During the process of intrauterine development, deviations occur that provoke improper formation of internal organs. Malformations of the ureters are not uncommon and account for a quarter of all anomalies of the genitourinary system. Pathologies affect the number, shape, location and structure of the ureters. Often, the abnormal development of internal organs does not cause discomfort and does not in any way affect the general condition of the patient. But predominantly abnormal development affects the functioning of the urinary system and provokes improper excretion of urine. In this case, you need to contact a specialist and fix the problem.
Abnormalities in the number of ureters
Aplasia (agenesis)
Aplasia or agenesis of the ureter is an anomaly in which a person is born without an internal organ. The deviation is often combined with aplasia or dysplasia of the kidney. There is unilateral and bilateral deviation. In the first case, aplasia occurs against the background of renal agenesis. In this case, there is an absence of the ureter, which is replaced by a thin fibrous cord or process. Bilateral anomaly is diagnosed extremely rarely and almost always leads to death.
Aplasia can be diagnosed by undergoing excretory urography, which reveals the lack of function in one kidney. Treatment of unilateral aplasia is carried out only when the process ends blindly. In this case, it may fester and develop an inflammatory process. The pathology is manifested by the following symptoms:
- severe constant pain in the lower back;
- complicated urination process;
- heat;
- intoxication of the whole body in a chronic form.
In the laboratory urine result, ureteral aplasia will be manifested by increased levels of white blood cells, bacteria, and protein.
Organ doubling
Duplication of the renal pelvis and ureters is observed relatively often. The anomaly occurs in one newborn out of 150. Doubling is more often diagnosed in women. Often an abnormal number of ureters is combined with a double kidney. In this case, each additional organ has a pelvis and an additional ureter. It is possible that the two ureters join and enter the bladder. But it is more often observed when each mouth goes separately to the bubble itself. As a rule, a deviation does not make itself felt in any way and a person may not find out about the existing anomaly throughout his life. Pathology can be diagnosed accidentally or intentionally if complications arise. In this case, the patient is prescribed cystoscopy, chromocystoscopy and retrograde ureterography.
Tripling of organs
There is a small chance of an abnormality of the ureters, in which the organs triple in size. In medical practice, cases have been recorded when a patient had from 4 to 12 ureters. This defect develops and manifests itself in the same way as a double tubular organ. If there are no complications, no signs of vesicoureteral reflux, then diagnosis and therapy are not prescribed. If an inflammatory process, ureterohydronephrosis or stones occurs, diagnostics is indicated, followed by surgical treatment.
Diagnosis for abnormalities in kidney development
If the doctor suspects renal abnormalities, he must prescribe a series of tests for diagnostic purposes:
- collecting information about life history;
- general blood and urine tests;
- blood pressure measurement;
- examination with palpation;
- examination using ultrasound (ultrasound), including Doppler ultrasound for
- establishing the direction of blood flow through the vessels;
- urography with intravenous administration of a contrast solution;
- computed tomography, which provides extensive information about the structure, structure and position of organs;
- angiography of the renal vessels.
If indicated, it is possible to carry out prenatal diagnosis of the fetus still in the mother’s womb, starting from the 13th week of pregnancy.
Radiation diagnostics of kidney development anomalies
The most complete data on the state of the urinary system can be obtained using modern research methods - radiation or imaging diagnostics. It includes ultrasound, x-ray, MRI and radioisotope techniques.
In the absence of contraindications, these are the most effective ways to check internal organs today. You can learn more about them from presentations that are often found on the Internet.
Ultrasound diagnosis of kidney development abnormalities
Ultrasound is necessary to identify pathologies, including their early stages. The method has virtually no contraindications, but is one of the most productive: ultrasound recognizes stones and inflammations, provides information about the location and size. In some cases, it can successfully replace more expensive computer studies.
Anomalies of structure
Hypoplasia
With hypoplasia of the ureter, as a rule, hypoplasia of the kidney occurs, from which the internal organ originates. This malformation of the kidneys and ureters is characterized by underdevelopment of internal organs. In pathology, there is insufficient development of one layer of the tubular organ of the urinary system, usually the muscular layer. During diagnosis, you may find that there is a narrowing of the ureter, but urine is able to pass. Less common is closure of the ureter with subsequent accumulation of urine. Given the complexity of the deviation and the condition of the diseased kidney, treatment is possible with nephrectomy, in which the kidney and ureter are removed.
Tubular organ stricture
By stricture we mean a narrowing of the urinary system organ, which forms in the ureteropelvic or vesicoureteral segment. There are the following types of strictures:
- one-sided or two-sided;
- single or multiple.
This abnormal phenomenon in an internal organ is mainly associated with congenital abnormalities, but often has an acquired nature. Acquired stricture is associated with trauma, instrumental damage, or prolonged inflammation. The symptoms of congenital and acquired deviations are identical. A person has the following signs of narrowing:
- stagnation of urine;
- impaired urination;
- hydronephrosis develops;
- infection occurs.
Diagnosis of the defect is possible only with the use of excretory urography, which is carried out using a contrast agent. A stricture can only be eliminated surgically. The type of surgery will be prescribed based on the general condition of the urinary tract and the location of the stricture. If the kidney parenchyma is significantly damaged and its functions are lost, then the internal organ and ureter are removed (nephroureterectomy).
Valve formation
The transverse folds, which are formed from the mucous membrane and contain muscle fibers, are called ureteral valves. For this reason, urine is unable to fully or completely penetrate the bladder. This anomaly is exclusively congenital. In a newborn, the length of the organ is the same as in an adult. For this reason, until the age of 4 years, a child’s ureter looks like a spiral, and there are valves at the bottom of the organ. Due to the wide lumen of the ureter in children, urine can be easily excreted. With age, the ureteral valves disappear and the anomaly goes away.
If the child’s pathology has not been reduced, then a gradual disruption of urine excretion occurs. First, the amount of urine decreases, and then the process of urination stops altogether. It is necessary to conduct a comprehensive diagnosis to confirm the diagnosis. After which treatment is prescribed, which is aimed at restoring the process of urination. As a rule, surgical therapy is indicated, in which the affected organ is removed or partially dissected.
Diverticulum
Diverticulum has a congenital and acquired nature and is characterized by a formation that resembles a ball connecting to the lumen of a tubular organ. As a rule, the anomaly affects the lower third of the ureter. A diverticulum may occur on both sides, but is predominantly located on the left side. When the diverticulum becomes large, it begins to put pressure on the ureter, which causes expansion of the organ, pelvis and parenchyma of the kidney. The patient undergoes removal of the diverticulum, and if necessary, a nephroureterectomy is performed.
Ureterocele
With ureterocele, a cystic formation is diagnosed that protrudes into the bladder. Typically, the anomaly occurs on the right side, but bilateral ureteroceles are not uncommon. The formation ranges from 1-2 mm to several centimeters. In women, a large ureterocele can protrude outward through the urethra. There are the following types of ureterocele:
- simple;
- protruding through the urethra;
- opening into the urethra or bladder diverticulum due to ectopia;
- blindly ending.
Neuromuscular dysplasia
This malformation is associated with a congenital abnormality in which the opening of the ureter and its intravesical part narrows, and neuromuscular dysplasia of the lower third of the organ occurs. Thus, the deviation causes megaureter - expansion of the tubular organ. An anomaly occurs due to the underdeveloped neuromuscular system of the organ. Often the deviation manifests itself when there are functional or organic obstacles in the area of the prostatic region or in the area of the intravesical part of the organ. The following stages of the anomaly are distinguished:
- achalasia, in which the lower part of the cystoid expands;
- megaureter is characterized by ureteral expansion along its entire length;
- hydroureteronephrosis is an irreversible deviation of the urodynamic and hydronephrotic function of the kidney.
Chapter 38. Diseases of the ureters
DISEASES OF THE URETER (UROLOGY)
The ureter is a hollow organ that drains urine from the kidneys to the bladder. The function of the ureter is finely regulated. Its violation, regardless of the cause, leads to kidney damage - most often hydronephrosis (Chapter 12) and pyelonephritis. Ureteral pathology can be congenital (developmental defects) or acquired.
DEVELOPMENTAL MALFORMATIONS OF THE URETER
Malformations of the ureters - from aplasia to duplication or tripling - are quite common. They may cause urinary tract obstruction requiring immediate treatment or may not cause any symptoms. To avoid confusion, instead of the old classifications of ureteral malformations, a new one was adopted, which is considered standard.
Aplasia of the ureter
With this malformation, the ureter is completely absent or is a blind outgrowth going to the side of the abdomen. The reason is a violation of the embryogenesis of the ureter, when the ureteral outgrowth from the Wolffian duct does not form at all (the kidney is also absent) or stops its development before growing into the metanephrogenic tissue (this leads to multicystic kidney). Bilateral multicystic kidney disease in combination with other developmental defects - Potter syndrome - is incompatible with life. Unilateral multicystic kidney disease usually does not manifest itself in any way. Less common are hypertension, infection, or kidney cancer. With unilateral multicystic kidney disease, most experts recommend observation, since the kidney atrophies over time. Because of the small increase in the risk of kidney cancer, some authors consider nephrectomy to be advisable. Due to the high incidence of vesicoureteral reflux on the opposite side, voiding cis-urethrography is indicated.
Duplication of the ureter
Complete or incomplete duplication of the ureter is the most common malformation of the urinary tract. According to autopsies, it occurs in 0.9% of cases, in girls - more often than in boys, and is often bilateral. The type of inheritance is autosomal dominant with incomplete penetrance.
Incomplete (Y-shaped) duplication of the ureter is the result of splitting of the ureteric outgrowth into
melting into metanephrogenic tissue. Clinically, this malformation, as a rule, does not manifest itself, but peristalsis at the site of cleavage may be impaired (Fig. 38.1). In such cases, due to reflux of urine from one half of the ureter to the other, dilation or obstruction of one or the other half is possible. Surgical treatment is ureteropyelostomy, which is effective in most cases.
Complete duplication of the ureter is the result of the formation of two ureteric processes, from which two ureters and two separate renal pelvis develop. During duplication, the main ureter is formed first in the caudal part of the Wolffian duct and drains the lower half of the duplicated kidney. The accessory ureter drains the upper half of the kidney, but enters the bladder caudal to the main one. Thus, according to the Weigert-Meyer law, duplicate ureters always intersect. If the ureter, which drains the upper half of the kidney, becomes too long during growth, ectopia and obstruction occur. The ureter, which drains the lower half of the kidney, usually enters the bladder more laterally than normal and has a shortened intramural section, which causes vesicoureteral reflux (Fig. 38.2). These patterns are also true for a more rare malformation - tripling of the ureter.
Duplication of the ureter may not be clinically evident or may be accompanied by recurrent infections.
Drawing 38.1.
Incomplete (Y-shaped) duplication of the ureter and hydronephrosis of the lower half of the left kidney. There is a reflux of urine from one half of the doubled ureter to the other, as a result of which one of them expands.
Figure 38.2. Bilateral complete duplication of the ureters. Reflux into the ureter draining the lower half of the right kidney, and nephrosclerosis as a result of chronic pyelonephritis. Ectopic orifice of the ureter draining the upper half of the left kidney.
tions of the urinary tract. In girls, the ureter draining the upper half of the double kidney may open distal to the urethral sphincter and even outside the urinary tract. Characterized by urinary incontinence (constant dribbling) during normal urination. In male fetuses of aviaries, the duct becomes the vas deferens and seminal vesicles, so the ectopic orifice of the ureter is always located proximal to the urethral sphincter and there is no urinary incontinence. In recent years, with the help of ultrasound, duplication of the ureters is detected in the prenatal period.
The most informative methods for diagnosing ureteral duplication are excretory urography and voiding cystourethrography. Duplication of the ureter is almost always detected on excretory urograms. The exception is cases when one ureter is not contrasted due to a sharp decrease in the function of the half of the double kidney drained by it. In this case, duplication can be suspected by indirect signs - displacement of the contrasting renal calyces or ureter and too few renal calyces for a kidney of a given size. Excretory urography also reveals nephrosclerosis, which develops as a result of chronic pyelonephritis. Migration cystourethrography helps detect vesicoureteral reflux and ureterocele. In
In many clinics, instead of excretory urography, ultrasound is now performed, which clearly reveals atrophy of the upper half of the double kidney and hydroureter, measures the thickness of the renal parenchyma and identifies organic changes in the bladder. Renal scintigraphy with 99t Tc-DMS allows a detailed assessment of renal function (Fig. 38.3).
The treatment tactics for vesicoureteral reflux, if present, do not depend on the presence of ureteral duplication. In mild cases, conservative treatment is indicated; in cases of severe reflux, surgical treatment is indicated. Surgical treatment of ureteral duplication is indicated for obstruction of the ureter draining the upper half of the duplicated kidney and ureteral ectopia. As with vesicoureteral reflux, a variety of operations are performed. If the function of half of the doubled kidney is sharply reduced, heminephrectomy is indicated. Otherwise, organ-preserving operations are performed - pyeloureterostomy, ureteroureterostomy or ureterocystoneostomy.
Ureterocele
A ureterocele is a sac-like protrusion of the intramural part of the ureter (Fig. 38.4). It can be intravesical and ectopic (in the latter case, part of it is located in the neck of the bladder or in the urethra). Intravesical ureterocele usually occurs without duplication of the ureter, ectopic - with duplication of the ureter, mainly in the ureter draining the upper half of the duplicated kidney. Ectopic ureterocele occurs 4 times more often than intravesical ureterocele. In girls, ureterocele is observed 7 times more often than in boys; in 10% of cases it is bilateral. A small ureterocele may be an incidental finding in adults.
The cause of ureterocele is considered to be slow or incomplete resorption of tissue inside the ureteric process, which is why, even in embryogenesis, obstruction and expansion of the ureteric process occurs proximal to the confluence with the urogenital sinus. A sac-like protrusion forms between the superficial and deep layers of smooth muscle of the triangle of the bladder. A large ureterocele can displace the orifice of the second ureter, dissect the detrusor, and even cause bladder neck obstruction. Often, ureterocele leads to pronounced hydroureter and hydronephrosis, and can be combined with atrophy of the upper half of the double kidney (the renal parenchyma may contain remnants of metanephrogenic tissue that are prone to malignancy).
Ureterocele manifests itself in different ways. Typically, the diagnosis is made by testing for a urinary tract infection. Patients may seek medical attention for symptoms of bladder outlet obstruction or urinary incontinence. In rare cases, girls or women experience ureterocele prolapse
Figure 38.3.
Duplication of the ureter and ureterocele. A. An excretory urogram shows a doubled right kidney (the upper half is shown with short arrows, the lower half with long arrows). On the left, only the lower half of the left kidney is visualized (shown by the white arrow). A filling defect was detected in the left bladder. B. Cystography also revealed a defect in bladder filling. There is no reflux. B. Renal scintigraphy with 99t Tc-DMS shows the functioning parenchyma of the upper half of the left kidney. D. After surgical correction of ureterocele and ureterocystoneostomy on the left, control excretory urography shows contrasting of the upper half of the left kidney.
Figure 38.4. Ureterocele. A. Bilateral ureterocele without duplication of the ureter. B. Ureterocele in combination with duplication of the ureter and decreased function of the upper half of the doubled left kidney.
urethra. Stagnation of urine provokes the formation of urinary stones, which are most often found in the distal ureter. Diagnosis is usually made by excretory urography (Figs. 38.3 and 38.5), which reveals a saccular outpouching or filling defect in the bladder. This study also makes it possible to judge the degree of hydronephrosis and identify kidney duplication. As already mentioned, many clinics now perform ultrasound instead of excretory urography. Victory cystourethrography is mandatory, in which it is possible to detect reflux of urine from the bladder into the ureter, which drains the lower half of the kidney, and eversion of the ureterocele during urination, which makes the ureterocele look like a diverticulum. Scintigraphy is used to assess renal function.
Treatment is selected individually. The only operation that was previously performed in severe cases of children with pyonephrosis was transurethral dissection of the ureterocele. However, recently it is believed that more radical interventions are possible in many cases, especially with intravesical ureterocele. The type of operation depends on the location of the ureteral orifice and ureterocele, as well as the degree of hydronephrosis and renal dysfunction. The scope of intervention ranges from heminefroureterectomy to ureterocele excision, reconstructive bladder surgery and ureterocystoneostomy. Often surgical treatment is carried out in two stages.
Ectopic ureter
Although ectopic ureter is most often combined with ureterocele and duplication of the ureter (see above), this malformation is possible without duplication of the ureter. The reason is a delay or disruption of the separation of the ureteric process from the Wolffian duct in embryogenesis. The cause of ectopia can also be the abnormal position of the ureteric outgrowth. This explains the frequent combination of renal malformations with ectopia of the ureteral orifice without its doubling.
The clinical picture depends on the gender of the patient and the location of the ureteral orifice. Boys usually do not have urinary incontinence. However, many people experience acute epididymitis when the ureter opens into the vas deferens or seminal vesicles. In girls, the ectopic ureteral orifice may be located in the urethra, in the vagina, or on the perineum. Infection is possible, especially if urine refluxes through the ectopic orifice. However, the pathognomonic symptom of ureteral ectopia in girls is urinary incontinence, which constantly leaks drop by drop, with normal urination. The diagnosis is more difficult to make if there is urgency and urinary incontinence. Often, ectopia of the ureter is combined with malformations of the genital organs.
Ultrasound and voiding cis-urethrography are used in diagnosis. In cases where ectopia of the ureter is combined with dystopia and reduction of the kidney,
It can be difficult to detect the latter with ultrasound. In boys, the ectopic ureteral orifice is easily identified by cystoscopy or retrograde catheterization of the ejaculatory duct (Fig. 38.6). Indirect signs of ectopic ureter are underdevelopment of one half of the bladder triangle and a cystic space-occupying formation in the lateral abdomen. In girls, the ectopic ureteral orifice can sometimes be seen next to the external opening of the urethra. In such cases, the diagnosis is confirmed by retrograde pyelography after the introduction of a radiocontrast agent into the ectopic orifice (Fig. 38.7). Renal scintigraphy allows you to evaluate the structure of the urinary tract and kidney function.
Treatment tactics depend on the clinical picture and renal function. If surgical treatment is indicated, ureterocystoneostomy or nephro-ureterectomy is performed. When the ureter is doubled, in some cases it is possible to perform a ureterocystoneostomy without touching the second ureter.
Abnormalities of the position of the ureters
The retrocaval (circumcaval or postcaval) ureter is a rare malformation in which
The normally formed ureter passes behind the inferior vena cava. The reason is a violation of embryogenesis of abdominal vessels. While the right posterior cardinal vein transforms into the secondary inferior vena cava, the persistent primary inferior vena cava pushes back the ureter and “forces” it to go around the secondary inferior vena cava posteriorly. There are two anatomical variants of the retrocaval ureter. In the first, the upper third of the ureter and the renal pelvis pass behind the inferior vena cava almost horizontally: there is no obstruction and no treatment is required. In the second option, the ureter runs normally to approximately the level of the L3 vertebra, where it bends backward in an inverted J shape and bends around the inferior vena cava, usually causing an obstruction.
The diagnosis is easiest to make with excretory urography. But, since the examination usually begins with ultrasound, a retrocaval ureter should be suspected when dilation of only its proximal parts is detected. Retrograde pyelography also makes it possible to diagnose this malformation. Cavography can be performed at the same time (Fig. 38.8). Nowadays, one modern method, accurate and non-invasive, is enough for diagnosis - MRI.
Figure 38.5. Ureterocele. A. Excretory urography shows moderate dilatation of the ureters (shown by long arrows), deformation of the distal ureters in the form of a cobra head, bilateral ureterocele (shown by short arrows) with minimal obstruction. The bladder is compressed by the uterus (the boundaries of the bladder are marked by white arrows). No treatment required. B. Excretory urography in an 8-year-old patient revealed a space-occupying formation in the bladder (shown by short arrows). The calyces of the upper half of the left kidney are not contrasted (shown by long arrows). This indicates duplication of the ureter and renal pelvis, and also that due to severe hydronephrosis, the upper half of the doubled left kidney does not function. The dilated ureter draining it passes into the ureterocele and, just below the kidney, displaces the second, contrasted, ureter laterally.
Figure 38.6. Ectopic ureter. A. The contours of the right kidney are not visible on the excretory urogram; the upper urinary tract on the right is not contrasted. B. With retrograde injection of a radiocontrast agent into the ejaculatory duct, the seminal vesicle and the ectopic orifice of the ureter are visualized (shown by arrows). B. A similar picture with geni-
tography.
If surgical treatment is indicated, the ureter is crossed (preferably in the widened part), its distal section is isolated from under the inferior vena cava and ureteroureterostomy is performed. To facilitate the postoperative period, the operation can be performed laparoscopically. If the retrocaval portion of the ureter is sclerotic or narrowed, its resection is performed.
There are other rare anomalies of the position of the ureter. For example, the left retrocaval
ureter in a patient with inverted internal organs and several cases of the ureter positioned behind the iliac vein. Treatment is the same as for retrocaval ureter.
Obstruction of the ureteropelvic segment
This malformation, together with obstruction of the vesicoureteral segment, is the most common cause of obstruction.
Drawing 38.7.
Ectopic ureter (6-year-old patient with congenital urinary incontinence). A. Cystoscopy revealed two ureteral orifices on the right and one on the left. All ureters were catheterized and retrograde pyelography was performed. B. The ureter is catheterized, the mouth of which is located next to the external opening of the urethra. Retrograde pyelography reveals a second, sharply dilated pelvis of the left kidney. After heminefroureterectomy, urinary incontinence ceased.
Figure 38.8.
Retrocaval ureter. A. A retrograde pyelogram shows displacement of the proximal ureter medially to the spine. Congenital deformation of the spine is also visible. B. On the cavogram (right oblique projection) the retrocaval ureter is visualized. M - ureter, MK - urinary catheter, IVC - inferior vena cava, CPV - common iliac vein.
structures of the ureters in children (Fig. 38.9). In turn, obstruction of the ureteropelvic segment is the most common malformation of the ureters. In boys it occurs more often than in girls (in a ratio of 5:2); with unilateral lesions it is more often localized on the left than on the right (also in a ratio of 5:2). Bilateral obstruction of the ureteropelvic segment is observed in 10-15% of cases, mainly in infants. Although familial cases of this pathology have been described, the mode of inheritance has not been established. The cause of ureteropelvic segment obstruction often remains unknown. Ureteral polyps and valves have been described, but are rare. The formation of an angle at the junction of the dilated renal pelvis into the ureter is characteristic. Although this anatomical feature may lead to obstruction, whether it is the underlying cause or a consequence of another malformation causing the obstruction is usually not clear. Stenosis of the ureteropelvic segment is a rare phenomenon; thinning of the wall and underdevelopment of the proximal ureter are much more common. Perhaps it is the structural features of the proximal ureter that underlie the disturbance of peristalsis of the ureteropelvic segment and, as a result, obstruction. During the operation, no
Two more features are rarely found - the high origin of the ureter from the renal pelvis and the intersection of the proximal ureter with the accessory artery supplying the lower pole of the kidney. The cause or consequence of the expansion of the renal pelvis is not clear, but, according to some authors, this malformation occurs due to abnormal rotation of the renal pelvis. Obstruction of the ureteropelvic segment caused by a disorder in the structure of the urinary tract can be distinguished from external compression by careful inspection during surgery.
The clinical picture depends on the age at which the developmental defect was detected. Currently, the diagnosis in most cases is made by ultrasound in the prenatal period. Sometimes a mass formation is found in the abdomen of an infant. In older children, abdominal pain and vomiting are most common, and hematuria and urinary tract infections are possible. In some cases, the diagnosis is made when complications occur - obstruction of the ureter by a stone (Fig. 38.10), injury to an enlarged kidney, or, rarely, arterial hypertension. Rarely, the disease is asymptomatic.
Excretory urography or ultrasound is used in diagnosis. In doubtful cases, scinti-
Drawing 38.9.
Congenital ureteral obstruction. A. Obstruction of the ureteropelvic segment and hydronephrosis on the right. B. Obstruction of the vesicoureteral segment on the left, hydroureter and hydronephrosis.
Figure 38.10.
Obstruction of the ureteropelvic segment on the right by a stone. A. An x-ray of the abdomen shows visible shadows in the projection of the right kidney. B. On the excretory urogram in the nephrographic phase, dilated drinking cups and multiple stones along the walls of the renal pelvis are visible. B. A delayed excretory urogram shows a picture typical of obstruction of the ureteropelvic segment.
kidney graph after administration of a diuretic or the Wee-Tucker test. Many surgeons consider voiding cystourethrography mandatory, since excretory urograms show vesicoureteral reflux and obstruction of the ureteropelvic segment.
| look the same. It is especially difficult to distinguish between these diseases when the ureter is highly contrasted.
: van or extended (or both) below level
obstruction, but necessary because one of the reasons
obstruction of the ureteropelvic segment -
pronounced vesicoureteral reflux.
Obstruction of the ureteropelvic segment with
: clinical manifestations - indication for surgery.
! Since now this malformation in most cases is diagnosed in the prenatal period and
I Most patients do not have clinical manifestations; it is important to be able to assess the severity and clinical significance of obstruction. On the one hand, surgical treatment at an early age can prevent complications, including urinary tract infections and urolithiasis, on the other hand, hydronephrosis may not manifest itself throughout life. Although the issue of indications for surgical treatment in general has not been resolved, chronic renal failure is considered absolute,
severe hydronephrosis, urinary tract infections and urolithiasis
; new disease. In other cases, they are limited to observation. Due to subsequent complications, approximately 25% of patients usually have to undergo surgery.
Due to the variety of anatomical variants, there is no universal operation for ureteropelvic segment obstruction. The goal of surgical treatment is always the same - to create a funnel-shaped ureteropelvic segment with sufficient diameter. In some cases, when the patency of the ureter is impaired over a short distance, for example due to compression by a vessel, the ureteropelvis
] the nickname segment is not crossed. In other cases, including when the cause of obstruction is a loop-like course of the ureter around the vessels going to the lower pole of the kidney, resection pyeloplasty is preferred. When the pelvis is located extrarenally, resection pyeloplasty is combined with Foley pyeloplasty (Y- or V-shaped flaps) so that the newly created ureteropelvic segment resembles a funnel as much as possible. Pyeloplasty according to Culp or Scardino (with cutting out a spiral or vertical flap, respectively) is indicated in cases where the renal pelvis is significantly dilated, but passes into the ureter at a normal level. These operations are also good because they less disrupt the blood supply to the ureter - this is important if surgery on the distal ureter (for example, ureterocystoneostomy) is planned in the future. Pyeloplasty according to Foley, Culp or Scardino is also indicated in cases where obstruction of the ureteropelvic segment occurs with a horseshoe kidney or its pelvic dystopia, since with resection
pyeloplasty in such conditions is impossible to anastomose the ureter with the most distal part of the renal pelvis. Whether it is necessary to install a ureteral stent or apply a nephrostomy during pyeloplasty is an open question. Good results were obtained both with and without these additional measures.
The prognosis is usually favorable, since the pathology is often unilateral, and with bilateral pathology, the obstruction on one side is almost always less pronounced than on the other. Imaging after surgery often shows no improvement, but several large studies suggest that repeat surgery is required in only 2% to 4% of cases. Significant improvement is observed with the extrarenal location of the pelvis, when the renal calyces are slightly deformed. In most cases, the expansion of the renal calyces persists, despite the normal outflow of urine.
Relatively recently, antegrade and retrograde pyelotomy began to be performed for obstruction of the ureteropelvic segment. These operations resemble Davis intubation ureterotomy. Retrograde pyelotomy can be performed using a catheter electrocautery (Akyusize). In adults, this is the best treatment method, effective in 80-85% of cases with a low risk of complications. In children, retrograde pyelotomy is also successful in 85% of cases, but open surgery is effective in 98% of patients, and the risk of complications after open surgery is not much higher than after endoscopic intervention. Laparoscopic pyeloplasty is also promising.
Obstruction of the vesicoureteral segment
Obstruction of the vesicoureteral segment occurs 4 times more often in boys than in girls. It is often bilateral, but on the right and left, as a rule, it is expressed to varying degrees. On the left, this malformation is observed somewhat more often. It is curious that with unilateral obstruction of the vesicoureteral segment in 10-15%
cases, agenesis or other malformations of the kidney on the opposite side are noted. The mechanism of embryogenesis disorders is not clear. It is only known that in most cases there is no stenosis of the vesicoureteral segment. During surgery, the catheter or probe can usually be advanced retrogradely above the level of obstruction. Monitoring intraoperative or fluoroscopic ureteral function may reveal a lack of distal peristalsis, resulting in functional obstruction. Histological examination reveals an excess of circular muscle and collagen fibers in the distal ureter, which may be the cause of the observed abnormalities. The changes are similar to those revealed
caused by obstruction of the ureteropelvic segment.
Currently, many cases of the disease are diagnosed using ultrasound and even in the prenatal period. Vesicoureteral segment obstruction usually presents with urinary tract infections, fever, and abdominal pain. Hematuria is often observed, which occurs in the absence of infection. The cause of hematuria is considered to be rupture of the vessels in the ureteral mucosa due to its overstretching. Another cause of hematuria is the formation of stones due to stagnation of urine. A pathognomonic sign of obstruction of the vesicoureteral segment during excretory urography is a sharply dilated distal ureter in the shape of a spindle or bulb and a less dilated proximal portion, a relatively normal renal pelvis and flattened renal calyces (Fig. 38.11). In some cases, to clarify the diagnosis, they resort to antecedents.
Drawing 38.11.
Obstruction of the vesicoureteral segment. Control excretory urogram in a 9-month-old patient with hydronephrosis detected in the prenatal period. A significantly dilated distal and less dilated proximal ureter and flattened renal calyces are visible.
grade or retrograde pyelography, renal scintigraphy after administration of a diuretic or Whitaker test. Previously, it was believed that in most cases of obstruction of the vesicoureteral segment, surgical treatment was indicated - resection of the distal ureter and ureterocystoneostomy. Due to the pronounced expansion, it is often necessary to first give the ureter a conical shape. Usually, part of the ureteral wall is excised on the side where the vessels do not enter it. With moderate dilatation of the ureter, intussusception of the dilated section can be performed. Since most of the smooth muscle of the ureter is normal, the prognosis is favorable. Meanwhile, in recent years it has become obvious that in at least 50% of patients, obstruction of the vesicoureteral segment spontaneously disappears over time. In this regard, in the absence of clinical manifestations, observation is quite justified. Due to the high risk of infection in newborns, antimicrobial prophylaxis is recommended and continued throughout the first 1–2 years of the child’s life.
Dilatation of the upper urinary tract without obstruction
Dilation of the upper urinary tract is not always a sign of obstruction. If dilatation is detected, voiding cysto-urethrography must be performed, because it excludes not only vesicoureteral reflux, but also malformations of the lower urinary tract. Diagnostic difficulties arise with residual dilation of the upper urinary tract after removal of obstruction, dilation due to bacterial infection (probably due to the direct effect of endotoxin on the smooth muscles of the ureter), hydronephrosis in newborns, as well as with prolonged polyuria in patients with diabetes insipidus. These cases require special research. Scintigraphy of the kidneys after administration of a diuretic helps to exclude obstruction (Fig. 38.12). Recently, puncture of the pyelocaliceal system has been increasingly performed. Against the background of its expansion, the risk of complications is minimal, but after puncture, antegrade pyelography and the Whitaker test can be performed. The latter is very useful for differential diagnosis (Chapter 8). Unfortunately, no research method can be considered absolutely reliable; sometimes different | methods give conflicting results, so the diagnosis is mainly determined by the clinical picture. I
content .. 60 61 62 ..
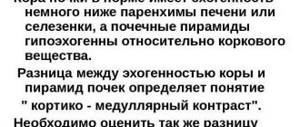
Shape anomalies
The ureter may be corkscrew-shaped or take on the appearance of a ring. The organ acquires a corkscrew or spiral shape as a result of kidney anomalies during intrauterine development. When they rise from the small pelvis, they unfold, and the ureters rotate. If the ureters remain in the same position and do not rotate, then they become twisted. Sometimes twisting provokes the formation of ring-shaped ureters.
The irregular shape of the tubular organ leads to improper excretion of urine from the kidney. In this case, the development of hydronephrosis, chronic pyelonephritis and the formation of kidney stones is inevitable. Depending on the severity of the anomaly, conservative or surgical treatment is prescribed. Considering the location of the problem, ureteroureteroanastomosis or ureterocystoanastomosis is prescribed.
Anomalies observed in the relationship of both kidneys
Horseshoe kidney. The lower poles of both kidneys are connected by an isthmus of renal parenchyma passing over the aorta. This area of the renal parenchyma is richly supplied with blood vessels, which fix it. The ureters of such a horseshoe-shaped kidney are located on its anterior surface, reach the isthmus and descend down. The same phenomena are established in other developmental anomalies similar to the horseshoe kidney (L- and S-shaped kidney, shapeless kidney).
If you have a horseshoe kidney, there may be continuous pain in the epigastric region, which is sometimes considered a sign of a gastric or duodenal ulcer. Complications such as hydronephrosis and kidney stones are common and require appropriate treatment. When pain occurs in the epigastric region, an operation with dissection of the isthmus and separation of both kidneys is indicated.
Position anomalies
Often a tubular organ is formed in the wrong place where it should be. The following position anomalies are identified:
- retrocaval organ;
- retroiliac;
- ectopic foramen.
With the rectocaval organ, an incorrect location occurs: the ureter, usually on the right side, is located behind the inferior vena cava. In this case, a person’s urine excretion is disrupted and hydronephrotic transformation occurs. A rare pathology is considered to be a retroiliac location, which is characterized by the presence of a ureter behind the iliac artery.
Ectopia is caused by the incorrect location of the mouths of the tubular organ. There are unilateral and bilateral anomalies. The mouth of the organ can be located and open into the neck of the bladder, the urethra. In women, it happens that the mouth is directed towards the vagina or uterus. In any case, prompt elimination of the problem and transfer of the mouth to the bladder is indicated.
Malformations of the kidneys and urinary tract in children
During embryogenesis, filter organs go through three main phases:
- preference;
- primary;
- constant.
The first is formed in the 2nd week of his life, but very soon it is greatly reduced in size. Instead, a primary one is formed, in the form of an elongated ellipse, which subsequently bifurcates. One takes part in the formation of the reproductive system, the other is responsible for the urinary system. Such a close relationship is the cause of joint pathologies of the genitourinary tract. Congenital kidney anomalies in children rarely go unnoticed by reproductive centers.
Congenital phimosis.
The opening in the foreskin may be narrowed and cause difficulty urinating. There are two forms. In one of them, the opening is narrow and the foreskin is fused with the head of the penis and when urinating, the stream is very thin or flows out in drops. In the second type, the opening is narrow, but the foreskin is not fused to the head of the penis. In such children, urine is released in drops or a thin stream, and the foreskin expands like a balloon. Treatment for mild forms of phimosis is conservative, in which the foreskin is gradually separated from the head of the penis every day in order to widen the opening of the flesh. For more severe forms, surgical treatment is necessary.
Congenital sclerosis of the bladder neck (Marion's disease).
The muscular layer of the bladder neck under the mucous membrane is hypertrophied and serous changes. This causes dyskinesia and difficulty in urinary evacuation. The disease was first established by Marion (1938) and is known by this name.
1. Among newborns, the disease is almost always boys, who have developmental delays and lack of appetite: the height and weight of children do not progress, sometimes intestinal disorders are observed; The temperature in children is low-grade. Vomiting occurs frequently. The stream of urine during miction is sluggish, and sometimes in some children urine flows out in drops.
In advanced cases of the disease, during clinical examination it is easy to feel the position of the bladder above the pubis. The urine becomes infected, interstitial nephritis develops, and serum urea and creatinine levels increase gradually. In such children, water and electrolyte disturbances occur very quickly, accompanied by acidosis and hyperkalemia. Secondary reflux appears, aggravating the condition of the sick child.
An accurate diagnosis is made using excretory urography, voiding cystourethrography and cystoscopy. Treatment is surgical.
2. In young children (from 2 to 5 years old) with Marion's disease, some children have a good general condition, but there is a disturbance in mictriculation. They urinate frequently and the stream of urine is sluggish. Children are almost always wet, so you can feel the bladder before miction. Urea levels are normal, kidneys are functioning normally, and urine is not infected. In other children, the disease is characterized by general intoxication, the causes of which are not clear. There is paradoxical ischuria and urinary infection. caused by Escherichia coli, etc. Progressive kidney failure gradually develops due to the onset of interstitial nephritis. The upper urinary tract is dilated and reflux is observed on the cystogram. Treatment is surgical, after which antibacterial treatment should be carried out for a long time.
3. In older children (5-15 years), mainly schoolchildren, there are complaints of polakiuria during the day and bedwetting. Urinary disorders have a depressive effect on children, who cannot control their urine output even during classes.
The diagnosis is made using excretory urography, voiding cystourethrography and cystoscopy. Treatment is surgical.
Valves on the posterior surface of the urethra. These are valves located at the back of the urethra that prevent normal urination. From the first days of life, they cause chronic urinary retention and kidney failure. Found only in boys.
The clinical picture in infants is characterized by frequent vomiting, diarrhea, dehydration, and developmental delays. A common symptom is constantly wet diapers of infants. The deterioration of the general condition occurs quickly, the level of urea in the blood rises, and the child may die within a few months from uremia.
In older children, the disease occurs with impaired urination, the urine stream is sluggish, and sometimes urinary retention is observed.
The diagnosis is made using excretory urography, in which it is possible to establish the dilation of all organs of the urinary system. Victory cystourethrography and cystourethroscopy confirm this diagnosis due to the characteristic picture that is observed with them. Treatment is surgical. Preferably, transurethral resection of the valves of the posterior surface of the urethra is performed.
Pseudopolyps on the posterior surface of the urethra. This is a myxoma-type pseudotumor located on a pedicle, with the base of the tumor located in the posterior part of the urethra. It causes dysuria and urinary retention. The diagnosis is made using excretory urography, voiding cystourethrography and cystoscopy. Treatment is surgical with a good outcome.
Anomalies of the vesicoureteral segment
The vesicoureteral segment is an important junction of the urinary system. This is the boundary between the upper and lower urinary tracts. Obstructive malformative uropathy in this segment can be multiple and their cause is morphological or functional. These anomalies are divided into two large groups: megaloureter and vesicoureteral reflux (vesicoureterorenal reflux).
Megaloureter. This is an anatomical dilatation of the ureter caused by obstructions at the level of this segment. The reasons that lead to the development of megaloureter are different and this gives a certain reflection on its clinical manifestations.
The leading symptoms for various forms of megaloureter in infants are: a gradual increase in weight and height, persistent pyuria, sometimes accompanied by an increase in temperature, albuminuria, dyspepsia, hematuria: later the picture of pyelonephritis and renal failure develops. In older children, the symptoms described above, which may be expressed to a milder degree, are gradually joined by polyuria. polydipsia and other manifestations of renal failure.
It is necessary to diagnose the disease as early as possible, before irreversible kidney damage has yet developed. To do this, excretory urography, cystography, cystoscopy, etc. are performed.
Treatment is surgical, followed by treatment for pyelonephritis.
Hypospadias.
According to various statistics, out of 500-1000 newborn boys, one is born with hypospadias. There are various forms: hypospadias of the glans penis, penis-scrotal, scrotal, perineal. With the exception of hypospadias of the glans penis, in almost all other forms there is a curvature of the penis, which is especially clearly visible during an erection. With scrotal hypospadias and perineal hypospadias, the penis is bent, short, and resembles a clitoris. In such cases, the doctor should direct his attention to establishing true or pseudohermaphroditism. The operation is performed between the ages of 3 and 6 years so that the child has a normal penis by the time he enters school.