is incomplete, so the resulting polyuria is insignificant, about 3.5 liters.
- Lack of potassium and excess calcium due to metabolic disorders or dietary habits cause minor deviations in kidney function.
- Diabetes mellitus increases blood density due to increased glucose concentrations. The body strives to remove sugar along with water and sodium. Concomitant metabolic changes prevent reabsorption of primary urine. Polyuria in diabetes mellitus is a consequence of both of these causes.
- Kidney diseases that lead to changes in the tubules and kidney failure. They can be caused by infection and subsequent inflammation, damage to the vessels supplying the kidney, hereditary syndromes, replacement of renal tissue with connective tissue due to lupus or diabetes.
Some medications can also cause pathological polyuria. The antifungal amphotericin, the antibiotic demeclocycline, the anesthetic methoxyflurane, and lithium preparations can reduce the ability of the kidneys to concentrate urine and cause polyuria. With prolonged use or significant dosage excesses, these changes become irreversible.
Literature:
- A. Ya. Althauzen “Clinical laboratory diagnostics”, M., Medgiz, 1959
- A. V. Papayan, N. D. Savenkova “Clinical nephrology of childhood”, St. Petersburg, SOTIS, 1997
- L. V. Kozlovskaya, A. Yu. Nikolaev. A textbook on clinical laboratory research methods. Moscow, Medicine, 1985
- Manual of clinical laboratory diagnostics. (Parts 1 - 2) Ed. prof. M. A. Bazarnova, Academician of the USSR Academy of Medical Sciences A. I. Vorobyov. Kyiv, “Vishcha school”, 1991
- Handbook “Laboratory research methods in the clinic”, ed. prof. V.V. Menshikova Moscow “Medicine” 1987
- V. N. Ivanova, Yu. V. Pervushin and co-authors “Methods for examining urine and the clinical and diagnostic significance of indicators of the composition and properties of urine”, Methodological recommendations, Stavropol, 2005.