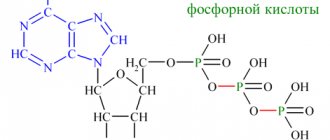
Urine contains mainly water, electrolytes, organic matter, and is a product of material metabolism and filtration of blood in the kidneys. The composition of urine is constantly changing and depends on the intensity of glomerular filtration, the level of reverse absorption of water and biologically active substances from primary urine and/or renal excretion. Assessing the composition of urine allows one to judge the functional capabilities of the kidneys, the stability of metabolic processes in the body, the presence of pathologies, and the effectiveness of the treatment tactics used. Normally, bilirubin metabolic products should not be present in urine. Bile pigments are quantified by special tests.
Pigments are formed from hemoglobin, which contains red blood cells.
What are bile pigments?
Bile pigments are products that are formed from hemoglobin, which contains red blood cells. The cells are destroyed to produce bilirubin in a free, unbound state. Once in the liver, this substance reacts with glucuronic acid and a bound pigment is formed. In this form, it enters the bile, and with it into the intestines.
When reacting with intestinal microflora and enzymes, urobilinogen is obtained. This compound is partially absorbed into the blood and then excreted in the urine. With pathologies of the bile-forming system, such as a removed gallbladder, an inflamed liver, bilirubinuria and urobilinogenelia develop.
What do urine pigments “tell”?
Taking into account the biochemical transformations and properties of bile pigments, their determination can be considered a reliable sign of liver damage and the inability to cope with the disposal of red blood cell breakdown products.
When bilirubinuria is detected, 2 variants of pathology should be assumed:
- disruption of the functioning of liver cells (inflammation, loss of number due to replacement by scar tissue, compression by edema, dilated and overcrowded bile ducts), this process is confirmed by checking the content of aspartic and alanine transaminases, alkaline phosphatase, and total protein in the blood;
- accumulation in the blood of an increased content of hemoglobin from destroyed erythrocyte cells; for clarification, a study of the hematopoiesis process and analysis of bone marrow punctate will be required.
Types of pigments
Urine may contain 2 types of bile substances: bilirubin, urobilinogen, which are formed during the division of red blood cells. If there are no pathologies in the body, urine should normally not contain bilirubin pigment. The concentration of urobilinogen throughout the day can vary within different limits, without exceeding the norm. Over time from the moment of collection of the material, urobilinogen in the urine is converted into urobilin.
Bilirubin pigment
When bilirubin increases, the urine turns dark brown.
The substance should not be detected in urine by classical laboratory tests, such as general and biochemical analysis. Normally, this metabolic product should be removed from the body. When its limit in urine is increased, bilirubinuria develops. Urine turns dark brown. The phenomenon often occurs when the gallbladder has been removed.
The free substance is insoluble in water, so it is not found in urine. The property of solubility is endowed with a compound bound by hepatic glucuronic acid. When the pigment is elevated in the blood, the excess is excreted from the kidneys into the urine. Increased bilirubin is observed against the background of progression of liver and biliary tract diseases. As a result of stagnation, rapid formation of cholesterol and bilirubin pigment occurs. They form a sediment in the bile with gradual crystallization, which becomes overgrown with calcium salts and other components, which leads to the formation of stones.
If jaundice of the skin appears, but there is no pigment in the urine, hemolytic jaundice is diagnosed. In this case, increased bilirubin is found in the blood. As a result of such hemolysis, indirect bilirubin pigment is not filtered by the kidneys, which means it is not excreted in the urine. The causes of bilirubinuria are:
- stone formation in the kidneys and urinary tract;
- failures in the diet with a large amount of carbohydrates;
- pathologies that cause rapid destruction of red blood cells, for example, blood diseases, malaria, sickle cell anemia, chemical intoxication.
The formation of urobilinogen is provoked by various diseases.
The substance is formed from bilirubin pigment when it reacts with intestinal enzymes. A small concentration of colorless urobilinogen should be in the urine.
This substance is oxidized to form yellow urobilin. If its content is exceeded, the urine becomes dark.
Urobilinogen is created at a specific rate, so it is regularly excreted in feces and partially in urine. An increase in the rate of its formation is provoked by various diseases. In some cases, the rate drops, then the pigment is not detected in the urine. Exceeding the concentration is usually associated with pathologies that cause intense breakdown of red blood cells, which provokes an increase in the amount of free hemoglobin, which is a source of excess bilirubin, and therefore urobilinogen.
Reasons for excess urobilin in urine:
- malaria;
- bleeding from the gastrointestinal tract, lungs, female genital organs;
- Werlhof's disease;
- Biermer's anemia or hemolytic jaundice;
- lobar pneumonia;
- hemorrhagic diathesis;
- liver diseases;
- severe biliary tract infections;
- cardiac dysfunctions;
- stagnation in the intestines.
If urobilinogen is not present in the urine, then you need to check the bile duct for blockage. For this reason, the passage of bile with bilirubin substance is disrupted.
Rules for collecting urine for analysis
The result of a urine test is influenced by the correct collection of the necessary material. If the rules are not followed, the result may be inaccurate. Accordingly, the prescribed therapy will also be incorrect.
When collecting urine, it is important to follow several rules.
Among them:
- The night before collecting material for analysis, it is necessary to perform a thorough external toilet of the genital organs.
- Collect urine in a special container in the morning. The container may not be sterile, but it must be clean.
- Remove the collected material to a dark place. Bile pigments are destroyed in light. Therefore, if it is not possible to immediately submit urine to a laboratory, it is better to put the material in the refrigerator. Here urine can be stored for no more than 2 hours.
- It is enough to collect 30-50 milliliters for research.
It is important to promptly detect the presence of bile pigments. Any violations or deviations from the norm can cause the development of serious diseases and complications.
Why is pigment analysis needed?
A change in the concentration of bile pigments in urine indicates the presence of a pathology that disrupts the process of dissolution of bilirubin pigment and filtration of urobilinogen. In this way, it is possible to diagnose complications due to a removed gallbladder, liver disease, and determine how well the stones were removed from the biliary system.
Bile pigments (bilirubin, biliverdin, etc.) are formed during the breakdown of hemoglobin in erythrocytes and appear in the urine during jaundice. Urine containing bile pigments is yellowish-brown or green in color (a characteristic sign of jaundice).
Test for bilirubin with iodine solution (Rosin's test)
Carefully add a 1% alcohol solution of iodine or Lugol’s solution to 3 ml of urine. When bilirubin is present, a green ring forms at the interface between both fluids. With normal urine the test is negative.
Gmelin's test for bile acids
Carefully add an equal volume of urine to 1 ml of concentrated nitric acid along the wall. In the presence of bile pigments, a green ring is formed at the border of the layering.
Methods for determining pigments in urine
It is important to carry out the most accurate and correct diagnostic measures in order to refute or confirm the pathology. To do this, you need to examine your urine for the presence of pigments. The analysis will help identify substances contained in the urine.
Bilirubin can be detected by oxidation of the starting material with iodine or nitric acid. If a pigment substance is present, the urine turns green during the reaction. For analysis, you need to take a sterile test tube and add 5 milliliters of urine. Then the solution containing iodine is added layer by layer.
As the last one take:
- Lugol;
- potassium iodide;
- alcohol tincture.
To check urobilin levels, you need to remove bilirubin from the urine. The pigment will interfere with the reaction carried out with a solution of calcium chloride and ammonia.
After eliminating bilirubin, you can begin various tests:
- Copper sulfate. It is combined with urine by adding a chloroform solution. The “cocktail” is shaken. The solution should turn intense pink.
- Spectroscope. The decoding will show the remainder of the blue-green part of the spectrum.
The color intensity of the solution during testing is marked with crosses. One will mean a weakly positive reaction, and 4 plus signs will mean a strongly positive reaction.
Determination of the level of bile pigments can only be carried out in special laboratories and clinics where biochemical reagents are available.
Qualitative determination of indican in urine.
Indican, a potassium or sodium salt of indoxyl sulfuric acid, is found in trace amounts in normal urine. A lot of indican is found in the urine of herbivores, as well as in human urine with increased decay of proteins in the intestines, with constipation and intestinal obstruction.
Pour 4 ml of test urine into a test tube and add an equal volume of sulfuric acid while stirring. Then add about 1 ml of chloroform, 1 - 2 drops of potassium permanganate solution, close with a stopper and turn over several times without shaking. Place the test tube in a stand and observe the intensity of the chloroform layer turning blue 13. Solve situational problems.
Be able to explain the principle of the determination method and the clinical and diagnostic significance of some biochemical parameters
1. Separation of blood serum proteins by paper electrophoresis and quantitative determination of protein fractions.
Separation and quantitation of proteins
blood serum fractions by electrophoresis on paper.
Principle of the method.
Electrophoresis is the movement of charged particles in a field of direct electric current. The speed of movement of protein molecules in an electric field depends on the charge, molecular weight, pH, and ionic strength of the solution.
Serum proteins are placed on a strip of paper moistened with a buffer solution, through which a direct electric current is passed. At pH 8.6, serum proteins are negatively charged and, under the influence of an electric field, move to the anode.
Human blood serum contains various proteins. Using electrophoresis, 5 fractions are isolated on paper - albumin, α1-, α2-, β-, γ-globulins.
Clinical and diagnostic significance.
Many pathological conditions are accompanied by quantitative changes in the ratio of protein fractions in the blood - dysproteinemia. A decrease in the content of the albumin fraction is characteristic of liver diseases due to a decrease in the protein-synthesizing function of hepatocytes. Hypoalbuminemia also accompanies kidney disease due to protein loss in the urine. An increase in the content of α1- and α2-globulin fractions is observed under stress, the presence of inflammatory processes due to “acute phase” proteins, collagenosis and metastasis of malignant neoplasms. The β-globulin fraction increases with hyperlipoproteinemia. The fraction of γ-globulins increases during immune reactions caused by viral and bacterial infections. A decrease in the γ-globulin fraction can occur in primary and secondary immunodeficiency.
Work order
1. Device design for electrophoresis.
The device consists of a rectifier that supplies direct current at the required voltage, and a chamber for electrophoresis. The chamber itself consists of 2 baths; one of them has a fixed partition where a platinum electrode (+ anode) is placed, and the other contains a stainless steel electrode (- cathode). Between the baths filled with the appropriate buffer, there is a connecting bridge on which strips of special filter paper are placed.
2. Carrying out electrophoresis.
Fill both chamber baths with a solution of veronal buffer with pH 8.6. There should be enough buffer solution in the baths so that it covers the fixed partition, but is below the movable partitions.
Insert electrodes into the baths. Cut strips of filter paper of the required size depending on the size of the chamber (usually 4-6 cm wide) and with a simple pencil mark the place where the serum will subsequently be applied (start). Soak these strips in Veronal buffer. Insert the connecting bridge into the bath chambers. Place strips of paper on dry plates with forceps, immersing the ends of the strips in baths with buffer, and apply 0.025-0.005 ml of serum to pre-marked areas of the paper at a distance of 5-6 cm from the edge of the bridge. Serum is applied from the cathode side.
Figure 1. Diagram of a chamber for electrophoresis of proteins on paper:
1-stabilizer; 2-chamber for electrophoresis; 3-buffer solution; 4-supporting connecting bridge-electrode; 5-filter paper for electrophoresis.
After applying the serum to the paper strips, the chamber is hermetically sealed with a lid. There is a locking clamp on the camera cover that is used to turn on the camera. The attached rectifier supplies the camera with a constant current of 2 to 4 mA at a constant voltage of 110-160V. Electrophoresis is carried out at a potential gradient of 3 to 8 V per 1 cm of strip at room temperature. Good separation occurs in 18-20 hours.
3. Turn off the device and identify protein fractions.
Turn off the device. Remove the cameras and remove the paper strips from the device. Then each strip is placed in a drying oven for 20 minutes at a temperature of 1050C. In this case, the protein fractions are fixed on paper. Proteins are stained with a bromophenol blue solution for 30 minutes, then the electropherograms are washed with a 2% acetic acid solution. The resulting electropherograms are dried in air. Protein fractions turn blue-green.
4. Quantitative determination of protein fractions.
The colored protein spots are cut out, the dye is eluted with a 0.01 N alkali solution. The color intensity of each fraction is determined colorimetrically using FEC.
Quantitative determination of protein fractions on an electropherogram can be determined in two ways: by elution of the dye and photocolorimetry and by the densitometric method.
albumins 55.4-65.9%
α1-globulins 3.4-4.7%
α2-globulins 5.5-9.5%
β-gdobulins 8.9-12.6%
γ-globulins 13-22.2%
Densitometric method.
In a special apparatus (densitometer), a beam of light is passed through the electropherogram, the absorption of which depends on the optical density of the colored protein spots. The light passing through the electropherogram is captured by a photocell and converted into an electric current, the vibrations of which are recorded on a paper sheet in the form of a curve, each peak of the curve corresponds to a certain protein fraction.
Figure 2. Electropherogram of human serum.
One of the important indicators of urine analysis is bile pigments. Urobilinoids in urine can indicate a number of diseases. Such pigments are formed as a result of the breakdown of hemoglobin and other proteins that contain it. They are present in bile and give it a yellowish color. The greatest value among the indicators is, of course, bilirubin and its transformation products, which are formed under the influence of intestinal microflora. We are talking about bilirubinoids. To detect them, the urine should be carefully tested.
Bile pigments in urine may indicate serious illness
Even if a person is healthy, urobilinogens can always be found in his urine, which, after oxidation by urine, turn into urobilins. Urine must stand in the light for a day so that urobilinogen is completely converted into urolibin. It is for this reason that fresh urine is examined for the content of urobilinogen, and standing urine for the content of urobilin.
Urobilinogen in urine is colorless, but urobilin is yellowish. These properties explain the fact that urine becomes darker over time. These substances are derivatives of bilirubin, which is excreted in bile - urobilinoids. If we compare the chemical structure of urobilinoids, it is obvious that it is close and similar.
These substances are not detected if bilirubin has not reached the intestines. This can happen due to many diseases - blockage of the bile ducts, fistulas, hepatitis.
With a high content of urobilinoids, we can talk about increased hemolysis, viral hepatitis, acute infections, heart or vascular failure, bleeding, and so on.
In the same case, if urobilinoids are not detected in the urine, but a icteric state is visible on the face, dystrophy of the liver tissue most likely develops.
When is the level of bilirubin in urine impaired?
Unconjugated bilirubin appears in the blood in liver diseases:
- viral hepatitis;
- toxic hepatitis due to poisoning with toxic substances (medicines);
- severe consequences of allergies;
- cirrhosis;
- oxygen hypoxia of liver tissue in heart failure;
- metastatic damage to cancer cells from other organs.
But it does not pass into urine due to the impossibility of filtration. Only in the case of renal and hepatic failure with destruction of the nephron membrane can it be detected in urine.
Urobilin standards
Urobilin in the urine of healthy people should be contained in scanty levels. There is so little of it that tests show negative results. It is clear from this that, under normal conditions, urobilins should not be detected in the urine.
The principle of formation of urobilinogen in urine
However, some body conditions can affect test scores. Reactions can be slightly positive (indicated by +), positive (2+) and strongly positive (3+). Elevated urobilin levels are called urobilinuria.
It is important to determine urobilin levels in urine, because the indicators can be used to judge how effective the urinary system is. The normal color of urine is clear or slightly yellowish. If the body suffers from fluid deficiency, then the amount of water in urine becomes less, and urobilin becomes more concentrated and the urine darkens. Also, certain medications, dietary regimens, and a hereditary disease such as alkaptonuria can affect the darkening of urine.
An increase in urobilin levels occurs under the following conditions:
- Impaired liver function. In this case, the organ cannot cope with the removal of urobilin.
- The formation of urobilin in excess in the intestines.
- Mechanical jaundice. In this case, urobilin is determined by the degree of blockage of the bile ducts. With complete blockage there is no urobilin in the urine, with incomplete blockage there is little of it. After the obstacle is removed, urobilinuria occurs due to the fact that a large amount of bilirubin enters the intestines.
Many experts insist that urobilin levels are not accurate evidence of the presence of the disease, but only indicate its possibility. Most often, a mechanism simply triggers to dump excess bioslag into the intestines. And this is an additional burden on the kidneys, which in this case cannot cope with their direct responsibility.
Reasons for appearance
In the normal state, bile in the urine is contained in minimal concentrations, which can fluctuate throughout the day, but do not exceed permissible limits. Normally, only urobilin is excreted in urine. The appearance of bound soluble bilirubin indicates pathology. At the same time, the substance itself is always elevated in the blood; the value of the indirect fraction may vary.
The absence of urobilin occurs with inflammation, tumor blockage of the bile ducts, impaired urination, and terminal liver lesions.
Video: All about bilirubin
In adults
In practice, doctors more often encounter disturbances in the excretion of heme breakdown products in the working population. Reasons that cause the appearance of bilirubin in urine:
- GSD, cholestasis;
- infections;
- intoxication, poisoning;
- hepatitis, Botkin's disease;
- cirrhosis;
- tumors of the hepatobiliary tract;
- removed gallbladder;
- intestinal obstruction;
- disorders of the heart and blood vessels leading to hypoxia of the parenchyma;
- hypothyroidism
Urobilin increases under the following conditions:
- Diseases of the liver parenchyma, when reuptake of bilirubin does not occur and high concentrations of pigments remain in the blood, exceed the renal filter and are found in the urine.
- Increased hemolysis of red blood cells. In addition to the physiological increase during menstruation and the neonatal period, it occurs with malaria, pneumonia, bleeding of various locations, disorders of the coagulation system, and sepsis.
- Gastrointestinal pathologies with increased absorption of hemoglobin breakdown products: chronic constipation, intestinal obstruction.
In children
Urobilin in infants is often elevated. The phenomenon is associated with physiological adaptation: the replacement of fetal hemoglobin is accompanied by an increase in the breakdown of red blood cells, and newborn jaundice occurs. It is important to monitor the dynamics of the condition: a rapid increase in the concentration and appearance of bilirubin in urine indicates a disruption of the natural process and the appearance of pathology.
At an early age, the cause of the appearance of pigments in urine is:
- genetic damage to the enzymatic transformation of bilirubin - Rotor, Crigler, Dubin-Johnson syndrome;
- disorders of the blood system (hemorrhagic diathesis, Werlhof's disease);
- hemolytic jaundice;
- intussusception followed by intestinal obstruction.
During pregnancy
At the time of gestation, the load on all organs and systems increases. Even in healthy women, an increase in urobilinogen can be detected in the urine. In this case, patients complain of darkening of the urine. In cases where there is pathology of the biliary system before pregnancy, the condition may worsen. Additionally, increased work of the heart and kidneys plays a role, contributing to an increase in the volume of blood volume and the concentration of absorbed substances.
Monitoring the level of bile pigments allows you to indicate the onset of an exacerbation. In a patient in an interesting position, it is necessary to exclude cholecystitis, viral hepatitis, pyelonephritis, and coagulation system disorders.
Causes of urobilinogen
Also, as in the case of urobilins, urobilinogen in a healthy body is absent in high levels. But still, traces of it should be found in urine. The complete absence of urobilinogen may indicate mechanical blockage of the bile ducts, due to which bile is simply not excreted from the liver, or indicate that renal filtration processes are impaired (this occurs in severe forms of glomerulonephritis, toxic kidney damage and neoplasms).
Test strips for determining bilirubin in urine
A sharp increase in urobilinogen levels may indicate the following conditions.
- Impaired detoxification functions of the liver. When liver cells are damaged and the functionality of the organ decreases, the liver stops processing bilirubin derivatives. For this reason, urobilinoids accumulate in the blood and are excreted in the urine. This happens in acute viral, toxic, drug-induced hepatitis, alcohol intoxication, tumors and cirrhosis.
- . It increases if a person suffers from hemolytic anemia or jaundice, as well as diseases during which red blood cells are massively destroyed.
A child may not have urobilinogen in his urine until he is three months old. And these indicators can be considered the absolute norm. This is explained by the fact that the intestinal microflora of such young children is not yet fully formed, it is not specific and is not capable of oxidizing bilirubin into urobilinogen.
Clinical symptoms
The inflammatory process occurring in the area of the gallbladder is characterized by pronounced symptoms, which cannot help but pay attention to. In the acute form of cholecystitis, the patient is concerned about:
- strong, sharp and persistent pain in the abdominal area, which can radiate to the right shoulder blade;
- excessive increase in body temperature; weakness and chills;
- the appearance of yellowness in the whites of the eyes;
- strong darkening of biological fluid. The color of urine with cholecystitis acquires excessively dark shades due to an increase in the level of bilirubin in the blood;
- presence of light-colored stools;
- the appearance of nausea, in rare cases, it may be accompanied by vomiting.
The chronic form of the pathology manifests itself as follows:
- the patient is almost constantly bothered by a dull, aching pain in the area of the right rib;
- mild nausea;
- the appearance of unpleasant heaviness in the stomach after eating fatty, spicy, fried foods and sweet carbonated drinks.
Sometimes clinical symptoms of pathology can appear after the body has been subjected to severe stress: hypothermia, overwork, being in a sitting position for a long time, depression, etc.
What to do
First of all, after conducting tests and detecting urobilinoids in the urine, there is no need to panic. Do not forget that negative states such as fear and anger can further aggravate the situation, have a detrimental effect on your physical health and lead to stagnation. Namely, stagnation is the cause of most inflammation and disease.
Once accurate results are obtained, you must definitely reconsider your diet and choose a suitable dietary regimen that will be gentle on your liver. Do not forget about the daytime regime, remember that the greatest activity of the liver occurs during the period from 21.00 to 3.00, but only if you are in an absolutely calm state, that is, sleeping. To put your body in order, wake up no later than 7 o’clock, and go to bed no later than 10 pm.
Regarding the dietary regime, it is worth adding the following. Give preference to a vegetable-dairy diet; it will improve the functioning of not only the liver, but also other important organs. It is also recommended to drink bitter herbs in order to improve bowel function. These include elecampane, wormwood, immortelle, milk thistle and tansy. To prepare an infusion, take a large spoon of any of the herbs listed, pour half a liter of boiling water over it and let it brew. Take a quarter glass before or after meals. Warm before use.
Sports, active recreation and water treatments should occupy an important place in your life. In this way, you will help ensure that toxins are better removed by the body not only through the excretory system, but also through the skin.
Principle.
Bile pigments in urine are determined by bilirubin and urobilin.
Determination of bilirubin (Rosin test).
Rosin's test is based on the transformation of bilirubin under the influence of oxidizing agents (iodine) into biliverdin, which has a green color.
Diagnostic value.
Normally, bilirubin is not contained in urine.
Bilirubin appears in urine during mechanical (subhepatic)
jaundice (cholesterolitis, obstruction of the common bile duct by a tumor, enlarged lymph nodes) and
parenchymal (hepatic)
jaundice (viral hepatitis, chronic hepatitis, cirrhosis of the liver).
In hemolytic jaundice, bilirubin is not detected in the urine.
Determination of urobilin (Florence test, Bogomolov test).
The most sensitive qualitative reaction to urobilin in urine is the Florence test.
Diagnostic value.
Normally, urine may contain small amounts of urobilin.
Urobilin is found in large quantities in urine in parenchymal (hepatic)
and
hemolytic
jaundice.
Microscopic examination of urine sediment.
Principle.
Microscopy should be carried out no later than 2 hours after urine collection, with low density (less than 1010) - immediately immediately after collection.
Elements of urine sediment, visible under a microscope, are divided into unorganized (salts) and organized (cellular elements, cylinders).
Unorganized urine sediment.
Unorganized urine sediment consists of salts that have precipitated in the form of crystals or an amorphous mass. The nature of the salts mainly depends on the colloidal state and reaction of the urine.
Diagnostic value.
Unorganized sediment has no special diagnostic value. The detection of a large amount of salts in the sediment during a single examination cannot be regarded as a pathological phenomenon.
Crystals of uric acid and urate are found in kidney stones, massive breakdown of tumor cells, leukemic tissue, and also in febrile conditions.
Oxalates are found normally in a plant-based diet.
Organized urine sediment.
Organized urine sediment includes epithelial cells, leukocytes, erythrocytes and casts.
Diagnostic value.
Squamous epithelial cells
enter the urine from the genital tract and partially from the urethra. Normally, there are single (up to 5) cells.
A large number of them is a sign of improperly collected urine - without previous toilet of the perineum.
In cystitis and urethritis, the detection of squamous epithelial cells in the urine is associated with intense desquamation of the mucous membrane and is combined with dysuria.
Damage to the tubular apparatus of the kidneys in nephritis is accompanied by the appearance of renal epithelial
and cylinders.
leukocytes
(up to 5 in the field of view).
Detection of leukocytes in urine sediment above normal - leukocyturia
(up to 50 leukocytes per field of view) or
pyuria
(more than 50 leukocytes per field of view). Leukocyturia (pyuria) is observed in inflammatory diseases of the kidneys and urinary tract (pyelonephritis, cystitis, urethritis, renal tuberculosis).
Normally, single erythrocytes
(up to 3 in view).
Hematuria
- presence of red blood cells in the urine.
Gross hematuria
- detection of blood during urine examination.
Microhematuria -
red blood cells in urine are detected only by microscopy.
Hematuria with a predominance of altered (“leached”) red blood cells is characteristic of acute and chronic glomerulonephritis, renal infarction, and hypernephroma.
Hematuria with a predominance of unchanged (fresh) red blood cells is characteristic of kidney stones, malignant neoplasms, and polycystic disease.
Urinary (renal) casts
are divided into cellular, granular, hyaline, waxy. The place of their formation is the renal tubules. Source: cellular elements, urine protein.
Normally, casts are not detected in urine, with the exception of isolated hyaline casts.
Cylindruria
- the appearance of casts in the urine is observed in renal pathology, accompanied by the release of protein, epithelium, erythrocytes and leukocytes in the urine (glomerulonephritis, pyelonephritis, nephrotic syndrome).
Hyaline casts can also be found in febrile patients, with congestive kidneys.
Granular casts are detected with severe lesions of the renal parenchyma.
Waxy casts are characteristic of nephrotic syndrome, renal amyloidosis, when there is a large amount of protein in the urine.
Cylinders of leukocytes and erythrocytes appear along with a large number of corresponding cellular elements in the urine.
Urobilinogen (mesobilirubinogen) is a product of bilirubin reduction. The latter is a bile pigment formed during the breakdown of proteins containing hemes.
Thus, urobilinogens arise from the disposal of red blood cells. Urobilinogen is formed in the intestines from bilirubin, which gets there along with bile. Under the influence of enzymes and microorganisms, it is oxidized and absorbed back into the blood. After this, it enters the kidneys and is excreted in the urine.
If urobilinogen in the urine is increased and its concentration exceeds 10 mg/ml, we speak of hyperurobilinogenuria. This condition may be a consequence of a violation of the reuptake of urobilinogen by hepatocytes, an increase in the synthesis of precursors of urobilinogen bodies - bilirubin, as well as an increase in the level of its absorption in the intestine. We will look at what this means in this article 34.
Bile analysis
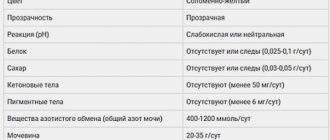
Laboratory study reveals deviations from standard values in its structure. Composition and secretion standards:
- basal - transparent light yellow, density 1007-1015, slightly alkaline;
- vesicular - transparent dark green, density 1016-1035, pH 6.5-7.5;
- liver - transparent light yellow, density 1007-1011, pH 7.5-8.2.
Fractional research will allow us to judge the dysfunction of the biliary system. Portions of bile collected during examination with a probe are sent for biochemistry, and, if necessary, for histology and microscopy. Samples are studied for sensitivity to antibiotics and microflora.
If the analysis indicators deviate from the norm, you can diagnose:
- Inflammatory process. It is characterized by a decrease in the transparency of bile, an increase in leukocytes, and the presence of cylindrical cells.
- Stones in the ducts, stagnation of bile. They are detected with high cholesterol and the presence of calcium crystals.
A study of bile can reveal the presence of helminths in the duodenum and bile ducts.
What it is?
Urobilinogen is formed in the intestine from bile bilirubin (intestinal flora takes part in this process).
Part of the substance is converted into stercobilinogen, which is excreted along with feces, and the second part is absorbed into the blood. The blood predominantly passes through the liver, due to which its cells take up urobilinogen and again convert it into bilirubin, which is then excreted along with bile. However, a small part of the blood passes from the intestine through hemorrhoidal anastomoses without reaching the liver. That is, some amount of urobilinogen still ends up in the urine.
How is urobilinogen formed?
Urobilinogen is a product of the subsequent processing of bilirubin in the intestine by:
- mucosal enzymes;
- bacteria.
More modern data indicate the presence of urobilinogen bodies, which include derivatives:
- mesobilirubinogen,
- i-ypobilinogen,
- urobilinogen IX a,
- d-urobilinogen,
- "third" urobilinogen.
The formation of urobilinogen from conjugated bilirubin occurs in the upper part of the small intestine and the beginning of the large intestine. Some researchers believe that it is synthesized by cellular dehydrogenase enzymes in the gallbladder with the participation of bacteria.
A small part of urobilinogen is absorbed through the intestinal wall into the portal vein and returns to the liver, where it is completely broken down. The other is processed into stercobilinogen.
Further, through the hemorrhoidal veins, these substances can enter the general bloodstream and are excreted into the urine by the kidneys. Most of the stercobilinogen in the lower intestine is transformed into stercobilin and excreted in the feces. This is the main pigment that provides color to feces.
The normal level in urine is considered to be no more than 17 µmol/l. If urine is briefly exposed to air, urobilinogen is oxidized by oxygen and converted into urobilin. This can be seen by color:
- urobilinogen is a colorless substance, fresh urine has a straw-yellow tint;
- after some time, due to the formation of urobilin, it darkens.
Normal level of urobilinogen in urine
Urobilin in the urine of healthy people should be contained in scanty levels. There is so little of it that tests show negative results. It is clear from this that, under normal conditions, urobilins should not be detected in the urine.
However, at least traces of urobilinogen must be detected in the urine of an adult.
Its complete absence is possible in three cases:
- The process of renal filtration is disrupted in severe forms of glomerulonephritis, toxic kidney damage and malignant neoplasms.
- Bile does not exit the gallbladder into the intestines due to mechanical blockage of the bile duct.
- The obstruction may be a stone or compression of the duct by the head of the enlarged pancreas or tumor.
Gradation according to the degree of increase in the level of urobilinoids:
- weakly positive (+);
- positive (++);
- strongly positive (+++).
It is important to determine urobilin levels in urine, because the indicators can be used to judge how effective the urinary system is. Exceeding the norm of urobilinoids is called urobilinuria. This enzyme increases when the liver or intestines are malfunctioning.
When is it necessary to check a urine test for bile pigments?
Qualitative tests for bile pigments are included in the mandatory list of standard urine tests.
Therefore, if the patient complains of:
- dyspeptic disorders;
- vague pain in the hypochondrium on the right;
- yellowness of the sclera, skin;
- darkening of urine and light-colored stool;
- It is necessary to exclude diseases of the liver and gall bladder.
When choosing a method of treating a patient, the doctor must not harm the human organs and systems, so the analysis is needed to exclude the toxic effect of the drug on the liver.
The appearance of jaundice requires examination for bile pigments
Poisoning with various toxic substances is accompanied by damage to kidney and liver function. By identifying bile pigments, the degree of disorder can be tentatively assumed.
In severe myocardial diseases, a positive test indicates the involvement of liver tissue in the formation of general hypoxia.
Causes of increased urobilinogen in urine
Urobilinogen was detected in the urine, what does this mean? An increase in the concentration of urobilinogen in the urine in men and women may indicate excessive production of bilirubin in the liver or a slowdown in its utilization. Similar symptoms most often occur with liver pathologies. Another cause of this condition may be the process of destruction of red blood cells in the body (hemolysis).
We list the main reasons as a result of which high levels of urobilinogen in urine are diagnosed:
- Increased hemoglobin catabolism: hemolytic anemia, intravascular hemolysis (transfusion of incompatible blood, infections, sepsis), pernicious anemia, polycythemia, resorption of massive hematomas.
- Increased formation of urobilinogen in the gastrointestinal tract: enterocolitis, ileitis, intestinal obstruction, increased formation and reabsorption of urobilinogen during infection of the biliary system (cholangitis).
- Increased in liver dysfunction: (excluding severe forms), and toxic liver damage (alcohol, organic compounds, toxins in infections and sepsis).
- Secondary liver failure: after myocardial infarction, cardiac and circulatory failure, liver tumors.
- Increased with liver bypass: liver cirrhosis with portal hypertension, thrombosis, renal vein obstruction.
In some situations, an increase in this indicator above normal is not associated with liver pathology, and may occur due to insufficient fluid intake or its excessive excretion. In this case, the pigment content remains unchanged, and its concentration increases solely due to the loss of liquid.
Disorders of the mechanism of excretion of bile pigments
In some patol conditions, disturbances in the formation, transport and secretion of gastrointestinal tract are observed (see Jaundice). Particularly noteworthy are cases when the retention of bile in the biliary system (due to blockage of the bile ducts or in severe forms of cirrhosis of the liver) is accompanied by the oxidation of part of the bilirubin into biliverdin, which also passes into the blood and gives the icteric color of the sclera, skin and mucous membranes a greenish tint.
Of great interest are experimental and wedge data on hereditary disorders of individual links in the mechanism of transformation and excretion of bilirubin. Thus, in the mutant rats described by Gunn (S. Gunn, 1938), the liver is deprived of the ability to conjugate bilirubin. This depends on the lack of formation or complete absence of specific enzymes in the liver. A colony of such animals was tracked for 19 years, and the belonging of the indicated defect to the number of hereditary disorders was undoubtedly shown. In such rats, the bile is colorless and contains almost no bilirubin. The content of unconjugated bilirubin in the blood serum increases to a maximum level (15-20 mg%). Jaundice develops, edges, as a rule, accompanied by functional and structural disorders of the c. n. With. In these animals, the pigment is not excreted in the urine, but it is secreted by the intestinal mucosa into the intestinal lumen. In addition, part of the bilirubin is converted into diazone-negative compounds, apparently mono- and dipyrroles, which are excreted in bile and urine. If bilirubin glucuronides are administered to such animals, they are excreted as part of bile. The introduction of unconjugated bilirubin does not increase the release of pigment into bile. Thus, metabolic disorders in these animals are associated with a disorder of only one link—the conjugation of bilirubin in the liver.
Another hereditary defect has been described in mutant sheep, in which, while maintaining the ability to conjugate bilirubin, the process of its release from liver cells into bile is disrupted. This probably depends on the lack of a specific transporter of conjugated bilirubin across the cell membrane. The excretion of pigment in the bile of these animals is sharply reduced. It is not free, but conjugated (direct) bilirubin that accumulates in the blood. At the same time, the presence of an unusual pigment of melanin nature is detected in the liver, which, apparently, is formed as a result of a reduced ability of the liver to secrete metabolites of certain amino acids and compounds related to them. At the same time, the secretion of bile acids in these animals is not impaired, and, therefore, they do not have intrahepatic cholestasis, in which general disorders of liver secretion are observed, affecting the secretion of various components of bile. In this case, only one final link in the mechanism of gastric excretion is disrupted.
Similar disorders have been described in humans (Dubin-Johnson syndrome), characterized by chronic non-hemolytic jaundice with a high level of conjugated bilirubin in the blood and the presence of melanin pigment in the liver (see Hepatosis). This disease is familial in nature and is also associated with a disorder of the mechanism of secretion of bilirubin glucuronides and a number of other organic anions, with the exception of bile acids, from liver cells into bile. The discovery and detailed study of hereditary disorders in experiment makes a valuable contribution to the understanding of hepatic transport of glandular fluids and is of great importance in deciphering the genesis of the corresponding syndromes observed in humans in the clinic.
Physiological jaundice of newborns is apparently associated with insufficient maturity of the liver enzyme system responsible for the conversion of bilirubin. Hereditary human hyperbilirubinemia is also accompanied by a violation of the process of bilirubin conjugation, an increase in the content of indirect bilirubin in the blood serum (see Hyperbilirubinemia).
Determination of the content of certain bile pigments in blood serum, urine and feces is used during wedge examinations of patients as an additional diagnostic test for a number of diseases. Thus, an increase in the content of urobilinogen in the urine at a rate of 0-4 mg per day (see Urobilinuria) is observed with hepatitis in its initial stage (see Hepatitis, Viral hepatitis), with liver necrosis (see), with toxic liver damage (see Toxic liver dystrophy), portal cirrhosis, obstruction of infected bile ducts, as well as congestive heart failure, severe acute infections, pulmonary infarction, severe subcutaneous hemorrhages. Normally, 40-280 mg of stercobilinogen per day is determined in human feces (in children the numbers are slightly lower), however, with hemolytic anemia and normal liver function, the excretion of stercobilinogen with feces increases, and with obstruction of the biliary tract, severe hepatopathy, cachexia, some anemias and when taking broad-spectrum antibiotics, it decreases.
See also Bile formation, Bile.
Treatment
Urobilinogen in urine - what does it mean? What to do in this situation? First of all, there is no need to panic. Negative emotions and emotional imbalance lead to stagnation in the body, which will further aggravate the situation. If you have a sharply positive reaction to urobilin bodies, you should consult a doctor and possibly undergo additional studies that will help find out the true cause of this situation.
Once accurate results are obtained, you must definitely reconsider your diet and choose a suitable dietary regimen that will be gentle on your liver. Do not forget about the daytime regime, remember that the greatest activity of the liver occurs during the period from 21.00 to 3.00, but only if you are in an absolutely calm state, that is, sleeping. To put your body in order, wake up no later than 7 o’clock, and go to bed no later than 10 pm.
Infusions of medicinal herbs will also help bring the body back to normal, improve intestinal function and remove excess toxins.
These are bitter herbs, for example, immortelle, wormwood, elecampane, tansy, milk thistle. To prepare a medicinal infusion, take one large spoon of dry raw materials of any of the listed herbs and pour 0.5 liters of boiling water, leave for at least half an hour, then filter. Take 1/4 cup before meals. Facebook
Blood analysis
If the patient’s condition changes in the direction of deterioration, or there is a fear of the development of inflammation in the body, blood is taken to study and determine deviations in its composition.
The doctor prescribes 2 types of examination:
- Clinical (CLA). Determines the number of blood cells. Capillary blood is taken.
- Biochemical. Studies a wide range of enzymes and substances. The object of study is venous blood.
Blood tests for cholecystitis are done after a 12-hour fast. To obtain accurate information, they are carried out at regular intervals.
A general blood test is necessary to determine the number of leukocytes, neutrophils, and ESR. During the period of exacerbation of the disease, they will be increased, which indicates an inflammatory process. A low hemoglobin level will indicate anemia. In a chronic course, blood cell parameters will be normal or less. Long-term inflammation in cholecystitis is indicated by a low level of leukocytes (leukopenia).
Causes of cholecystitis
Inflammation of the walls of the gallbladder occurs for various reasons.
Basically, the provoking factor is considered to be the presence of stones in the cavity of the bladder. Like any other organ in the human body, the liver performs many functions, one of which is the synthesis of cholesterol. After formation, cholesterol enters the bile solution, which consists of various substances, including acids, bilirubin, water, etc.
If the balance of bile acids and cholesterol is disturbed in one direction or another, crystalline stones form, which attach to the inner walls of the bile ducts. As a result, the outflow of bile is blocked and it begins to accumulate in the bladder cavity, which causes the development of an inflammatory process.
If therapeutic measures are not taken when this pathology appears, an infection can develop in the cavity of the bladder and lead to unimaginable consequences. This type of cholecystitis is called stone cholecystitis.
In addition to stone cholecystitis, there is another - stoneless. It occurs due to:
- penetration of bacteria or infections into the cavity of the gallbladder: typhoid fever, salmonella, etc.;
- after surgery or injury to the digestive organs;
- due to severe burns;
- with a tendency to constipation; with improper functioning of the immune system;
- if the patient leads a sedentary lifestyle;
- for endocrine diseases.
Moreover, there are a number of accompanying factors that can become serious provocateurs of cholecystitis:
- dysconesia of the biliary tract - uneven output of bile. This pathology is not considered dangerous, but it can provoke the appearance of stones in the cavity of the bladder, which, in turn, will lead to cholecystitis;
- gastritis, in which there is low acidity;
- circulatory disorder in the area of the bladder walls.
Diagnostics
Competent treatment prescription depends on diagnostic measures. First of all, the specialist conducts a conversation with the patient, during which he learns about all the symptoms that bother him. Then the study is scheduled.
Lab tests
A complete blood count is considered very important, as it can help determine the level of white blood cells. Increased leukocytosis is an indicator that there is an infection in the body, however, this nuance is not considered an indicator of cholecystitis.
At the next stage of the examination, blood biochemistry is prescribed, during which much attention is paid to the amount of bilirubin in it. Bilirubin is an indicator of the proper functioning of the liver and gallbladder. In an absolutely healthy person, its level can vary from 3.4 to 17.1 µmol/l. However, if the patient suffers from a bile outflow disorder or liver disease, this figure will be much higher.
An increase in bilirubin levels is observed not only in the patient’s blood, but also in his biological fluid and feces, so urine and stool tests will confirm the suspicion of cholecystitis.
Also, to identify liver problems, the patient will be prescribed a liver test. This type of diagnosis is considered mandatory and allows you to determine:
- the type of bilirubin in the blood, as well as its amount;
- the level of other enzymes contained in the blood.