Ectopic ureter is an anomaly in the topography of the ureter, in which the orifice is not located in a typical manner. This is a congenital disease. This disease occurs quite often, it is divided into: intravesical and extravesical. There is a risk of developing pyelonephritis. During an extravesical location, a person's urethra may leak after visiting the toilet.
You should immediately seek help from specialists, conduct a diagnosis and begin treatment. The disease has several subtypes, so the treatment for each of them is significantly different. The disease is congenital and manifests itself in childhood. Both women and men are at risk. Women suffer from ectopia several times more often.
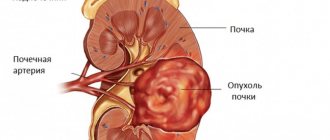
The tubes that connect the renal pelvis and bladder are called the ureter. The kidneys contain filtered fluid. At the entrance to the kidney, the ureter has a check valve that prevents the backflow of urine into the kidney. At the other end, the ureter connects the kidney to the bladder. In the normal anatomical position, the ureteral orifices resemble Lieto's triangle, the three sides of which are: the ureteral orifices and the urethra in the center.
With various disorders, the ureter extends beyond the connection in the triangle, or does not connect to them at all. The mouth opens into the intestines or genitals of a man or woman. The pathology always occurs with the presence of an extra ectopic ureter and renal pelvis. The ureter begins to change its development.
Along the entire length of the hollow tube of the ureter, other organs are adjacent to it. If the renal pelvis is enlarged, then the ureter is attached below the vessels, and if it is reduced, then behind the vessels. A blood vessel coming from the lower part of the renal conus crosses the ureter. Below it intersects with the femoral nerve and the psoas muscle. The right tube is located under the inferior vena cava, colon and colon, and the left tube is located under the abdominal aorta and colon.
general information
Ectopic ureter is associated with an abnormal location of the orifices of the internal organ, which can be located in the extravesical or intravesical region. In this case, the mouth is often included in the uterus, vagina, urethra or other nearby organs. Often, along with ectopia of the ureteric orifice, duplication of the organ and pelvis is detected.
In rare cases, ectopia of the main or solitary ureter is observed. As a rule, doctors observe an ectopic ureter, which is connected to the pelvis located above.
This phenomenon is congenital and makes itself felt a short time after birth. The pathology is predominantly diagnosed in the fairer sex; in men, the deviation is extremely rare. Thus, the pathological process manifests itself differently in both sexes and differs in location.
Varieties
The pathology affects one or two kidneys.
There are several classifications of the pathological process, in which the symptoms and treatment will differ. Considering the localization of the mouth of the internal organ, ectopia can be intestinal, uterine, vaginal, hymenal, vestibular or paraurethral. The pathology can be unilateral or bilateral. In the first case, one internal organ is affected. With bilateral pathology, two kidneys are damaged. Symptoms will appear depending on the type of abnormal phenomenon. Treatment depends on both the type and the severity of the disease. There are also such forms of ectopia:
- intravesical;
- extravesical.
With intravesical ectopia, the ureter is located in an atypical place of the ureter. In this case, the patient develops either pyelonephritis. If extravesical ectopia of the ureteric orifice is diagnosed, then in men the excretory duct enters the posterior urethra, seminal tubercle or vesicles. Often the orifices are attached to the prostate gland or vas deferens. In women, the orifice of the ureter joins the vagina, uterine body, urethra, or cervix. With such a deviation, the patient experiences urine leakage, but the urinary process is not disrupted.
Main reasons
Ectopic ureteral orifice is one of the congenital anomalies.
Pathology develops, as a rule, during the intrauterine formation of the fetus. The entire ureter is formed during the 3-8th weeks of pregnancy. Due to a woman’s somatic illnesses or under the influence of medications during pregnancy, anomalies occur during the formation process that affect the normal development of the system. In some cases, a hereditary factor plays a role. As a result, the ureteric orifices are not attached to the bladder, but remain attached to the primary kidney. Thus, ectopia of the ureters is provoked.
Then the formation of the vagina, uterus and tubes (in girls) occurs, in which the orifices are located in one of these organs. Sometimes the mouth extends into the urethra or the neck of the bladder. Typically, in women, the ureteral orifice is located behind the urinary system, which leads to leakage of urine.
In the male body, during the formation of the epididymis, seminal vesicles, and vas deferens, the ureteric tubes are attached to one of these structures. But due to the fact that men have an anatomically different urinary system, they do not leak urine. Often in both sexes the pathology is observed together with other renal pathologies, namely polycystic disease, ureterocele, duplication of internal organs and others.
Causes of urinary incontinence in dogs
Recently, the number of diseases of the urinary system in pets has increased greatly.
Urinary incontinence in dogs is one of the unpleasant problems that owners sometimes have to deal with in their pets. Impaired urination in the form of incontinence brings serious physiological problems to animals and everyday problems to humans. Urinary incontinence is the involuntary (uncontrollable) leakage of urine from the urethra. Urinary incontinence can be constant and intermittent, depending or not depending on the time of day and emotional state.
The main causes of urinary incontinence in bitches are:
- cystitis,
- ectopia of the ureters,
- complication after sterilization,
- neurological disorders,
- calculi (stones) of the bladder,
- renal failure,
- diabetes mellitus, etc.
The emotional factor is mainly found in young animals up to 3-4 months.
Difference between ectopic ureteric orifices in men and women
This pathology occurs much more often in girls, and much less often in boys.
Doctors have noticed that this problem is diagnosed 3-4 times more often in the fairer sex. If a man encounters a deviation, usually such an anomaly is independent (primary). When the female body is affected, ectopia and a double ureter are diagnosed simultaneously. Leakage of urine is typical for women, but this symptom is not observed in men, so they do not always seek help. This fact is explained by the different structure of the urinary system. In the female body, the opening of the internal organ is located below the urethral sphincter, so urine flows out. In most men, the mouth of the internal organ flows into the prostate gland, and ectopia with outlet into the ejaculatory duct is extremely rare. In representatives of the fairer sex, the pathological process occurs in the urethra, and in a smaller part, the mouth of the ureter is located in the uterus.
Prevention of ureteral ectopia in dogs
There is no way (that is 100% guaranteed) to prevent ureteral ectopia in pet dogs. There is an opinion among veterinarians and breeders that it is necessary to limit the breeding of dogs with this anomaly, but the problem has been poorly studied. Many people believe that dogs with this defect should be spayed or neutered.
Page 5 of 22
The anomaly is that the orifice of the ureter ends in the urinary tract distal to its usual place or is localized in various parts of the genital organs. An ectopic ureter can be single and drain an ontogenetically normally developed kidney, but more often ectopia is accompanied by duplication of the pelvis and ureter. Usually the ureter of the upper pelvis is ectopic. There are cases of bilateral ectopia or ectopia of both ureters on the same side. Ectopic ureters in girls are 3-4 times more common than in boys. Based on the anatomical location and characteristics of the clinical manifestation of ectopia in girls, the following anomalies are distinguished.
Symptoms
The surest sign of a pathological process in girls and women is the release of urine, which is difficult to control. But there is no disturbance during urination. Urine is released especially often during intense physical activity, during a change of position or when moving. Often the patient complains of the following symptoms that indicate ectopia of the ureteral orifices:
- vaginal discharge;
- inflammatory processes in the internal genital organ;
- pain in the abdominal area;
- lumbar pain;
- inflammation of the epithelial layer of the perineum.
The most pronounced sign of pathology in men is pyelonephritis.
Representatives of the stronger sex experience pyelonephritis, which tends to recur. The patient complains of dull pain in the lumbar region and abdomen. Purulent discharge is often observed during urination. The process of urine excretion becomes more frequent. If the mouth flows into the epididymis, then an inflammatory process of this organ occurs and symptoms characteristic of the pathology appear. In some cases, there is vague pain that is localized in the pelvis and perineum. Over a long period of time, the pathology leads to infertility and impaired ejaculation.
The pathology is accompanied by hydronephrosis.
Often, against the background of ectopia of the right or left ureter, various infectious lesions of the urinary system occur. In most cases, ectopia of the orifices is accompanied by ureterocele, in which blockage of the ureters occurs, which leads to stagnation of urine. If the pathology is not detected in a timely manner and treated, then renal failure develops with all the ensuing symptoms.
Diagnostics
For a detailed examination of the urinary system, the ultrasound diagnostic method is used.
In case of ectopia of the ureteric orifices, a comprehensive diagnosis is necessary, consisting of instrumental and laboratory studies. First of all, the doctor is interested in the present symptoms that are observed in the patient. Then the patient is examined, after which diagnostic measures are prescribed. First of all, you should undergo ultrasound diagnostics of the kidneys and organs of the urinary system.
Effective diagnostic methods are urethroscopy and cystoscopy. With cystoscopy, it is possible to determine the pathology in which the openings of the accessory ureter are not found in the urinary triangle. Urethroscopy allows you to determine the ectopia of the orifice and its degree. In most cases, the patient undergoes excretory urography, which reveals a double kidney or ureter. Using ascending urethrography, the location of the ureter is determined.
To make a diagnosis, a color test is used using indigo carmine, which is injected into the bladder through a catheter. If urine leaks through the catheter, this indicates ectopia. Computed tomography is used to determine the location of the dysfunctional kidney. Using voiding cystourethrography, you can find out where the ureter joins the bladder. The method determines the presence of vesicoureteral reflux.
A general blood test is the basis for diagnosing most known diseases.
Laboratory diagnostic methods are also important, especially when pyelonephritis is suspected. In this case, a complete blood count will indicate a significant presence of leukocytes and bacteria. Bacteriological culture is prescribed to determine the causative agent of the infection. Another method for studying infectious injury is a smear from the urethra.
Ectopic ureter in girls usually manifests as a urinary tract infection if the ostium is located proximal to the urethral sphincter, or urinary incontinence if it is located outside the sphincter. Figure 51-7 shows a duplication of the ureter with ectopia in the vestibule of the vagina. Depending on the amount of renal parenchyma, the nature of urinary incontinence varies.
Rice. 51-7. Scheme of a typical ectopic ureter. The orifice of the lower ureter is located normally. When removing an ectopic ureter that enters the bladder distal to the external urinary sphincter, great care must be taken not to damage the sphincter.
If a small amount of urine is produced, then incontinence may be intermittent only when the child is standing, and in such cases sometimes a diagnostic error occurs, because the incontinence is regarded as functional (stress). Excretory urography may reveal delayed renal function if sufficient renal parenchyma is present.
However, in most cases of extravesical ectopia of the ureters, the upper segment of the kidney is “silent”. Figure 51-8 shows a patient with ectopic ureter. Excretory urography did not allow a diagnosis to be made (Fig. 51-8A). No reflux was detected during voiding cystography. On cystoscopy, the ectopic orifice was located distal to the bladder neck.
Retrograde pyelography showed the changes shown in Figure 51-8B. Currently, with the widespread use of modern ultrasound diagnostic methods, the detection using these methods of a “silent” dilated upper segment of the kidney should, with an appropriate clinical picture, suggest ectopia of the ureter.
Rice. 51-8. Ectopic ureter. A, Excretory urogram - complete doubling on the right and a small, normal-looking left kidney. B, A bilateral retrograde pyelogram revealed a “silent” upper pole of the left kidney.
The following symptoms on excretory urograms may indicate ectopia of the ureter: the presence of duplication of the urinary tract on the opposite side (see Fig. 51-8); asymmetry of cups on both sides; the location of the upper pole of the kidney on the affected side is higher than it should be; “fading flower” - a downward and somewhat lateral displacement of the lower, often deformed cavity system. When upper segment function decreases, it may enhance on delayed images, but late visualization of the upper segment is sometimes due to reflux.
If the ureteral orifice is located at or distal to the bladder neck, reflux may not occur when the bladder is full, but may occur during voiding. In rare cases, the dilated upper ureter puts pressure on the lower one, causing its obstruction, which sometimes results in atrophy or pyelonephritic scar changes. Micture cystourethrography may show reflux into the ectopic ureter, into the ipsilateral lower ureter, or, in rare cases, into both ureters.
An ectopic ureter can be detected during examination of the perineum, during cystoscopy, or during vaginoscopy. Sometimes, however, finding its mouth can be quite difficult. In such cases, even if the function of the upper segment of the kidney is reduced, intravenous administration of indigo carmine helps. In the presence of a single (non-duplicated) ectopic ureter, the most informative diagnostic methods are currently ultrasound examination and computed tomography.
As soon as the diagnosis is confirmed, surgical treatment is immediately carried out according to the same principles as for duplication of the ureters. It is especially necessary to follow these principles in cases where ectopia is combined with doubling and localization of the ureteric orifice proximal to the external urinary sphincter.
One of two types of surgical interventions is used: reimplantation of a double ureter as a single complex or upper heminephrureterectomy with reimplantation of the lower ureter. In boys with ureteric ectopia into the reproductive tract, the ureter is usually not doubled, and the renal parenchyma is sharply reduced in volume. In such cases, it is most advisable to perform nephroureterectomy.
In girls, where the ureter passes through the external urinary sphincter, great care must be taken not to damage the bladder sphincter. Catheterization of the orifices of both normal and ectopic ureters and expansion of the latter by injecting physiological or dyeing solution into it makes it possible to identify the course of the ureters behind the bladder.
The ureters should be severed very carefully to preserve blood supply to the lower ureter. The distal part of the ectopic ureter is isolated behind the bladder to the level of the neck and external urinary sphincter, where the ureter is ligated. If possible, the mucosal lining of this remaining stump should be removed to allow suturing of the orifice.
The proximal part of the ectopic ureter is removed along with the dysplastic and atrophied upper segment of the kidney from a separate lateral incision. In those rare cases when the upper segment has functioning parenchyma, it is advisable to perform a ureteropyelostomy or ureteroureterostomy, anastomosing the upper ureter with the lower pelvis or with the lower ureter.
In infants, superior heminephrectomy and ureterectomy through one lateral incision are preferred, leaving the lower part of the ectopic ureter. As the child gets older, if there is a recurrent infection indicating that the remnants of the ureter are functioning as a diverticulum, a final operation is performed - removal of the distal part of the ectopic ureter.
K.U. Ashcraft, T.M. Holder
Ectopic ureteral orifice is an abnormal location of one or both ureteral orifices in the bladder or extravesically. Until 1965, 101 observations of this malformation were described in the domestic literature. Currently, the number of publications describing the abnormal location of the ureteral opening has increased significantly. This is due to improved diagnosis of ureteral ectopia.
D. D. Murvanidze et al. (1978) diagnosed ectopic ureteral orifice in 1 child out of 750 children with diseases of the urinary system. A. L. Axelford (1964) identified this anomaly in children with a frequency of 1: 1600 autopsies. Often this malformation is combined with duplication of the ureters. An opening related to the ureter of the upper or lower half of the kidney can be ectopic. Typically, the ureter draining the superior pelvis opens at a lower level in the urinary tract than the ureter draining the inferior pelvis. The opening of the ureter of a congenitally single kidney may be ectopic.
The malformation is much more common in girls. The literature provides the following ratios of the frequency of this anomaly in men and women - 1: 3, 1: 4, 1: 5. According to K. Blundon, J. Lane (1960), urinary incontinence in girls in 75% of cases is caused by ectopic opening of the ureter . We also received similar data.
E. M. Shimkus and co-authors (1976) describe 11 observations of ureteral ectopia in girls, A. Ya-Pytel, A. G. Pugachev (1977) - 18, D. D. Murvanidze and co-authors (1978) - 6, E. A. Ostropolskaya and co-authors (1979) - 49, S. Ya. Doletsky and co-authors (1979) -32. E. A. Ostropolskaya and co-authors described ectopia of the ureter in 1 boy. This rarity of diagnosis of anomaly in boys can be partly explained by the rarer detection of the main symptom of this anomaly (urinary incontinence). In boys, the ectopic opening of the ureter is always proximal to the external sphincter and is not accompanied by urinary incontinence.
The opening of the ectopic ureter most often opens into the urethra (or near its opening), rectum, vestibule or fornix of the vagina, cervix or body of the uterus, vas deferens, etc.
There are many classifications of ectopia of the ureteral orifice, but the most convenient classification is Yu. G. Ediny (1953), who divides all types of ectopic ureteral orifice into two groups:
1) the ectopic opening of the ureter opens into the derivatives of the urogenital sinus (cervicovesical, urethral and paraurethral ectopia, vestibular ectopia);
2) the ectopic opening of the ureter opens into the derivatives of the ductus paramesonephricus and the intestinal tube (vaginal, uterine and intestinal ectopia).
A. Ya. Pytel (1968) considers it necessary to add to this classification the terms “ectopia of the opening of the main ureter” without doubling the upper urinary tract and “ectopia of the opening of the accessory ureter.”
The location of the ureteral opening in the bladder more lateral, below its typical location, is relatively common. This localization in most cases is combined with vesicoureteral reflux, ureterocele, and refluxing megaloureter. The frequency of detection of lateral ectopia of the ureteral orifice in vesicoureteral reflux has led to the assumption of a pathogenetic connection between ectopia and reflux. Intravesical types of ectopia of the ureteral orifice include displacement of the ureteral orifice into the neck of the bladder or the posterior part of the urethra. These types of developmental defects are not always diagnosed, since the main symptom – urinary incontinence – is not observed.
Intravesical types of ureteral ectopia are often complicated by pyelonephritis, as they cause disturbances in urodynamics. Fixation of the opening lateral to or below the genitourinary triangle leads to underdevelopment of the antireflux mechanism, disruption of the closure of the opening, and subsequently to the development of ureterohydronephrosis on the corresponding side. Cervical ectopia and displacement of the ureteral opening to the posterior part of the urethra in boys are usually accompanied by compression or narrowing of the intramural portion of the ureter with the subsequent development of ureterohydronephrosis and pyelonephritis. The manifestations of this type of abnormality of the ureteral orifices depend on the clinical course of complications (pain, dysuria, fever, pyuria, etc.). When children are examined for the listed complaints, a developmental defect is diagnosed. Since the diagnosis is made only in cases where the abnormal opening leads to disruption of urodynamics, treatment must be surgical. The operation of choice is numerous options for neocystoureterostomy with antireflux protection.
More striking clinical manifestations are characteristic of extravesical variants of ectopic ureteral orifice.
is a congenital anomaly of the topography of the ureter, consisting in an atypical intravesical or extravesical location of its mouth. With extravesical ectopia, there is involuntary leakage of urine against the background of intact urination; intravesical types of anomalies are accompanied by the development of pyelonephritis and ureterohydronephrosis. Diagnostics may include ultrasound, cystoscopy and urethroscopy, excretory urography, cystography, ureteropyelography, renal angiography, gynecological examination in women, sigmoidoscopy. If renal function is preserved, ureteroureteroanastomosis or ureteropyeloanastomosis is performed. If kidney function is lost, partial or total nephroureterectomy is indicated.
Urethral ectopia.
With such an anomaly, the orifice of the ureter is located in the urethra distal to the voluntary sphincter. A characteristic clinical feature of this type of anomaly is the constant and not consciously controlled release of urine from the urethra with simultaneous normal urination. Often in the first year of life, due attention is not paid to the constant urinary incontinence of such a child. In the future, constant urinary incontinence is sometimes mistakenly regarded as a functional weakness of the sphincter of the bladder, enuresis of central origin, etc. It is especially difficult to recognize cases in which urine excretion occurs during the day with an upright position of the body or only during sleep when the muscles of the perineum are relaxed, which is erroneous is regarded as nocturnal enuresis.
Vaginal and vestibular ectopia are clinically no different from urethral ectopia. The orifice of the ureter may be located in the vestibule of the vagina. More often it is located on the anterior wall of the vagina closer to the midline, on the side wall or on the cervix.
With ectopic ureters in boys, the orifice can be localized in the prostatic urethra, in the seminal vesicles and, less commonly, in the vas deferens and ejaculatory ducts. Since the orifice is proximal to the sphincter, ectopia is not accompanied by urinary incontinence.
The unusual localization of the orifice leads to a complete disruption of the outflow of urine from the kidney, and the child develops severe ureterohydronephrosis even before birth. Subsequently, the addition of infection is accompanied by a clinical picture characteristic of infected hydronephrosis and pyelonephritis. The nature of urinary incontinence caused by vaginal or urethral ectopia can be easily determined by examining the child’s genitals. The discharge of small amounts of uncolored urine from the urethra or vagina after preliminary administration of a methylene blue solution into the bladder undoubtedly indicates ectopic ureteric orifice and excludes the possibility of congenital vesicovaginal fistula and weakness of the vesical sphincter. However, the main task of diagnosis is not so much to identify the localization of the ectopic mouth, but to find out on which side the pelvis is located, to which the ectopic ureter belongs. Often, when a kidney is doubled, this is difficult, since catheterization of the ectopic orifice is often impossible, and a sharp decrease in the functional capacity of the parenchyma related to the upper pelvis does not allow it to be detected on intravenous urograms. In such cases, recognition of a double kidney is based on catheterization of the orifices that normally open in the bladder and retrograde ureteropyelography. Identification of the inferior pelvis by a number of its inherent radiological signs (absence of the superior horn, small number of cups, low location, outward displacement, etc.) with a normal opposite kidney allows one to accurately localize the side where the double pelvis is located. In some cases, signs of bilateral duplication of the pelvis are revealed when there are only two normally located orifices in the bladder. If in such a condition there are no signs of merging ureters (ureter fissus) on one side, this indicates ectopia of both ureters of the upper pelvis. With data confirming the absence of kidney duplication, one must remember the possibility of vaginal ectopia of one of the branches with caudal bifurcation of the ureter or ectopia of the ureter of the third accessory kidney. Treatment
. The method of choice in the treatment of urinary incontinence and infected ureterohydronephrosis caused by ectopic ureter of a double kidney is resection of its upper half along with the ureter. In cases of ectopic ureter of the non-duplicated pelvis, the nature of the surgical treatment is determined by the degree of secondary changes in the kidney. With moderate dilatation of the ureter and preserved kidney function, neoimplantation of the ureter into the bladder is indicated. If there is a sharp decrease in kidney function as a result of advanced hydronephrosis, nephrectomy is recommended.
Ectopic ureteral orifice is an abnormal location of one or both ureteral orifices in the bladder or extravesically. Until 1965, 101 observations of this malformation were described in the domestic literature. Currently, the number of publications describing the abnormal location of the ureteral opening has increased significantly. This is due to improved diagnosis of ureteral ectopia.
D. D. Murvanidze et al. (1978) diagnosed ectopic ureteral orifice in 1 child out of 750 children with diseases of the urinary system. A. L. Axelford (1964) identified this anomaly in children with a frequency of 1: 1600 autopsies. Often this malformation is combined with duplication of the ureters. An opening related to the ureter of the upper or lower half of the kidney can be ectopic. Typically, the ureter draining the superior pelvis opens at a lower level in the urinary tract than the ureter draining the inferior pelvis. The opening of the ureter of a congenitally single kidney may be ectopic.
The malformation is much more common in girls. The literature provides the following ratios of the frequency of this anomaly in men and women - 1: 3, 1: 4, 1: 5. According to K. Blundon, J. Lane (1960), urinary incontinence in girls in 75% of cases is caused by ectopic opening of the ureter . We also received similar data.
E. M. Shimkus and co-authors (1976) describe 11 observations of ureteral ectopia in girls, A. Ya-Pytel, A. G. Pugachev (1977) - 18, D. D. Murvanidze and co-authors (1978) - 6, E. A. Ostropolskaya and co-authors (1979) - 49, S. Ya. Doletsky and co-authors (1979) -32. E. A. Ostropolskaya and co-authors described ectopia of the ureter in 1 boy. This rarity of diagnosis of anomaly in boys can be partly explained by the rarer detection of the main symptom of this anomaly (urinary incontinence). In boys, the ectopic opening of the ureter is always proximal to the external sphincter and is not accompanied by urinary incontinence.
The opening of the ectopic ureter most often opens into the urethra (or near its opening), rectum, vestibule or fornix of the vagina, cervix or body of the uterus, vas deferens, etc.
There are many classifications of ectopia of the ureteral orifice, but the most convenient classification is Yu. G. Ediny (1953), who divides all types of ectopic ureteral orifice into two groups:
1) the ectopic opening of the ureter opens into the derivatives of the urogenital sinus (cervicovesical, urethral and paraurethral ectopia, vestibular ectopia);
2) the ectopic opening of the ureter opens into the derivatives of the ductus paramesonephricus and the intestinal tube (vaginal, uterine and intestinal ectopia).
A. Ya. Pytel (1968) considers it necessary to add to this classification the terms “ectopia of the opening of the main ureter” without doubling the upper urinary tract and “ectopia of the opening of the accessory ureter.”
The location of the ureteral opening in the bladder more lateral, below its typical location, is relatively common. This localization in most cases is combined with vesicoureteral reflux, ureterocele, and refluxing megaloureter. The frequency of detection of lateral ectopia of the ureteral orifice in vesicoureteral reflux has led to the assumption of a pathogenetic connection between ectopia and reflux. Intravesical types of ectopia of the ureteral orifice include displacement of the ureteral orifice into the neck of the bladder or the posterior part of the urethra. These types of developmental defects are not always diagnosed, since the main symptom – urinary incontinence – is not observed.
Intravesical types of ureteral ectopia are often complicated by pyelonephritis, as they cause disturbances in urodynamics. Fixation of the opening lateral to or below the genitourinary triangle leads to underdevelopment of the antireflux mechanism, disruption of the closure of the opening, and subsequently to the development of ureterohydronephrosis on the corresponding side. Cervical ectopia and displacement of the ureteral opening to the posterior part of the urethra in boys are usually accompanied by compression or narrowing of the intramural portion of the ureter with the subsequent development of ureterohydronephrosis and pyelonephritis. The manifestations of this type of abnormality of the ureteral orifices depend on the clinical course of complications (pain, dysuria, fever, pyuria, etc.). When children are examined for the listed complaints, a developmental defect is diagnosed. Since the diagnosis is made only in cases where the abnormal opening leads to disruption of urodynamics, treatment must be surgical. The operation of choice is numerous options for neocystoureterostomy with antireflux protection.
More striking clinical manifestations are characteristic of extravesical variants of ectopic ureteral orifice.
- This is a rare congenital abnormality of the genitourinary system in which one or both ureters exit into the urethra or vagina without passing through the bladder, and is one of the most common causes of urinary incontinence in young animals.
Normally, urine is formed in the kidneys and released through the ureters into the bladder, where it accumulates to a certain volume, and then is released out through the urethra during the act of urination, that is, periodically. With this pathology, the ureters pass past the bladder and open lower, into the urethra (in males) or the vagina (in females). Most of the urine continuously flows out, and only a small part enters the bladder through reverse movement.
Since ectopic ureter is a congenital disease, symptoms appear from birth. This pathology is more common in females than in males. Among the clinical signs, urinary incontinence is noted in the form of continuous leakage, sometimes with short breaks (the further in the caudal direction the orifice of the ureter is, the greater the tendency to constant incontinence). An important sign of ureteral ectopia is the release of urine at a time when the animal is not urinating - during sleep, while eating, during play.
But, it should be taken into account that ectopia of the ureters is not only an aesthetic problem. Ectopic ureters quickly expand, which gives rise to the development of pathogenic microflora. Subsequently, urethritis and hydronephrosis occur, which leads to the death of the animal.
In most cases, it is possible to confirm the diagnosis by combining pneumocystography with excretory urography. In cases where radiography does not reveal the correct diagnosis, and other causes of incontinence are unlikely, the diagnosis should be made surgically, by exploratory laparotomy.
Treatment involves surgical reimplantation of the displaced ureter into the bladder and treatment of the urinary tract infection. A timely operation makes the dog completely healthy; it takes several weeks to several months to restore normal urination.
As an example, below is a clinical case from our practice.
Anamnesis:
The owners of a female Labrador retriever aged 6 months came to the clinic with complaints that the dog had been suffering from urinary incontinence since 3 weeks of age. At the moment, a diagnosis of urocystitis was made. Medications taken: at the moment - no, during previous treatment - antibacterial drugs of various groups, in particular: ceftriaxone, sinulox, nitroxaline. The general condition is satisfactory, the appetite is good, the stool is regular and formed.
Clinical examination:
Consciousness and behavior are normal. Temperature 38.4 °C. When examining the fur in the area of the vulva, the inner surface of the thighs is discolored, urine is constantly released from the vagina. The abdomen is soft, painless, and not enlarged in volume. The bladder is not palpable. The vaginal mucosa is hyperemic; a vaginal examination did not reveal any pathologies. Neurological examination - no pathologies were identified.
Laboratory research:
A clinical blood test showed a sluggish inflammatory reaction. The biochemical blood test revealed no abnormalities. A urine test indicated an inflammatory process in the kidneys and bladder. Based on the above data, ureteral ectopia was suspected. To confirm the diagnosis, special diagnostics were carried out.
RTG:
An overview image revealed no pathologies of the bladder and ureters. By combining pneumocystography with excretory urography, a caudal displacement of the ureteric orifices was revealed. The left ureter is dilated, the contours of the left kidney are enlarged. Conclusion: ectopia of the ureters.
Ultrasound:
the left kidney is drooped, enlarged in size approximately 8.7x4.5 cm. The pelvis and proximal ureter are dilated, there is a moderate increase in the echogenicity of the parenchyma. The bladder is poorly filled. The remaining organs are without pronounced pathologies.
Conclusion:
hydronephrosis of the left kidney.
Diagnosis:
ectopia of the ureteric orifices, left-sided hydronephrosis.
Treatment:
Laparotomy revealed bilateral ureteral reflux, the lumen of the ureters was increased to 1 cm. The bladder was collapsed, the left kidney was enlarged. The ureters pass along the wall of the bladder into the pelvic cavity.
A ventral cystotomy was performed from the apex to the neck of the bladder. Somewhat distal to the intended orifices of the ureters, two longitudinal incisions 5-7 mm long were made, and the mucous membrane of the ureters was sutured to the mucous membrane of the bladder with interrupted sutures. Urine flow into the bladder was noted. A continuous suture was placed on the bladder wound.
After surgery, the animal received Sinulox at a dose of 12.5 mg/kg 2 times a day for 3 weeks. 1.5 months after the operation, voluntary urination was restored. 2 weeks after the operation, according to the results of ultrasound, the condition of the left kidney improved significantly. Cystoscopy one month after surgery confirmed the normal functioning of the ureters and bladder.
General information
With ectopic ureter, its mouth may open distal to the angle of Lieto's triangle or flow into adjacent organs (urethra, vagina, uterus, intestines, seminal vesicles). The pathology in most cases is combined with complete doubling of the ureter and pelvis, while the ectopic, as a rule, is the ureter connecting to the upper pelvis. Less common is the incorrect location of the base of the solitary or main ureter. Ectopic ostium is a congenital anomaly of the ureter, which manifests itself already in childhood. In practical urology, this malformation is detected 4 times more often in girls than in boys.
Anatomical certificate
The ureters are tubes connecting the renal pelvis and bladder. The renal pelvis is a reservoir that receives fluid filtered by the kidneys. At their exit, the ureters have a sphincter that prevents urine from flowing back into the kidney. The other end of the ureter connects to the bottom of the bladder.
Normally, the orifices of the ureters and urethra form Lieto's triangle. Its apex is the beginning of the urethra, and the corners of the base are the orifices of the ureters. With ectopia, the ureter connects to the bladder outside this triangle or does not communicate with it at all. An anomaly is the opening of the mouth into the urethra, intestines or genitals.
The pathology is almost always accompanied by the presence of an extra renal pelvis and an additional ectopic ureter. The ureter coming from the superior duplex pelvis receives abnormal development.
Causes
The development of the urogenital system during embryogenesis occurs between the 3rd and 8th weeks of gestation. Initially, the ureteric primordia are formed from mesodermal ducts proximal to the area of their future location. Gradually they migrate downwards to enter the posterior wall of the bladder in a typical location. Under the influence of teratogens (somatic diseases of the pregnant woman, occupational hazards, medication, hereditary factors and other adverse effects), the orifices of the ureters are not promptly implanted into the bladder, remaining in the rudiments of the mesonephric duct.
Subsequently, the vagina, uterus and fallopian tubes are formed from the paramesonephric ducts in girls, so the ureter ends up opening into one of these structures, or derivatives of the urogenital sinus - the bladder lateral to Lieto’s triangle, the urethra, the bladder neck, and the paraurethral region. All variants of ectopia in women are found either outside the urinary system or below the level of the external sphincter of the bladder, which is clinically manifested by drip leakage of urine.
From the mesonephric buds in men, the epididymis, seminal vesicles and vas deferens develop, and the ectopic ureter, as a rule, opens into these structures. However, since these anatomical structures are located proximal to the external sphincter of the bladder, ectopic ureter in men is never accompanied by urinary incontinence. The pathology is often combined with doubling of the kidney and ureter, ureterocele, kidney dystopia, hypoplasia and polycystic kidneys and other congenital anomalies.
Classification
Ectopy of the base of the ureter can be unilateral or bilateral, intravesical (intravesical) or extravesical (extravesical). The intravesical ectopic ureter opens in an atypical location of the bladder. The extravesical ectopic ureter in women can empty into the vaginal vestibule, urethra, vagina, cervix or uterine body; in men - into the posterior urethra, seminal vesicles, seminal tubercle, vas deferens, prostate or epididymis.
Depending on the location of the ureteric orifice, cervicovesical, urethral, paraurethral (vestibular), hymenal, vaginal, uterine, intestinal and other types of ectopia are distinguished. The type of pathology determines the characteristics of clinical manifestations, diagnosis and treatment tactics for a given defect.
Symptoms
A pathognomonic sign of extravesical ectopia of the base of the ureter in girls and women is constant uncontrolled drip of urine with intact normal urination. Increased involuntary urine output is observed with movements, changes in body position, and physical activity. In addition, there may be discharge from the genital tract, vulvitis and colpitis, pain in the abdomen and lower back, inflammation of the skin of the perineum due to constant contact with urine (urinary dermatitis).
In boys and men, ectopia in the prostatic urethra is manifested by recurrent pyelonephritis, dull pain in the lower back and abdomen, pyuria, urgency and frequent urination. When the ectopic ureter flows into the epididymis, a clinical picture of epididymitis may develop. Also, the disease in men is characterized by vague pain in the perineum and pelvic area, discomfort during ejaculation, constipation, infertility, asymmetry of the scrotum or abdomen, palpable formation in the abdomen or lumbar region. The presence of vesicoureteral reflux causes the gradual development of hydronephrosis.
Clinical picture of ureteral ectopia
Depending on the type of ectopia of the ureteral orifice, it manifests itself with different signs. Symptoms in girls differ from those that accompany pathology in boys.
In girls, the cervical and paraurethral location of the orifice causes urine leakage. At the same time, normal urination is maintained. Urine leaks from the double ureter, since it has practically no muscle tissue and is characterized by atony. Typically, this form of anomaly is diagnosed almost immediately after birth.
Signs that the ostium is located outside the bladder may appear in children, adolescents, and adults.
In women, the following symptoms indicate it:
- leakage of urine, especially during physical exertion;
- irritation of the skin surface and itching in the perineum caused by exposure to urine;
- constant vaginal discharge, often purulent, which can be mistaken for vulvovaginitis and vaginal dysbiosis;
- lumbar pain and in the abdominal area at the connection of the ureter to the uterus;
- Possible menstrual irregularities.
Symptoms characteristic of pyelonephritis appear, but without specific changes in urine. In men, ectopia is not accompanied by incontinence due to the structure of the genitourinary system, so diagnosing the anomaly in them is more difficult.
To prescribe an examination, we are guided by the following signs:
- painful, incomplete or untimely urination;
- pus in the urine;
- pain during bowel movements;
- pain in the testicles;
- feeling of discomfort during ejaculation in men.
If the orifice of the ureter extends into the epididymis, symptoms of epididymitis appear. Men may experience prolonged constipation and may develop infertility. The scrotum has an asymmetrical shape.
Intestinal ectopia is expressed by recurrent pyelonephritis due to intestinal microflora entering the ureter and kidney. Possible stool upset and abdominal pain in children and adults.
When the orifice of the ureter is located above the neck of the bladder or in the posterior urethra, there are no symptoms or external signs.
One of the diagnostic signs of intravesical ectopia in boys and girls is the development of pyelonephritis and hydronephrosis (enlargement of the renal pelvis).
Diagnostics
An examination for suspected ectopia of the base of the ureter includes collection of complaints, examination of the patient, ultrasound of the kidneys and bladder, urethroscopy and cystoscopy, excretory urography, cystography, ascending urethrography. To identify complications and assess kidney function, scintigraphy, renal angiography, CT, and MRI are required. A comprehensive echographic, endoscopic, and x-ray examination of the urinary system allows us to detect anatomical anomalies of the kidneys and ureters - dystopia, duplication, ectopia; assess the condition of the pyelocaliceal system.
Paraurethral ectopia is easily accessible to external examination and is not difficult to diagnose. The vaginal location of the orifice in women can be detected during gynecological examination and colposcopy with catheterization of the ectopic ureter. Uterine ectopia is more difficult to diagnose, requiring ultrasound of the pelvic organs, hysteroscopy, and sometimes diagnostic laparoscopy.
In men, digital examination of the rectum and urethroscopy are mandatory. Rare cases of intestinal location of the base of the ureter can be detected by sigmoidoscopy. Laboratory data for ectopic orifice are characterized by the detection of leukocytes and bacteria in a general urine test, typical for pyelonephritis. To identify pathogens that support inflammation, a bacteriological examination of urine and a smear from the urethra is carried out.
Treatment of ectopic ureteral orifice
Treatment is surgical, including two fundamentally different approaches - organ-preserving or organ-removing. If the functional characteristics of the kidney are preserved, implantation of the ectopic ureter into the bladder can be undertaken - ureterocystoanastomosis. In the case of duplication of the ureters, good results are obtained by applying ureteropelvic and interureteral anastomoses - ureteropyeloanastomosis and ureteroureteroanastomosis. With these interventions, the accessory ureter, which has an ectopic orifice, is removed, and the part of the kidney that it drained is preserved.
With extravesical ectopia in men, the kidney quickly loses its ability to function normally, so it is often necessary to resort to organ removal interventions. In case of decreased function of one half of the kidney, heminephrectomy with ureterectomy is indicated. If kidney function is completely lost, nephrectomy is performed.
Treatment of pathology
Treatment of ectopia is carried out promptly. It has two different approaches: with and without organ preservation. If kidney function is severely impaired, then compression of the ureter is applied in the area of the ureteropelvic segment. After such a procedure, resumption of ureteral patency often occurs. In this case, this operation is combined with excision along the entire patency of the canal. Removal of the ureter alone increases the risk of developing nephrogenic hypertension and hydronephrosis.
If kidney function is normal, conservation surgery may be performed. Implantation of an ectopic ureter into the bladder. Such actions are called ureterocystoanastomosis. A special mechanism is implanted into the affected area to prevent ureteral reflux. The consequence of such an operation is often stagnation of urine and the development of pyelonephritis. This occurs due to abnormal development of the ureter, congenital expansion of the canal.
If doubling occurs, the most effective method of surgery will be anastomosis. The junction of the part of the ureter that is ectopic is removed, but the part that is leaking is left. With nonvesical ectopia in men, the normal functioning of the kidney is most often disrupted. In most cases, the damaged organ must be removed. Or heminephrectomy is performed - the damaged renal segment is removed. A ureterectomy is also performed - partial or complete removal of the ureter.
After surgery, a course of rehabilitation is required. The patient needs constant medical supervision and care. The rehabilitation course is quite long, it depends on the complications that arise, the characteristics of the body and the general condition of the patient. The patient is required to undergo an X-ray examination every six months or a year in order to verify the anatomical functionality of the genitourinary system.
If there are no complications after surgery, the prognosis is favorable. There is a possibility of developing a disease associated with a urinary tract infection, but in the early stages they are easily curable. Hematuria – bloody spots in the urine – may persist in the early stages. In men, renal circulation may deteriorate after surgery.
For infections, antibiotics are used, instrumental treatment procedures are used: the bladder and ureters are washed with antiseptics and antibacterial drugs. Also, patients are prescribed anti-inflammatory drugs and antispasmodics. The conservative method is only effective in treating stones if they are no more than 6 mm in diameter. Medications help remove stones or dissolve them.
If this does not help, then lithotripsy sessions through the skin are used. This is a modern method of crushing pebbles. Sound waves act specifically on the area with the stone, it crumbles and is excreted along with urine. Sometimes, when prescribed by a doctor, sitz baths and heating pads are performed on the lower abdomen. If blood appears in the urine, such procedures are not carried out.
Prognosis and prevention
With timely initiation of treatment and the absence of complications, the prognosis is usually favorable. In the early postoperative period, urinary tract infections and long-term hematuria may occur. In men after heminephrectomy, in rare cases, disturbances in the blood supply to the kidney are observed, requiring complete removal of the organ. Patients of both sexes are advised to observe a urologist, monitor blood pressure, and undergo periodic tests to exclude proteinuria. Preventive measures include the exclusion of teratogenic effects.
Veterinary medicine is a rather exciting profession. Doctors often have to figure out how and why to treat another four-legged patient. But, as a rule, all cases are quite standard. It happens that a specialist knows about some ailments only from books, without ever encountering them in practice. Here, for example, is ectopia of the ureters in a dog. A rare pathology, but if the dog is unlucky enough to suffer...
First, let's talk a little about normal canine anatomy. So, there are kidneys that filter the blood and produce urine. It goes through the ureters to the bladder, and from there it is discharged into the urethra. The last stage is conscious, that is, the animal can control the act of urination.
So what is the essence of ureteral ectopia? The thing is that with this pathology, the ureters flow directly into the urethra, bypassing the bladder. And what follows from this? It’s simple - urine, barely having time to be synthesized in the kidneys, immediately flows out into the external environment. The animal cannot control this process, and therefore constantly walks... wet, emitting the caustic spirit of ammonia. As a rule, the disease begins to manifest itself clearly from the age of three weeks (in females). In male dogs, the pathology may remain undetected much longer.
But the smell is far from the most unpleasant thing.
The problem is that urine, constantly flowing from the external genitalia, simply corrodes the skin, causing the dog to lose hair en masse from the “back regions.” Such disgrace significantly increases the risk of developing many infectious diseases, including endometritis, cystitis, vaginitis and others. Since this disease also occurs in male dogs, they have no less problems, including orchitis, epididymitis, and balanoposthitis. Females and males suffering from this disease very often become infertile.
Postoperative complications
After the intervention, the patient undergoes a control examination to determine the patency of the ureter and to exclude vesicoureteral reflux (reverse movement of urine from the bladder into the ureter). If the patient was diagnosed with hydronephrosis before surgery, it will persist for several more years.
Late postoperative complications that are difficult to treat - the addition of a urinary tract infection, long-term persistence of hematuria. Sometimes the blood supply to the kidney may be impaired after heminephrectomy. Constant monitoring of blood pressure and proteinuria is necessary. For women after successful surgery, the prognosis is usually favorable.
Diagnosis
How is ectopic ureter in a dog diagnosed? It is quite possible to make a diagnosis based on a combination of clinical signs. We have already said that primary symptoms appear at a very early age, so no particular difficulties are foreseen. But there are still certain tests that are highly advisable to carry out in any case.
It is necessary to do a urine test and culture it on nutrient media. In addition, a blood test is indicated, as this allows you to find out whether the ectopia is complicated by a secondary infection. X-rays and ultrasound examinations of the abdominal cavity are also required. Contrast fluoroscopy is highly desirable, since only this method allows you to clearly see the ureters themselves. Accordingly, along with all their structural pathologies.
Therapy
Alas, the only way out of this situation is surgery.
. Conservative (drug) treatment is ineffective. Only surgery can help. It is quite complex and involves “forced” insertion of the ureters into the bladder. Alas, even with a successful operation, it is not possible to get rid of the side effects of the disease in all cases.
Veterinarians note that restoration of conscious urination is observed in 50-63% of operated dogs. The dependence here is quite simple: the earlier the surgical intervention was performed, the greater the chance of restoring this function. Other animals experience sporadic urinary incontinence throughout the rest of their lives. As a rule, nothing can be done about this.
But this applies only to classical surgical procedures. In the last few years, promising methods of surgical intervention for ureteral ectopia have been developed, in which the surgeon restores muscle structures. If everything goes well, then the chances of completely restoring the normal process of urination increase to 70-86%. As in the previous case, the age of the animal being operated on is of great importance. The earlier (but not earlier than six months of age) the operation was performed, the better for the dog.
Treatment of the disease
First of all, it is necessary to create a new entrance of the ureter into the bladder. Hydronephrosis and severe inflammation in the kidney are indications for organ removal.
If urinary incontinence persists after surgery, repeat X-rays with contrast are performed. Unfortunately, ectopia of the ureter is a developmental anomaly and modern surgical treatment methods help only in no more than 58% of cases. Unfortunately, dogs that exhibit ureteral ectopia have concomitant developmental anomalies of the pelvic organs. For example, they may have a double vagina, as well as a non-functioning sphincter and a short urethra.
For the presence of microbial complications, antibacterial agents are used, which are selected taking into account urine culture. The reason for the persistence of incontinence after surgery may be other congenital anomalies.
We are talking about the failure of the urethral sphincter, underdevelopment of the bladder, developmental disorders of the genital organs, etc. Ectopic ureter
Similar articles
Panosteitis refers to a short-term painful condition characterized by lameness. This disease...
Even if they have thick fur, dogs are still susceptible to extreme...
Leave a request for treatment for your pet right now!