According to statistics, in the modern world the development of anomalies of the genitourinary system
occurs in every tenth person on planet Earth. Anomalies lead to serious disorders and problems of a physiological and psychological nature. Abnormalities of the genitourinary system can only be diagnosed using specialized medical equipment, such as ultrasound or x-ray.
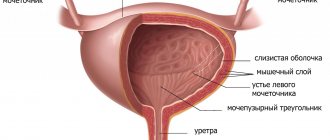
Malformations of the urinary organs (genitourinary system)
– are genetic mutations expressed by the hyperdevelopment of a particular organ or, conversely, its underdevelopment. Anomalies affect the kidneys, bladder, ureters, urethra, as well as the male and female genital area.
Pathologies of the organs of the genitourinary system are divided into two types: anomalies in the structure of the organ and anomalies in the location of the organ in the abdominal cavity. Developmental disorders of the ureters include:
- Doubling
- Congenital narrowing
- Aplasia
- Ectopia
- Retrocaval arrangement
- Pathology of ureteral valves
- Doubling
- Diverticulum
- Aplasia
- exstrophy
With pathology of the bladder there is:
It is worth noting that the most dangerous is exstrophy - a pathology of both the bladder and the abdominal cavity, pelvic bones, as well as the urinary canal. This disease requires mandatory treatment, otherwise it can be fatal.
Pathologies of the urethra in men are malformations of the urethra (urinary system), or in other words, congenital pathology of the structure of the urethra and disruption of its functions. Pathologies include: hypospadias, epispadias and duplication.
Hypospadias
It occurs only in men and is an abnormal location of the external opening of the urethra, usually located lower than it should be.
Epispadias
, on the contrary, is an anomaly in which the opening of the urethra is located above normal in the upper cavity of the genital organ.
Urachal pathologies
Certain anomalies of the urachus are observed - a special tube that connects the bladder of a baby being carried by a woman with the amniotic fluid:
- urinary diverticulum - the urachus does not heal completely, while a bulging wall forms in the area of the urachus;
- vesico-umbilical fistula - the urachus does not heal along its full length. The urinary cavity communicates with the external environment directly through the opening in the navel area. This problem manifests itself in the fact that urine is released from the navel;
- umbilical fistula - the area of the urachus does not completely heal in the area near the navel. The urachus cavity communicates with the outside world through an opening located near the navel;
- urachus cyst - in fact, partial fusion of the urachus only in the middle, which causes its expansion into a sac-like shape.
The disease also manifests itself as contracture of the bladder neck. Thus, it narrows, which is caused by a large amount of tissue directly at the mouth of the urination channel, which creates an obstacle to the outflow of urine.
Main causes of pathology
Urinary pathologies are often congenital diseases that develop in the fetus during the period of gestation by the mother. The main risk factors observed in the development of ureteral pathologies:
- the presence of hereditary factors - the appearance of errors directly in the genetic apparatus of the child’s cells in the womb, which cause incorrect structure, as well as the manifestation of pathologies in the development of certain systems and organs;
- environmental hazards associated with professional activities, for example, constant temperature changes, ionizing radiation;
- infectious diseases of the mother during pregnancy, for example, syphilis, rubella and other problems;
Exstrophy disease: features
Occurs in the bladder. It is a developmental defect. The child does not have the anterior wall of the bladder, the abdominal wall (abdominal in front). This pathology occurs in 1 child per 40-50 thousand. newborns. At the same time, the defect is possible in boys much more often than in girls.
The specifics of this anomaly are not yet fully known. As a rule, the defect manifests itself along with splitting of the pubic bones and total epispadias. There are three levels of exstrophy, depending on the size of the abdominal wall defect. It is important to say that the degree is influenced by the distance of divergence of the pubic bones. Diagnosed at birth. In this case, only surgical treatment is possible, the method of which is selected depending on the complexity of the defect.
In the 1st degree of the disease, surgical intervention can be used to close the defect of the abdominal wall located in front. In addition, the bladder is sutured. For grades 2 and 3, the ureters are transplanted into the intestines. As for the urinary tract, it is removed, after which the defect in the abdominal anterior wall is sutured.
Causes of anomalies
Most often, diseases of the genitourinary system associated with developmental anomalies are caused by a number of established factors. These include:
- genetic predisposition (the disease is transmitted at the gene level);
- infectious and venereal diseases suffered during pregnancy;
- exposure to radiation, as well as ionizing radiation;
- addiction to alcohol and tobacco products;
- wrong diet;
- contact with toxic substances;
- use of hormonal drugs.
If an anomaly in the development of the genitourinary system is detected, an examination of all members of the patient’s family is required. In addition, consultation with a specialist will help clarify the situation and calculate the risks of repeating a similar scenario in future generations.
Kidney duplication
One of the most common abnormalities of maturation inside the womb, characteristic of the upper urinary tract, is their duplication. Mostly it is located on one side, in more rare cases it is present on both. In a situation with duplication of the upper urinary tract, there are often two other defects of the ureteric orifices - these include ectopia of the ureteral orifice and ureterocele. In general, pathologies of the upper urinary tract are divided into four fairly large groups:
- anomalies associated with impaired communication of blood vessels with the upper part of the urinary tract;
- partial dysplasia of the ureteral wall;
- ectopia of the ureteric orifices;
- ureterocele.
Moreover, congenital malformations of the urinary tract include all diseases associated with abnormalities in the development of the kidneys. Such an ailment, for example, is kidney doubling. This often diagnosed anomaly is characterized by either duplication of some components of the kidney (pelvis, vessels or ureters), or all of these elements at once, which is called complete duplication of the kidney. In this case, both halves are usually considered independent organs, and the pathological process often affects only one of the organs.
The following developmental anomalies are characteristic of the kidneys: malposition and dystopia. These subtypes of abnormalities are divided into pelvic, iliac, lumbar, thoracic and transverse. At the same time, patients with dystopia often have problems with intestinal activity. In general, without certain clinical manifestations, these types of diseases can remain undetected for a very long period of time.
One of the serious deviations in the formation of the urinary tract is considered to be an anomaly in the relationship of the kidneys, in which the organs grow together. Depending on the type of fusion, they can take different shapes, changing the appearance of the organ to L-shaped, S-shaped and horseshoe-shaped. Kidneys fused with each other are easily subject to inflammatory processes, and in addition can cause renal hypertension. Due to the development of other diseases caused by inflammatory processes (pyelonephritis, hydronephrosis, abnormal blood supply), arterial hypertension can also progress.
Recommended topic:
Pyelocalicectasia of the right and left kidney
Polycystic kidney disease
Another developmental anomaly that is serious is polycystic kidney disease. The disease is most often transmitted genetically and has a dominant type of inheritance. With this ailment, most of the kidney parenchyma is affected by a huge number of hollow tumors (cysts) of different sizes. In 7 out of 10 cases, a child whose organs are affected by polycystic disease is born dead. If the number of tumors is not so large, their performance (and therefore the viability of the body) is maintained, but in many cases there is a high chance of developing renal failure. This disease is often accompanied by polycystic disease of other parts of the body.
Another non-hereditary anomaly is a solitary cyst of the organ in question. This disease involves a single cyst in the kidney, which can be either congenital or acquired. As the size of the cyst increases, renal function is impaired, and patients suffer from lower back pain.
The abnormality known as spongy kidney is characterized by the formation of a large number of tumors in the renal pyramids. This disease usually does not lead to the development of organ failure.
Separately, it is worth considering a ureterocele - this is a protrusion, more like a hernia, inside the ureter. After all, it sometimes provokes dilation of the upper urinary tract, pyelonephritis and urolithiasis.
Diverticulum
This anomaly can be acquired or congenital. It reveals a saccular bulging of the urinary wall. Most often in children this defect is congenital. In this case, the defect is not only single, but also multiple. Placed on the side/back wall of the bladder. As a rule, stagnation of urine is observed in the diverticulum, which affects the formation of cystitis. It happens that the mouth of the ureter opens into it, which can cause pyelonephritis caused by vesicoureteral reflux.
What are the manifestations of this pathology? Children often complain of difficulty urinating. It happens that you have to empty your bowel movements 2 times: first the urinary tract is released, then the diverticulum itself is released.
Treatment is prescribed by a urologist. Initially, a specialist can make a diagnosis based on the results of cystography and cystoscopy. In this case, treatment is performed only surgically. The main goal of the operation is to remove the pathology of the urinary wall.
Urinary diverticula in children can have different locations. However, quite often they are accompanied by problems with urination. Dysuria is possible in situations where the diverticulum is located near the urinary neck, which causes active compression of it. In the presence of acquired diverticula, impaired urination also occurs, which is caused by the formation of this pathology. The appearance of urinary stasis in the bladder due to diverticula in children has an aggravating effect on the condition of children, causing infections leading to chronic pyelonephritis. Chronic kidney failure may also occur. At the same time, urinary stasis in pathology also sometimes causes various complications, in particular, it causes stone formation or the appearance of another formation in its cavity.
It is important to take into account that bladder diverticula may not manifest themselves for a long time. At the same time, after a while, signs of infection in the urinary as well as the upper tract (urinary) begin to appear, which can cause urosepsis.
To facilitate the fight against infectious foci of the urinary tract, as well as to improve the functioning of the kidneys (if there are such disorders), in some cases patients need to undergo a vesical suprapubic fistula in advance. In this case, diverticulectomy is performed only in the second stage.
Vesicoureteral reflux.
This is a very common disease, which is the cause of the development of a large percentage of pyelonephritis in childhood. The fate of the child depends on good knowledge of this disease, timely detection and early treatment. The disease is characterized by insufficiency of the vesicoureteral segment and temporary or permanent return of urine from the bladder to the upper urinary tract. Vesicoureteral reflux is a pathological process and is caused mainly by the reverse return of urine during an increase in pressure in the bladder during urination. There is a slow expansion of the upper urinary tract. Mechanical disorders accompanied by infectious ones complicate reflux with ascending pyelonephritis, which can gradually lead to irreversible renal failure.
Etiology. There are two types of reflux - secondary and primary (congenital).
Secondary vesicoureteral reflux. The mechanism of occurrence of this type of reflux is as follows:
1. When it is caused by an obstruction to the outflow of urine at the level of the bladder neck and urethra, chronic urinary retention occurs in the bladder. Due to increased pressure, the direction of the ureters passing obliquely through the bladder changes, insufficiency occurs and reflux appears.
2. Neurogenic bladder in congenital spina bifida in 30-40% of cases is accompanied by reflux, which is the result of neurogenic damage to the vesicoureteral segment.
3. With cystitis, reflux can also occur. The inflammatory process covers the openings of the ureters, their gaping increases and reflux occurs, which lasts temporarily and disappears after antibiotic therapy. Sometimes this type of reflux is very difficult to distinguish from primary reflux.
4. During operations on the bladder, especially those involving the area of the vesicoureteral segment, the latter may be damaged and reflux may develop. The clinical picture is characterized by symptoms of a chronic inflammatory process.
Primary (congenital) vesicoureteral reflux. It is caused by an anomaly of the vesicoureteral segment and, above all, aplasia of Bell's muscle. With this developmental anomaly, in most cases the position of the ureter is normal. During cystoscopy, its opening is easily detected, since it is hyperemic and edematous. The urine excreted is cloudy. This type of reflux most often occurs in girls aged 3 to 12 years.
Clinic. 1. In infants, the clinical phenomena are unclear (hypotrophy, anemia, gastrointestinal disorders); only a urological examination helps make a diagnosis. In such children, pyuria and albuminuria are present, and in bilateral forms, the urea level reaches 50-80 mg%.
2. Young girls (from 9 months to 7 years) are characterized by periodic increases in temperature, accompanied by pyurea and bacteriuria. Such children develop normally. Hypertheremia occurs without preliminary prodromal phenomena and reaches 40°C within a few hours with symptoms of general infectious intoxication; after a few hours the temperature drops. During febrile attacks, the child experiences pyuria and bacteriuria. Without a urine test, it is very difficult to make a diagnosis. Sometimes such children complain of pain in the lumbar region, especially during urination.
3. In older children, more often in girls aged 8 to 16 years, admitted to the hospital due to anemia, azotemia reaches 100 mg% and sometimes the pressure is moderately elevated. Anamnestic data indicate an increase in temperature without explanation of apparent reasons. When examining urine, pyuria, bacteriuria, and albuminuria are detected.
Diagnosis. It is placed on the basis of excretory urography and ascending voiding cystography performed to detect vesicoureteral reflux.
Treatment depends on the type of reflux. For secondary reflux, surgical treatment is indicated - removal of the obstruction causing chronic urinary retention. After surgery, long-term anti-infective treatment is necessary, after which the reflux usually stops.
For reflux caused by an inflammatory process in the bladder, long-term anti-infective treatment is indicated (orofuran, sulfonamides, nalidix, biseptol, etc.) with a recommendation to perform retrograde cystography every three months to establish regression of reflux. Typically, in 92% of cases, this type of reflux resolves under the influence of conservative treatment.
For primary congenital reflux, surgical treatment is indicated - surgery to remove antireflux. Difficulties are sometimes caused by the fact that some primary refluxes are very similar to inflammatory ones and cannot be accurately differentiated. In such cases, anti-infective treatment is prescribed for three months. A voiding cystography is performed. If the tendency of reflux to decrease is established, this treatment can be continued for another three months. If even after this the reflux has not stopped, but the degree of its development has increased, and, despite treatment, the inflammatory process continues, it is considered that the reflux is primary and surgical intervention is necessary. In cases where, after the third month of drug treatment, reflux does not regress and there is no tendency to stop the urinary infection, the child must still be referred for surgical treatment. After surgery, long-term antibacterial treatment should be carried out, for 6 months - 1 year, with periodic monitoring of urine, as well as excretory urography and retrograde cystography in the presence of uroinfection 3 months after surgery.
Cervical contracture is a urinary problem
A pathology in which an excess of connective tissue appears in the wall of the bladder at its outlet. The disease manifests itself in different ways, depending on its complexity. Both complicated urination and complete retention may occur, which causes severe discomfort in patients. Treatment is prescribed by a doctor only after examination. To make a diagnosis, urethrocystography and urethrocystoscopy are used. During a surgical operation aimed at eliminating cervical contracture, the resulting structure is dissected.
Cause of pathologies
Urinary anomalies are a group of fairly rare diseases. However, most often in medical practice it is the pathologies described above that are encountered.
The causes of diseases associated with the development of urinary tract lie in the impact of negative factors directly on the fetus during the formation of organs in the womb. It is worth noting that non-closure of the urachus is often associated with a failure of the mechanisms leading to its closure.
Note! Self-medication is very dangerous. Entrust the health of your child to experienced doctors who will examine you, prescribe an examination and perform all the necessary manipulations in order to rid your child of bladder pathologies. Now there are many highly specialized clinics in which the child will be provided with all the necessary medical care by specialists with extensive experience.
Abnormalities of kidney structure
Solitary unilateral cyst. The cyst is full of serous contents and is not associated with the renal cavity system. Objectively, it can be palpated as a “kidney tumor” and gives a characteristic image during venous urography. Treatment is surgical for large cysts, and for smaller ones, transcutaneous puncture is performed.
Multilocular unilateral cyst (cystoadenoma). The polycystic mass covers only one kidney and objectively the same changes as described above are found. In young children, cysts cause thinning of the renal parenchyma and lead to nephrectomy.
Polycystic kidney disease of newborns. A rare disease with a very severe course. Both huge polycystic kidneys deform the abdomen of the newborn, who suffers from kidney failure from the day of birth. Such children die before reaching a year of age if they are not put on chronic dialysis.
Juvenile hepatorenal polycystic disease. Both kidneys are large in size, with unsmooth contours due to small cysts located near their surface. The function of the liver is also impaired due to its enormous size due to fibrosis, as in congenital cirrhosis (biliary fibroadenomatosis). Accompanied by portal hypertension with frequent attacks of hematemesis, which are the most common cause of death.
Congenital polycystic kidney disease, similar to the adult type. Occurs in older children. It is a polycystic disease of adults that causes early symptoms in childhood. Treatment is initially conservative, and later, in case of renal failure, chronic analysis and kidney transplantation are performed.
No bladder
Absence of the bladder or agenesis of the bladder is an extremely rare developmental anomaly, combined with multiple malformations that are incompatible with life. If a woman registers her pregnancy with the LCD on time and undergoes screening ultrasounds and fetal hormone studies, such defects are detected in the first half of pregnancy and are an indication for its termination.
Another variant of congenital bladder pathology is the absence of the anterior wall of the bladder or bladder exstrophy. It is also a rare developmental defect, but children with bladder exstrophy do not have any other abnormalities. With this type of malformation, the bladder is located outside the abdominal cavity due to the absence of part of the anterior abdominal wall. Also, the absence of a bladder wall makes it “inverted”; urine flows freely out.
The places where the ureters enter the bladder – the orifices of the ureters – are also formed incorrectly. They have very weak sphincters, which allows urine to flow back into the ureters and contributes to its stagnation in the renal pelvis.
With exstrophy, the urethra and its sphincters are also not formed, in girls the clitoris is split, in boys the penis is split along the upper surface. In children of both sexes, divergence of the pubic bones is observed. The location of the anus changes topically, but practically does not make any adjustments to the functioning of the intestines.
Due to a defect in the anterior abdominal wall, the navel is deformed, located lower than usual, and almost smoothed out.
The absence of urine in the bladder during fetal development deforms the urinary system. Modern technologies in the field of reconstructive urology make it possible to gradually, starting from the first day of life of a person with exstrophy, restore the integrity and functionality of all parts of the urinary system.
Surgical treatment of exstrophy begins in the first day or two of the baby’s life. Prenatal diagnosis of this malformation and timely referral of the mother to a fourth-level hospital with experienced pediatric urologists are very important.
The scope of the first operation depends on the degree of exstrophy and possible concomitant pathologies, and the condition of the baby. Most doctors prefer to immediately restore the integrity of the bladder, reposition it back into the pelvis, reposition the pelvic bones, restore the integrity of the anterior abdominal wall and form the urethra.
When reconstruction is carried out in the first days of a child’s life, repositioning of the pelvic bones is carried out with the least number of complications and the shortest rehabilitation period.
The absence of urine flow into the bladder indicates pathology of the ureters. “Transplantation,” that is, the formation of new ureters from part of the intestine, can also be carried out in the first stage of reconstruction of the urinary tract.
The second stage will be plastic surgery of the genital organs and, if necessary, a bladder transplant.
Types of birth defects
In more than thirty percent of cases, congenital pathologies of the urinary organs are inextricably linked with deviations in the development and functioning of the reproductive system.
The following may be subject to abnormal changes:
- kidneys – pathology can be unilateral or bilateral;
- one of the ureters (less often a pair);
- bladder and urethra;
- reproductive organs (male more often than female).
Defects can affect the structure of tissues and the structure of the organ itself, as well as its blood supply system. An organ may have an atypical location in the body and, accordingly, influence the functioning of all its systems in a certain way.
Deviations in the structure and function of the kidneys
Congenital kidney pathologies may be associated with their location inside the body, the number of organs and their structure, as well as the atypical structure of their circulatory system.
Congenital pathologies of blood vessels providing blood supply to the kidneys:
- The number and location of the renal arteries. In this case, there may be an accessory, double or multiple renal artery.
- Anomalies in the structure and shape of the arterial trunks. These include an aneurysm - a modification of the walls of blood vessels, characterized by the absence of muscle fibers and thickening. Fibromuscular stenosis is an excess of muscle tissue. Arteriovenous fistulas are “bridges” between the venous and arterial systems.
- Congenital modifications of the renal veins - by number: accessory and multiple, by shape and position - ring-shaped, retro-aortic, extracaval.
These abnormalities of the renal vessels are not accompanied by painful symptoms and are detected during the examination of the patient.
However, they can become a “time bomb”, since the rupture of an aneurysm can lead to massive internal bleeding, kidney infarction, fibromuscular dysplasia - to a decrease in the lumen of the renal artery, hypertension, kidney atrophy, nephrosclerosis and other negative phenomena.
There are five groups of deviations:
- number of kidneys;
- sizes;
- location;
- organ tissue structure;
- relationships with other bodies.
Kidney defects:
- Aplasia is the absence of a kidney and its vessels. The bilateral form of this pathology is incompatible with life. With unilateral aplasia, one kidney functions and is enlarged.
- Kidney doubling. The organ consists of two parts fused vertically - upper and lower. It is much longer than normal in length. The half of such a double bud, located on top, is often underdeveloped. Each part of the duplicated organ has its own blood supply system. Doubling can be complete or incomplete, one-sided or two-sided.
- Accessory (third) kidney - has its own blood supply system. The size is smaller than normal, and the location is in the pelvis or iliac region (lower than normal). The third kidney itself is often abnormal. Has its own ureter.
- Hypoplasia is a kidney that is reduced in size, but has normal structure and functionality. “Dwarf kidney” can be one-sided or two-sided. In unilateral cases, the opposite kidney is enlarged in size.
- Dystopia is a deviation from the norm regarding the internal placement of the kidney. Normally, the kidneys are located in the retroperitoneal space; in the case of dystopia, the organ may be in the thoracic or pelvic cavity, in the iliac or lumbar region.
- Spliced kidney. It can be bilaterally symmetrical (“biscuit-shaped” - both kidneys are completely fused, “horseshoe-shaped” - fusion occurs at the upper or lower poles), bilaterally asymmetrical L, S - shaped, unilaterally - L-shaped.
- Dysplasia is a structural anomaly in which the kidney has a reduced size and an abnormal structure of the parenchyma (dwarf, rudimentary).
- Polycystic kidney disease - normal parenchymal tissue is modified in the form of cysts. Only small healthy areas of the organ parenchyma that are not replaced by cysts function. The pathology is bilateral.
- Multicystic kidney - the tissues of the organ are replaced by multiple cysts containing fluid. This kidney does not function.
- Megacalycosis is expansion of the calyces and thinning of the parenchyma.
- Spongy kidney - multiple small cysts in the renal pyramids. In most cases it is bilateral.
Many of these pathologies are associated with abnormalities of the genital organs. In some cases, congenital anomalies become known after infection, when negative symptoms appear. Kidney dystopia may be accompanied by periodic abdominal pain.
The fusion of the kidneys and their abnormal location, as well as the peculiarities of their shapes, can provoke a mechanical effect on the ureters, blood vessels and nerve endings, which causes pain and disruption of the blood supply to the organs. Polycystic kidneys present with multiple symptoms characteristic of renal failure.
Congenital pathologies of the bladder
This organ plays a vital role in the functioning of any living organism. It is designed to collect urine and then remove it from the body.
Anomalies in the development of the bladder are the result of certain disruptions during the intrauterine formation of the unborn child under the influence of a number of unfavorable external or internal factors:
- Agenesis. The bladder and urethra are absent in the fetal body, which is incompatible with life.
- Doubling. The organ is divided into two parts by a longitudinal septum. With complete bifurcation, each part of the bladder has its own urethra and one ureter. Incomplete duplication, called a “two-chambered” bladder, is characterized by the presence of one common urethra and a single neck.
- Diverticulum. This disease is characterized by the presence of sac-like “protrusions” of the bladder walls. Urine accumulates and stagnates in these formations, which contributes to the development of inflammatory processes and the formation of stones. These types of bladder abnormalities can be either congenital or acquired. The most characteristic symptoms are urinary retention, absence of urination, or urination in two stages.
- Exstrophy. A severe congenital defect in which the bladder has no anterior muscular wall, and there is a hole in the lower abdomen with a diameter of several centimeters. The back half of the bladder with the ureters protrudes into this open cavity, from which urine is released out. This anomaly is combined with defects of other organs and splitting of the pubic bones. It can only be treated surgically.
- Anomaly of the urachus (urinary duct between the fetus and amniotic fluid), which should close by birth, but sometimes this does not happen. In such cases, there is an umbilical or vesico-umbilical fistula, cystic formations of this duct, and vesical diverticula.
- Narrowing of the lumen of the bladder neck. Significant growth of fibrous tissue in the neck of the organ, which prevents the outflow of urine from the bladder.
Congenital pathologies of the ureters
These pathologies cause disruption of the processes of excretion of urine from the body. Anomalies of the ureters are quite common among all congenital malformations of the genitourinary system.
Deviations may be as follows:
- the number of ureters is different from normal;
- there is an atypical location and relationship with other organs;
- the shape, structure and size of these organs are abnormal;
- the structure of muscle fibers is different from normal.
Anomalies of the ureters, as a rule, are accompanied by congenital pathologies of other elements of the urinary system - kidneys, bladder, urethra and reproductive organs:
- Agenesis. The urinary organ is absent on the right or left side. Unilateral – accompanied by the absence of a kidney.
- Doubling. Tripling. Characterized by a double (triple) pelvis. It can be complete or incomplete, one-sided or two-sided.
- Retrocaval, retroiliac ureter - rare position anomalies when the ureter intersects with vessels, which lead to compression and obstruction of the ureter.
- Ectopic orifice. Displacement of the ureteric orifice into the bladder neck (intravesical). Extravesical ectopia - displacement of the ureteric orifice into the urethra, rectum, vas deferens, uterus.
- A spiral-shaped annular ureter leads to its compression and the development of hydronephrosis and pyelonephritis.
- A ureterocele is a protrusion of the wall of the ureter into the bladder.
Anomalies of the ureters associated with changes in their structure - hypoplasia (the lumen of the ureter is narrowed, the wall is thinned), neuromuscular dysplasia (lack of muscle fibers in the walls of the organ), achalasia, ureteral valves, ureteral diverticulum.
These anomalies are quite rare and are not always diagnosed in childhood. However, the pathologies associated with them can be very serious. Treatment is most often carried out surgically.
Bladder duplication
Duplication of the bladder is a rare anomaly of intrauterine development in which two bladders are present and functioning in one body.
There are several types of bladder duplication.
two equal bladders, each with its own neck, have one ureter and empty into its own urethra.
two equal bladders are connected by a common neck and flow into one urethra.
one bladder with a complete or incomplete septum inside. The parts of the bubble may be equal or different.
Clinic: frequent urination, incontinence and persistent cystitis.
Treatment is only reconstructive surgery.
Abnormalities of the blood vessels of the kidney
Additional blood vessels. These are veins or arteries emanating from the upper or lower pole of the kidney and supplying an additional specific segment of the renal parenchyma. They can cause congenital hydronephrosis, especially if they cross the pyeloureteral segment. Treatment of hydronephrosis is surgical.
Congenital narrowing and aneurysm of the renal artery. Rare anomalies that cause arterial hypertension. Established using renal arteriography. Treatment is surgical; reconstructive surgery is performed on the renal artery or, if impossible, nephrectomy.
Pathology of the urachus
Pathology of the urachus and vitelline duct are congenital pathologies that occur in children, as well as in adults. Often this pathology does not bring any clinical picture, but this depends on the clinical form. For example, incomplete fusion or non-closure of one of the parts of the urachus can only be found as artifacts during examination for another reason. Complete nonunion, in turn, leads to a number of symptoms, the most basic of which is the discharge of urine from the navel, which, of course, should not be normal.
Typically, the diagnosis of this pathology comes down to determining the pathology based on clinical or instrumental data. For example, pathology of the urachus on ultrasound may not be detected even by an experienced functionologist. In this case, probe examinations of the bladder, as well as insertion of a probe into the umbilical fistula, can help.
Treatment mainly comes down to surgery. The remainder of the urachus is excised (it is reduced into a ligament) using the extraperitoneal method. This type of surgical treatment should relieve the main symptoms and improve the quality of life in the future.
Are you afraid to go to the doctor? specialist online!
Anomalies of the genitourinary organs
The most common are developmental anomalies of the ureters. Diseases in this category make up approximately a fifth of all ailments related to disorders of the genitourinary system. Like other anomalies in the field of urology, these developmental disorders are in many cases accidentally detected in children during examinations related to other diseases, and are also sometimes accompanied by dysfunction of the renal system. Patients are often diagnosed with narrowing or dilatation of the ureter. Despite the huge number of different types of anomalies associated with the ureter, they cause disturbances in urodynamics (the movement of urine through the urinary system). Accordingly, obstruction of urine flow leads to the development of inflammatory processes in the kidneys (for example, cystitis), which causes disruption of its functioning. In many cases, children are diagnosed with several anomalies of the ureters on both sides, which leads to irreversible changes in the kidney. Typically, such malformations are detected between the ages of 6 and 10 years.
Recommended topic:
Hydrocalycosis of the kidneys
Testicular hypoplasia
Anomalies in the development of male genital organs refer to defects in the formation of the genitourinary parts of the body. Most often, abnormal development of the testicle is included in this category, with which 5 to 7 percent of babies are born. Among such deviations, several quantitative ones are distinguished: anorchism (in which both testicles are completely absent), monorchism (there is only one), polyorchism (the number is three or more). Among other anomalies of testicular development, hypoplasia (underdevelopment) of this organ and cryptorchidism (does not descend into the scrotum) are noted. The last anomaly is considered the most frequent of all. Diseases in this category are monitored very carefully by doctors, since their consequences determine whether a boy will be able to have offspring as an adult.
Kidney agenesis
Abnormalities of kidney development are another type of malformation of the genitourinary organs. Problems with their formation are typical for a third of all patients with urological diseases. Due to the frequent detection of such anomalies and the serious consequences of kidney diseases associated with developmental defects, doctors are increasingly attentive to signs that may indicate the presence of any problems. In many cases, timely treatment helps prevent the development of much more serious diseases and avoid serious and sometimes irreversible consequences. In many cases, disorders of kidney development are accompanied by abnormalities in the development of renal vessels. Due to the fact that kidneys with developmental defects have impaired blood circulation and urodynamics, chronic inflammatory processes begin to form in the body. This leads to the fact that kidneys with structural pathologies are more vulnerable to diseases such as pyelonephritis, hydronephrosis and kidney stones. It is important to point out that in the absence of any symptoms and other noticeable manifestations of the disease, abnormalities are sometimes not detected throughout life.
In addition to abnormalities in kidney development, doctors distinguish between problems with the formation of renal vessels. Pathologies of this type are common. The seriousness of such an ailment depends on whether it is accompanied by any kidney disease or whether it is the only type of anomaly of the genitourinary system. In some cases, abnormal renal vessels lead to various kidney ailments, however, the majority of such ailments do not make themselves felt.
Bladder exstrophy
Among congenital pathologies of the urinary tract, along with bladder agenesis, bladder exstrophy is considered the most severe (an example photo can be found on the Internet).
Bladder exstrophy is the absence of the anterior wall of the bladder and the anterior abdominal wall below the navel. The “inverted” bladder gapes outwards, urine flows freely into the amniotic fluid before birth and into the environment after the baby is born.
Bladder exstrophy in children (photos below) is a developmental defect that has no identified cause. This anomaly is multifactorial; it can be triggered by maternal smoking, exposure of the woman to toxic substances, and abdominal trauma at different stages of pregnancy. It is a combined defect; it is always accompanied by the absence of the anterior abdominal wall. Otherwise, the child is absolutely healthy and viable.
It is interesting to note that exstrophy is much more common in boys than in girls, but the mother can carry and pass on the defective gene.
Symptoms of bladder exstrophy are:
- A visually striking defect in the anterior abdominal wall is its absence below the navel;
- Inverted urinary tract protruding into the defect of the anterior abdominal wall;
- Urine flowing freely from the ureters;
- A bright red, inverted bladder, sometimes with a papillary surface.
In most children diagnosed with bladder exstrophy, epispadias goes hand in hand with bladder pathology.
Epispadias is a splitting of the urethra, separation of the pubic bones, splitting of the penis along the upper surface in boys, splitting of the clitoris and vagina in girls.
Complications of this malformation also include fecal incontinence, prolapse of the genital organs in girls due to the inferiority of the pelvic diaphragm, shortening of the penis in boys due to divergence of the pubic bones.
Exstrophy of the bladder can be combined not only with epispadias, but also with other anomalies of the development of the organs of the urinary system, spinal cord, and spine.
This defect is diagnosed in equal parts both at the second screening ultrasound during pregnancy and after childbirth. After the birth of the child, it is recommended to conduct an MRI of the abdominal organs, excretory urography, and ultrasound.
Symptoms and diagnosis of urinary system abnormalities
Anomalies of the urinary system can subsequently lead to the development of cystitis, urethritis, pyelonephritis and so on. The formation of kidney stones is also possible.
Anomalies can be detected using laboratory diagnostic methods: ultrasound, magnetic tomography, palpation, uroflowmetry, cystourethroscopy, computed tomography.
It is important to remember that if you detect an elevated temperature for unknown reasons, as well as loss of appetite, you should immediately contact a urologist.
Sign up for an examination of urinary system anomalies
Make an appointment
Bladder exstrophy. Treatment
Treatment is only surgical. The volume of surgical intervention and their frequency will depend solely on the severity of the defect. With a defect of the anterior abdominal wall up to 4 cm and an isolated defect, surgical treatment can be simultaneous and one-time, the success of treatment and the prognosis in this case will be positive.
For children diagnosed with bladder exstrophy, treatment begins 3-4 days after birth. The best option when diagnosing pathology in utero would be to give birth directly in a perinatal center that specializes in helping children with exstrophy.
If exstrophy of the bladder is isolated and minimally expressed, the operation will be performed once and consist of the following:
- Correction of the position of the pelvic bones - bringing together the pubic bones to “close” the pelvic diaphragm;
- Closure of the bladder defect and its displacement into the pelvic cavity;
- Ensuring the complete release of urine from the urethra;
- Separation of the corpora cavernosa from the pelvic bones for primary lengthening of the penis in boys, vulvo- and vaginoplasty in girls;
- Correction of a defect in the anterior abdominal wall using nearby tissues.
For the treatment of such a pathology as bladder exstrophy, clinical recommendations are based on the experience of leading countries in the field of helping children with this pathology - America, Great Britain. Based on their experience, treatment begins with the first operation during the first days of the baby’s life.
Following the work of European and American colleagues, working with the diagnosis of bladder exstrophy, pediatric surgery in the Russian Federation does not stand still. For more than 20 years, the Moscow Clinic of Pediatric Urology has adopted (and noted the positive effect of observing children undergoing surgery) the experience of early initiation of treatment. In the first month of a baby’s life, the reduction of the pubic bones is most effective and less traumatic; subsequent divergence of the bones is noted to be no more than 4 cm in half of the cases, while in children without reduction of the pubic bones or with later reduction against the background of osteotomy, the divergence of the pubic bones is 15-18 cm .
Unfortunately, all current treatment methods are still unable to achieve a good quality of life with bladder exstrophy. The problems of a non-growing bladder, urinary incontinence, and a high risk of kidney infection due to imperfect genesis of the sphincters of the urinary system remain unresolved.
If exstrophy of the bladder and total epispadias are combined, then the treatment will be multi-stage, long-term, and the discomfort in the child’s life will remain forever.
A striking example of this is four-year-old Ukrainian Ilona Lukyanova with “bladder exstrophy”; the forum will tell about the girl’s pathology from birth and the treatment performed. We also collect financial assistance for expensive uroplasty in Serbia. Unlike citizens of Ukraine who are not protected by the state, citizens of the Russian Federation, if they have compulsory medical insurance, can contact the Research Institute of Urology and receive advice and sign up for treatment, the cost of which will be covered by insurance.
For citizens without a compulsory medical insurance policy and citizens of other countries, consultations and treatment are carried out by appointment for cash or non-cash payment. For patients diagnosed with congenital exstrophy of the bladder (Moscow), the cost of surgery, postoperative observation and rehabilitation is added up and will depend on the complexity of each specific case.
The prognosis for cure is disappointing - discomfort will be an integral part of the life of young patients, urodynamic disturbances are increasing every year, and the risk of renal failure is only growing.
Bladder neck contracture
Bladder neck contracture is a common pathology of the genitourinary system, which occurs in both women and men. The causes of this pathology can be different, ranging from congenital developmental anomalies, to previous surgical interventions, as well as previous infection.
The clinical picture of bladder neck contracture most often manifests itself in disturbances in urination processes, but may also include other symptoms (pain, discomfort in the bladder area).
Treatment of this pathology is exclusively surgical.
What is a pathology of the development of the genitourinary system?
Malformations of the genitourinary system are genetic mutations expressed by the underdevelopment of a particular organ, or, conversely, its hyperdevelopment. Abnormalities include damage to the kidneys, bladder, ureters, urethra, and cause problems in the male and female genitalia. Some may be considered minor, such as duplication of the ureters.
Malformations of the organs of the genitourinary system entail serious consequences, but there are also less dangerous pathologies.
Diverticulum
Diverticulum formation in the bladder.
A diverticulum is a neoplasm that resembles a sac protruding through the wall of the bladder tissue; in fact, it is a hernia. There may be only one such cavity; when there are more of them, we can already talk about diverticulosis. The size of the sacs is very diverse, sometimes they can reach the size of the organ itself, and in rare cases even significantly exceed it.
The location of the pathology, as a rule, is the posterior wall and those located in the lateral segments; other areas are less often affected.
By nature, the disease is presented in two forms - congenital and subsequently formed:
- Congenital (is a true diverticulum) - differs in that it has an identical tissue structure to the bladder.
- Acquired (pseudo-diverticulum) is determined by the absence of a membrane of muscle tissue in the body. Urinary diverticula consist of layers of mucosal and submucosal epithelium.
Bladder diverticulum, causes.
The pathological feature, congenital in nature, of the urinary organ is divided into two types:
- Genetically determined, inherited weakness of the muscle tissue of the lining of the bladder. Here we are talking not about the disease, but about a predisposition to it. A pathological process can be easily provoked by: sudden stress, acute inflammatory process, etc.
- Bladder diverticulum in children is always congenital and is formed in utero under the influence of various factors:
- antisocial habits of a pregnant mother, use and abuse of alcohol-containing products, drug use;
- stress, especially strong or sudden emotional shocks during pregnancy;
- in cases of fetal infection;
- radiation, unfavorable ecology.
The main reasons for the start of the pathological process in the acquired form can be considered infections affecting the genitourinary system, a prerequisite for which is difficulty urinating. Urethritis, cystitis, stranguria, fibroids (in women), adenoma and phimosis (in men), tumor processes, etc.
Constant, forced tension on the walls of the bladder gradually weakens the muscle tissue and causes its atrophy. The weakened fibers of the tissue under the pressure of urine diverge, pushing out part of the mucous membrane, forming a diverticulum.
Congenital detrusor hypertrophy
Detrusor hypertrophy is an enlargement of the bladder muscle that pushes urine out and allows urination to occur. Congenital pathology, in addition to the detrusor anomaly, does not have accompanying anomalies; the state of urodynamics, urethra, etc. is normal. To avoid subsequent complications, it is necessary to remove the underdeveloped muscle and replace it with a loop of intestine.
If left untreated, the child has difficulty urinating and the bladder does not empty completely. The newborn becomes restless and strains. Over time, a large volume of urine accumulates in the bladder because the detrusor is unable to cope with the load. As a result, the bladder stretches, atrophy occurs, followed by atony of the organ.
Diagnostic methods.
There are three main ways to diagnose this disease:
- Cystography (x-ray). The essence of the procedure is to introduce contrast into the bladder. Then, a series of photographs are taken in different projections. Allows you to identify the number of nodes, shape, size of the neck of the formation, the presence of tumors, stones, etc.
- Echography (ultrasound) - the most accurate study will be provided that the Doppler image is in color. Identification of the same parameters as with cystography, plus the position of diverticula in relation to other organs;
- Cystoscopy. Research by inserting a cytoscope into the bladder, and then, if the thickness of the neck allows, of course, penetrating into the diverticulum itself. This allows you to examine and determine in more detail the type of formation, the presence and degree of inflammation, and reflux. Presence and nature of neoplasms, stones, sand, etc.
If the presence of the disease is reliably detected, auxiliary studies are prescribed, such as: uroflowmetry (urine outflow rate.)
Treatment of kidney abnormalities
In cases where developmental anomalies are not complicated, no treatment is required. If a disease occurs against this background, the patient is prescribed therapy, which can be medicinal or surgical in nature:
- therapeutic diet;
- antibiotics;
- antihypertensive drugs;
- cyst puncture;
- angioplasty of the renal arteries, pelvis and ureters;
- organ removal.
For example: with a diagnosis of “urolithiasis”, ICD-10 code No. 20-23, stone-absorbing drugs, painkillers and anti-inflammatory drugs are prescribed.
However, the pathological structure in some cases complicates urine loss, which can lead to complex inflammation that is life-threatening. In such conditions, surgical intervention up to nephrectomy is necessary. First, X-rays are taken in three projections to determine the condition of the second paired organ.
Patients who constitute a risk group should pay increased attention to their own health, undergo periodic tests and undergo instrumental examination, at least an ultrasound scan - once a year.
Diverticula symptoms, treatment:
- 1. Symptoms.
- 2. Diverticulum: treatment.
- Urinary diverticula, open surgery (diverticulectomy). The bladder is removed and the diverticular sac is cut off. At the incision site, each layer of the wall is sutured. A drainage and catheter for urine drainage are installed to prevent pressure on the sutures during the recovery period after surgery.
- Bladder diverticulum, endoscopic surgery. An endoscope is inserted into the inside of the bladder. The device is equipped with a camera and a special device with which you can cut off the diverticulum and cauterize the cut. As in the first case, after the operation a drainage and urinary catheter are installed.
With a small, single formation, the disease can occur with virtually no symptoms. Unpleasant sensations and complications appear when the diverticulum begins to increase in size, or the number of existing ones begins to increase.
The main symptom is the inability to empty the urinary cavity at one time. This is explained by the fact that only the main section of the bladder is released the first time. Then the fluid from the diverticula partially fills the urinary tract again, and the urge to urinate repeats. The duration of the emptying process increases, and may result in a slight purulent discharge.
In addition, constant stagnation of urine in diverticula contributes to the initiation of inflammatory processes, cystitis, urolithiasis, and urological infections. In themselves, these diseases are not signs of diverticulum, but, taking persistent, recurring or even chronic forms, they indirectly indicate the original source of the problem.
The most dangerous type of this pathology is considered to be a form of the disease in which the ureteral duct extends directly into the cavity of the diverticulum.
With this course, the disease can be complicated by the development of ureteral reflux, which in turn can provoke diseases such as hydronephrosis, pyelonephritis. And, subsequently, even cause kidney failure.
The form of the disease does not differ by gender. Symptoms of bladder diverticulum in women do not differ from those in men and in cases of the disease in children.
If the “nodules” are small, the disease occurs in a mild form and does not cause dysuric phenomena (difficulty urinating), stagnation of urine in the cavities - there is no need for surgical intervention, the patient is simply observed by a urologist. For minor inflammatory processes, antiseptic rinsing of the cavities of the bladder diverticulum and treatment with sanitation are performed. In some cases, herbal antibiotics are prescribed.
In case of a complex course, the attending physician may decide on surgical intervention. If there are large diverticula with diverticulosis, surgery is inevitable. There are two types that guarantee effective removal of bladder diverticulum forum:
This technique is more often used for true diverticulum and for patients for whom general anesthesia is contraindicated.
It is important to take into account that the postoperative period is characterized by a long period of rehabilitation. Constant medical supervision is required. Strict compliance by the patient with all recommendations and prescriptions to avoid relapses.