Basic forms, their causes
There are three main forms of acute renal failure (table), which help determine how to take measures to prevent such a complication and treat the pathology:
| Forms | Cause | The situation in which pathology develops | |||
| Prerenal | Appears outside the kidneys (caused by poor circulation) |
| |||
| Renal | Kidney problem |
| |||
| Postrenal | Disturbed urine flow |
| |||
Possible complications
Severe acute renal failure can lead to adverse consequences:
- Pulmonary edema, pleurisy, pneumonia, and respiratory failure may develop.
- Impaired heart rhythm and conduction, cardiac and vascular failure, cardiac tamponade may occur.
- Overhydration or dehydration.
- Cerebral edema, encephalopathy.
- Aseptic peritonitis.
- Lethal outcome – in severe cases reaches 70%.
Acute renal failure requires emergency measures to eliminate renal dysfunction and hemodynamic disorders. Competent diagnosis and timely treatment reduce the risk of serious complications and death. If the slightest dysfunction of the urinary system organs appears, it is very important to immediately consult a specialist or call an emergency medical team.
Source: PochkiMed.ru
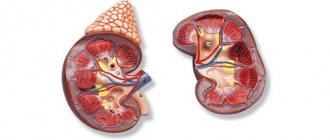
Pathogenesis
Impaired functionality of the renal corpuscles in the cortical layer of the organ, which are an important part of the glomerular structures, determines the pathogenesis of the disease. The destructive impact of functional disorder operates in several directions. First of all, the release of nitrogen end products from the blood is inhibited or completely stopped. With the liquid part of the blood, they are carried throughout the body, entering the internal organs and vital systems. This leads to pollution and disrupts gas exchange in the body. The presence of oxygen in the body decreases, carbon dioxide increases. The glomerular structures of the kidneys suffer from this situation, and their partial or complete necrosis occurs. Restoration of the filtration function when the renal corpuscles die off is practically impossible. In the future, the process is complicated by inflammation, which leads to poisoning of tissues and blood with poisons.
Main criteria for surge arresters
RIFLE classification
In 2002, the rifle classification was developed and published in 2004, allowing the identification and diagnosis of acute kidney injury. Hidden in English letters is the definition of the phases of development of renal failure:
- R - risk;
- I - damage;
- F—failure;
- L—loss of function;
- E - irreparable (terminal) degree of deficiency.
Acute kidney injury is diagnosed when two conditions occur:
- time criterion;
- functional criterion (weakening of organ functions, determined by the amount of urine excreted or the degree of creatinine in the blood).
| RIFLE classification of the development of acute renal failure | ||||||
| Class | Glomerular filtration rate | Diuresis | ||||
| R risk | Increase in Ccr by 1.5 times or decrease in GFR by 25% | <0.5 ml/kg for ≥ 6 hours. | ||||
| I damage | Increase in Ccr by 2 times or decrease in GFR by 50% | <0.5 ml/kg for ≥ 12 hours. | ||||
| F deficiency | Increase in Ccr by 3 times or decrease in GFR by 75% | <0.3 ml/kg for ≥ 24 hours or anuria ≥ 12 hours. | ||||
| L loss of function | AKI for ≥ 4 weeks | |||||
| E irreparable deficiency | ARF for ≥ 3 months | |||||
| Ccr - creatinine level; GFR - glomerular filtration rate | ||||||
AKIN classification
To improve diagnostics by increasing the control of minor deviations in the concentration of creatinine in the blood, the classification was improved in 2007 by a group of AKIN specialists. The emphasis is on the end product of the creatine phosphate reaction and the glomerular filtration rate (GFR) is excluded. Acute renal failure is characterized by the following criteria:
| AKIN diagnostic system | |||||
| Stage | Serum creatinine | Urine volume | |||
| 1 | 1.5-1.9 times normal or an increase of ≥ 0.3 mg/dL | <0.5 ml/kg/h for ≥ 12 h. | |||
| 2 | 2.0 - 2.9 times higher than normal | <0.5 ml/kg/h for 6-12 hours. | |||
| 3 | 3.0 above normal | < 0.3 ml/kg/h in 24 hours or anuria ≥ 12 hours | |||
Symptoms
During the course of the disease in the first stages, the symptoms of acute renal failure are quite vague and insignificant, and the main clinical picture is formed by the manifestations of the disease that led to the disorder.
Gradually, a decrease in the volume of daily urine begins to be recorded, up to 400 milliliters or less, up to anuria (up to 50 milliliters per day). The patient feels nauseous and may vomit, loses appetite, becomes drowsy and lethargic. As the condition progresses, lethargy, confusion, hallucinations, delirium, and convulsions are observed. The skin turns pale and becomes dry, hemorrhages are visible underneath, and progressive swelling is observed. The patient's breathing is rapid and deep. During stethoscopy, cardiac arrhythmias are detected and hypertensive phenomena are recorded. The stool is usually loose and the abdomen may be distended. Further, the deficiency progresses, symptoms of acute poisoning arise, and if measures are not taken, the patient may die.
The stages of acute renal failure are:
- Initial.
- The stage of oligoanuria (the most severe condition, without medical intervention leading to critical consequences for the body).
- Polyuria.
- Recovery.
Some of the symptoms typical for the first stage are described above, but basically they all relate to the underlying disease. To these can be added such characteristic signs of intoxication as anemia and jaundice of the skin.
If the syndrome is caused by glomerulonephritis, there may be blood in the urine, and the process of urine flow is accompanied by pain, and pain in the lumbar area is also observed.
The course of oligoanuria is accompanied by signs:
- a drop in the volume of urine excreted, up to the complete cessation of urination;
- acute intoxication. The patient feels nauseous, the skin itches, breathing quickens, the heart beats quickly and unevenly. Appetite is reduced or absent;
- blood pressure is consistently high;
- consciousness is confused, the patient may faint, and even fall into a coma. Sometimes, especially against the background of injuries and bleeding, a state of shock is observed;
- swelling of the skin and internal organs is observed;
- body weight increases as unremoved fluid accumulates in the body;
- symptoms of general malaise appear.
The further prognosis of the patient’s condition depends on the timeliness and effectiveness of therapy. If therapeutic measures are carried out on time and correctly, there is a high chance of the person returning to normal life: the disorder passes from the stages of oliguria and polyuria to recovery. At the same time, diuresis (as urination is sometimes called in the medical literature) gradually increases, returning to normal. The body is cleansed of toxins, swelling subsides due to the removal of excess fluid.
The polyuria stage poses a certain danger for the patient, since active urine formation is fraught with the development of dehydration and electrolyte disturbances. The condition must be compensated for by fluid intake and diet. The polyuric stage lasts about a month, after which the recovery stage begins, lasting up to 12 months.
The above applies to successful and timely treatment.
If therapy is ineffective or too late, the course of acute renal failure worsens and a set of symptoms develops:
- the patient develops shortness of breath. It is triggered by the accumulation of fluid in the lungs;
- the patient coughs, blood is visible in the sputum;
- multiple hemorrhages occur under the skin and throughout the body;
- the patient loses consciousness and falls into a coma;
- muscles are affected by cramps and spasms;
- the heart rhythm is depressed;
With these signs there is a high probability of death.
Symptoms and stages
The development of acute renal failure goes through 4 stages:
The first is due to the impact of a stress motivator on the body (intoxication, stress, large blood loss). No clinical signs are observed. The overall picture of the disease depends on the reasons that caused the pathological condition.
- The second is characterized by a sharp decrease in urine output by the kidneys. 300-500 ml of urine is released per day - this is oliguria, less than 50 ml is anuria. The products of final metabolism, excreted in a healthy body through the kidneys, in this situation accumulate in the blood. The water-electrolyte balance is disrupted, the renal system for regulating the acid balance is suppressed. The duration depends on the degree of damage to the organ; the condition lasts on average up to 14 days. The patient is accompanied by symptoms of acute renal failure: nausea;
- vomit;
- swelling;
- loss of appetite;
- headache;
- heart rhythm failure.
Emergency care and intensive care for acute renal failure
Treatment of acute renal failure should be started as early as possible. Emergency care is provided in a specialized department by resuscitators. The choice of treatment tactics depends on the cause of development, form and phase of the pathological process. The patient must be hospitalized in the hospital department. A diet and strict bed rest, monitoring of diuresis, blood pressure, monitoring of respiratory rate, heart rate, pulse, saturation, and body temperature are prescribed.
Emergency care in the initial stage of acute renal failure is aimed at eliminating the causative factor and consists of the following treatment:
- Infusion therapy is prescribed to replenish the volume of circulating blood, correct metabolic disorders, and remove the patient from a state of shock. Glucose-saline solutions, Reopoliglucin, fresh frozen plasma of the required group, Hemodez, Albumin are used. Treatment with glucocorticosteroid hormones – Prednisolone, Methylprednisolone – is prescribed.
- Washing the stomach and intestines.
- Removing toxic substances from the bloodstream. Plasmapheresis, replacement blood transfusion, and hemosorption are performed.
- In case of a septic process, antibacterial treatment in a combination of two antibiotics is indicated. The drugs of choice are drugs from the carbopenem group (Tienam, Meronem), Vancomycin.
- In the obstructive form, surgical intervention is performed to restore urine flow. Catheterization of the ureters can be performed; in severe cases, for health reasons, drainage of the kidney or removal of its capsule can be performed.
If the initial stage of acute renal failure has become oliguric, the following is added to treatment:
- Intravenous administration of Furosemide with Dopamine, Mannitol to increase diuresis. Therapy is carried out against the background of a protein-free diet, under strict control of the fluid drunk and excreted, and monitoring of central venous pressure. It is necessary to monitor body weight and monitor urea and electrolyte levels.
- Peritoneal dialysis or hemodialysis. Prescribed when the therapy is ineffective, when the level of potassium and urea increases according to biochemical analysis.
In the polyuric stage of acute renal failure, treatment is aimed at correcting electrolyte disturbances and combating dehydration. The losses of sodium and potassium are replenished with appropriate medications. Rehydration is carried out with glucose-saline solutions intravenously or orally. Dietary nutrition is changing - the consumption of salt and water is not limited. The diet includes foods rich in potassium. As diuresis normalizes, the amount of rehydration solutions decreases.
Acute failure during pregnancy
Acute kidney disease during pregnancy is a life-threatening complication. The danger is that kidney damage always appears quickly, within a few hours or days. Most often, the problem makes itself felt at the beginning of the third trimester, after childbirth. But there is a risk when acute renal failure develops due to infectious diseases. The reasons for the development of pathology during pregnancy are as follows:
- increased load on the kidneys due to more blood being filtered;
- chronic inflammatory processes of the urinary system;
- exacerbation after abortion or after childbirth;
- fetal death during pregnancy.
With timely attention to the signs of acute renal failure (back pain, decreased urination, thirst, and others), it is possible to restore the functionality of the organ and save the life of mother and child.
If measures are not taken in a timely manner, the disease goes through all periods of acute renal failure, new signs are added (blood in the stool, numbness in the limbs) and there is a high probability of death for both the woman and the fetus. In the acute course of the disease, the expectant mother should definitely consult not only a urologist, but also a gynecologist.
Reasons for the development of the condition
Various pathologies lead to deficiency, which doctors assigned the following classification:
- prerenal (extrarenal) – diseases leading to disruption and slowing of blood circulation in the kidneys;
- renal – problems with the kidneys themselves. Renal diseases include pathologies of renal tissues of various origins - intoxication, tumors, ischemic disorders, inflammation, etc.;
- obstructive or postrenal - problems that give rise to the syndrome of acute obstruction of the urinary organs.
Prerenal disorders in this classification occupy a leading place among the causes of deficiency (up to 80 percent of all diagnosed cases). Their important feature is reversibility: for the most part, these pathologies can be cured, with complete restoration of renal function. An exception to this rule is tubular ischemia and necrosis of organ tissue, the fight against which will be difficult.
Among the prerenal causes of renal syndrome:
- pulmonary artery thrombosis;
- blood loss after injuries and surgical interventions;
- pathologies of the heart muscle, accompanied by a decrease in its blood output;
- burns of large areas of the body;
- dehydration of the body for various reasons;
- drop in vascular tone;
- effect of diuretic drugs.
Renal causes are damage to organs due to injury or disease. On average, renal disorder accounts for about a fifth of all reasons for the diagnosis in question. Renal problems of renal origin can affect the entire complex of tissues: tubules, glomerular system, interstitium (tissue connecting these components). Diseases can be either infectious or inflammatory in nature, or caused by vascular pathologies, allergies, or immunological problems.
The abundance of breakdown products in the blood from extrarenal foci of diseases can also lead to a decline in their natural function, provoking renal syndrome. There are often cases of complex influence of several negative factors at once.
The main causes of acute renal failure in this category:
- intoxication with poisons (including from insect bites, reptiles), drug components, heavy metals and compounds used in radiography, etc.;
- a common cause of the disorder is pyelonephritis, glomerulonephritis and similar pathologies of the urinary system;
- atherosclerosis, thrombosis, vascular aneurysms and other similar disorders;
- the cause may be mechanical damage to tissue due to injury.
Postrenal (obstructive) causes are pathologies of the collecting and excretory parts of the urinary system. They account for about ten percent of diagnosed cases. Postrenal failure occurs due to an acute disturbance of urodynamics, with urine drainage becoming difficult, although the kidneys are functioning normally. Sometimes there is a possibility of developing ischemia, since the pelvis, overfilled with accumulated urine, puts pressure on the surrounding tissues, which is reflected in postrenal symptoms.
Obstructive phenomena of the postrenal variety arise due to:
- spasmodic bladder sphincter;
- tumors of the bladder and prostate, pelvic organs, urinary tract;
- hematomas and various injuries;
- inflammation of the bladder and ureters, causing postrenal symptoms;
- congenital structural anomalies in an adult or child.
In rare cases, acute renal failure can develop in pregnant women.
Complications and consequences
Acute kidney diseases do not go smoothly, and significant pathological outcomes often occur:
Violation of water-salt balance can result in sudden cardiac arrest.
- The changes that occur suppress the formation of red blood cells, which leads to the development of anemia.
- Against the background of kidney failure, the body's immune forces decrease. There is a high probability of infectious diseases being associated. The most dangerous thing is sepsis.
- Deviations in the nervous system leading to lethargy and disorientation.
- Disturbances in the functioning of the cardiovascular system lead to the development of heart failure and the appearance of arrhythmia.
- Difficulties in the functioning of the gastrointestinal tract can lead to the development of an inflammatory process complicated by bleeding.
- Against the background of liver problems, hepatic-renal failure develops.
Methods for making a diagnosis and finding out the causes
Diagnosis of acute renal failure is carried out by tests in the laboratory, samples taken from the patient, and instrumental methods for determining diseases. In the laboratory, the following is revealed:
- hemoglobin level, red blood cell sedimentation rate and number of leukocytes per unit volume of blood;
- make diagnostics on the concentration of protein in the urine and the density of the liquid, establish the presence of various blood components in urine and their concentration;
- the presence of uric acid and creatinine in the blood, their level, as well as the ratio of microelements concentrations.
Instrumental diagnostic methods:
- Electrocardiogram. Its results visualize the functioning of the heart muscle and allow precise identification of disorders associated, for example, with hyperkalemia.
- Ultrasound examination. This method determines the size of organs, the level and quality of their blood supply, and identifies obstructive phenomena.
- Tissue biopsy. The samples taken are used to determine tumors, foci of infection, and other pathological changes.
An X-ray examination is important to determine the condition of the heart and lungs.
Diagnosis of acute renal failure
If acute failure is suspected, the doctor takes into account the history of symptoms and examination of the patient. Further clinical recommendations are supported by the results of cfo and laboratory tests:
- Blood analysis. Helps determine: potassium level;
- nitrogenous compounds;
- number of red blood cells, platelets;
- presence of infection.
Analysis of urine. Allows you to assess the degree of organ damage by the presence of sediment in urine. In addition, it is determined:
- By assessing the volume of daily urine, the water-salt balance in the body is monitored. To do this, urine is collected over the course of one day; its amount may be less than normal.
Determination of leukocyte cells as a consequence of an allergic reaction.
Diagnostic methods using mechanical instruments allow you to examine the organ and assess the difficulties of the process (chronic or acute), determine the presence of blockage of the ducts:
- Ultrasound of the peritoneum;
- CT (computed tomography);
- X-ray of the peritoneum determines the presence of stones in the kidneys or ducts.
If the cause of the acute condition is blockage of the ducts, additional types of studies may be needed:
- MRI, which allows you to assess the degree of change in the structure of the organ.
- Kidney pyelography. Through catheterization of the ureter, contrast is introduced for a detailed anatomical study of the organs of the urinary system.
- Renal scintigraphy. Evaluates the functional state of the organ.
Clinical manifestations:
1. The presence of a provoking factor: running, jumping, riding a bicycle, motorcycle, walking, but sometimes an attack occurs at rest.
- The attack usually begins suddenly. The intensity of the pain syndrome may vary. The pain is initially felt in the lumbar region from the side of the diseased kidney and spreads along the ureter towards the bladder and genitals. The patient is excited, rushes about, takes a forced position. An increased urge to urinate and cutting pain in the urethra may occur. Nausea, vomiting. Marked weakness.
- Possible increased body temperature, chills, hyperhidrosis.
- Blood tests: leukocytosis, accelerated ESR.
- The duration of renal colic ranges from several minutes to several hours. Less commonly, an attack with short breaks can last for several days.
Differential diagnosis:
acute surgical pathology of the abdominal organs (attack of cholelithiasis, acute cholecystopancreatitis, appendicitis, intestinal obstruction); inflammatory diseases of the pelvic organs; dissecting aortic aneurysm; intervertebral disc herniation; Exacerbation of chronic intestinal diseases, diverticulitis.
What treatment is needed?
The manifestation of symptoms indicating the development of an acute form of the disease indicates the need to deliver medical assistance to the patient as soon as possible. Until the doctor arrives, people nearby will need self-control to assess the situation and provide the necessary first aid.
Urgent Care
The necessary assistance in the first phase of the development of the disease will be of a more preventive nature, aimed at eliminating the causes that caused the acute condition and eliminating the violations that have occurred. To begin with, the patient is provided with bed rest, rest and warmth. To restore blood movement through the vessels, drip therapy is carried out using solutions of albumin, glucose, mannitol, plasma and others. After blood volume is restored, diuretics are used. Vascular spasms are relieved with novocaine mixtures.
Emergency care for acute renal failure during the development of the second phase is aimed at eliminating symptoms, since the situation is complicated by anuria or oliguria. Treatment of acute renal failure is concentrated on eliminating the consequences of poisoning of the body. All conditions that threaten the patient’s life are prevented and eliminated. Hypertonic solutions, vitamin preparations, anticonvulsants and antibiotics are used.
Effective treatment
Drug therapy is carried out in the intensive care unit, taking into account the complexity of the process and the cause. Acute renal failure is not a primary disease, so first restore blood supply to the kidneys, eliminate blood loss, and improve heart function. After eliminating the root causes, you will need funds to restore kidney function:
- antibiotic;
- a drug to compensate for fluid volume;
- diuretic;
- medications to support heart function;
- medications that improve blood flow;
- gastric lavage (in case of poisoning).
Acute renal failure syndrome is a highly fatal condition. The earlier treatment is started, the greater the likelihood of recovery.
Emergency care for acute adrenal insufficiency in children
⇐ PreviousPage 4 of 4
Acute adrenal insufficiency is a life-threatening condition for a child, the severity of which is caused by a sharp and rapid decrease in the concentration of gluco- and mineralocorticoids with progressively increasing dehydration, gastrointestinal disorders, cardiovascular failure and the risk of cardiac arrest due to hyperkalemia.
Clinical diagnosis
Characteristic, first of all, is the suddenness and severity of the increase in the severity of the child’s condition. The main clinical manifestations of acute adrenal insufficiency:
vascular collapse, developing in phases (sympathicotonic - vagotonic - paralytic phases): rapidly progressive decrease in blood pressure to 30-40 mm Hg. Art., weak pulse, muffled heart sounds, tachycardia followed by bradycardia, acrocyanosis, marbling of the skin, decreased diuresis up to oligoanuria;
abdominal syndrome: repeated vomiting, profuse loose stools without pathological impurities, cramping abdominal pain;
neurological disorders: severe weakness, muscle hypotension, adynamia, later - loss of consciousness, convulsions, meningeal symptoms, hyperthermia, which is subsequently replaced by hypothermia;
cutaneous hemorrhagic syndrome: star-shaped hemorrhagic rash, ecchymoses, with Waterhouse-Friderichsen syndrome - purple-bluish spots on the skin of the torso and limbs, there may be vomiting “coffee grounds”, bleeding from injection sites.
In acute adrenal insufficiency, there is usually no time for laboratory confirmation. Laboratory data are nonspecific: hyponatremia, hypochloremia with simultaneous hyperkalemia, hypoglycemia, increased residual nitrogen and urea in the blood serum, decreased blood pH, coagulogram - signs of the I-III stage of DIC syndrome, ECG - signs of hyperkalemia (lengthening of the PQ interval, widening of the QRS complex , tall pointed T wave), microproteinuria, hematuria, maybe acetonuria.
Differential diagnosis is carried out with intestinal infections, poisoning, comatose states of various origins, acute surgical diseases of the abdominal organs!
Treatment must be started immediately, as minutes play a role in its outcome!
Urgent Care
1. Provide access to the vein and urgently administer for rehydration:
IV jet plasma;
then establish an intravenous drip of 5-10% glucose solution and 0.9% sodium chloride solution in a ratio of 1:1 or 1:2 (with severe dehydration) at a rate of 100-150 ml/kg at an early age, 80- 100 ml/kg - in preschool age and 50-75 ml/kg - in school age (daily doses).
Do not use potassium supplements!
2. Simultaneously with the start of rehydration, prescribe hormone replacement therapy with hydrocortisone (better!) or prednisolone. The first dose of the drug is 50% of the daily dose:
1/2 of this dose should be administered intravenously and
Inject 1/2 dose intramuscularly to create a hormone depot.
The remaining dose is distributed evenly every 3-4 hours (in severe conditions - every 2 hours during the first 6 hours).
3. In case of intractable vascular insufficiency or in the absence of hydrocortisone, administer:
deoxycorticosterone acetate solution (DOXA) at a rate of 1 mg/kg per day IM; the first dose is 50% of the daily dose, the rest is administered evenly after 8 hours.
4. If blood pressure cannot be raised, then it is necessary to prescribe:
microjet intravenous injection of dopamine 8-10 mcg/kg min under the control of blood pressure and heart rate or
0.2% norepinephrine solution 0.1 ml/year of life IV or
1% solution of mezaton 0.1 ml/year of life i.v.
5. For convulsions and low blood sugar, administer a 20-40% glucose solution at a dose of 2 ml/kg intravenously.
6. Oxygen therapy.
7. Correction of hemocoagulation disorders depending on the stage of DIC syndrome.
8. It is mandatory to prescribe broad-spectrum antibacterial therapy for prophylactic or therapeutic purposes.
Hospitalization in the intensive care unit due to emergency measures.
, emergency care for acute renal failure in children. Acute renal failure (ARF) is an acutely developing, potentially reversible syndrome, characterized by a sudden total impairment of renal function in ensuring homeostasis, manifested clinically by disturbances in water-electrolyte metabolism and the acid-base state of the blood, an increase in azotemia with the development of uremia, and pathological damage to almost all systems and functions of the body. .
Depending on the cause, there are prerenal, postrenal and renal forms of acute renal failure.
Clinical diagnosis
The course of acute renal failure is staged, with the initial period usually lasting from 3 hours to 3 days, oligoanuric - from several days to 3 weeks, polyuric - 1-6 weeks or more (up to 3 months), the recovery stage - up to 2 years.
The initial stage of acute renal failure (preanuric - functional renal failure) is manifested by symptoms of the underlying disease and a decrease in diuresis, which has not yet reached stable oliguria. For early recognition of the transition to the oligoanuric stage of acute renal failure, it is necessary to take into account hourly diuresis.
Oliguria - diuresis less than 300 ml/m2 body surface area per day or less than 0.5 ml/kg per hour, or less than 1/3 of the age-related daily diuresis (see Appendix). Anuria - diuresis less than 60 ml/m2 per day or less than 50 ml/day. The exception is newborns in the first 3-4 days of life, when diuresis may be absent even in healthy children, as well as newborns older than 7 days and children under 3 months, when oliguria is considered to be a decrease in diuresis of less than 1 ml/kg per hour.
In the oligoanuric stage of acute renal failure, a threatening condition develops primarily due to overhydration, electrolyte imbalance and uremic intoxication. Overhydration can be extracellular in nature (increase in body weight, peripheral and cavitary edema) and/or intracellular (edema of the brain, lungs). Brain edema (angiospastic encephalopathy) is manifested by an increase in headache, agitation, vomiting, decreased hearing and vision, muscle twitching with increased tone and tendon reflexes, and subsequently coma and convulsions. Another real complication of the resulting hydremia is acute heart failure of the left ventricular type, up to pulmonary edema: sudden shortness of breath of the inspiratory type, scattered wheezing in the lungs, muffled heart sounds, rapid, weak pulse (for more details, see the section “Pulmonary edema”).
Developing uremic intoxication may be indicated by: increasing adynamia, lethargy up to the development of coma, anorexia, dyspeptic manifestations, the addition of toxic stomatitis and gastroenteritis, Kussmaul respiration, in the blood serum - an increase in urea and/or creatinine.
In the oligoanuric stage of acute renal failure, peripheral blood tests show anemia and a decrease in hematocrit. Urinary syndrome is characterized by hypoisosthenuria, proteinuria with hematuria and leukocyturia. The main causes of death: overhydration with the development of cerebral and pulmonary edema, hyperkalemia (cardiac arrest), decompensated acidosis (less commonly, alkalosis), intoxication, sepsis.
The polyuric stage of acute renal failure (the stage of diuresis restoration) is characterized by a gradual increase in diuresis followed by a decrease in azotemia. Due to polyuria, due to the failure of the tubules, electrolyte disturbances (hypokalemia, hypocalcemia, etc.), dangerous dehydration with loss of body weight may occur, and therefore this stage is also often called critical. Clinical manifestations of hypokalemia: lethargy, lethargy, muscle hypotonia, hyporeflexia, possible paresis, cardiac disorders (bradycardia, conduction disorders); on the ECG - flattening and inversion of the T wave, an increase in the prominence of the U wave and deflection of the ST segment (see Appendix). In the polyuric stage, death is possible from cardiac arrest (hypokalemia) or from a septic process.
Treatment of a child with developed acute renal failure is carried out in a specialized hemodialysis department or intensive care unit, differentiated depending on the stage of the process and the etiological factor.
Urgent Care
Initial stage of acute renal failure
1. Treatment of the underlying disease. In case of hypovolemia and shock - restoration of bcc with solutions of rheopolyglucin (polyglucin), 10% glucose, 0.9% sodium chloride according to generally accepted principles under the control of central venous pressure, blood pressure, diuresis.
2. To stimulate diuresis:
for hypovolemia, 15% mannitol solution at a dose of 0.2-0.4 g/kg (by dry matter) intravenously; if there is no increase in diuresis after administering half the dose, further administration is contraindicated; mannitol is also contraindicated in heart failure and hypervolemia;
against the background of sufficient replenishment of blood volume, 2% Lasix solution at a dose of 2 mg/kg IV; if there is no response, repeat the administration after 2 hours in a double dose; In order to enhance the diuretic effect of Lasix, simultaneous administration of titrated dopamine at a dose of 1-4.5 mcg/kg per minute is possible.
3. Prescription of drugs that improve renal blood flow:
2.4% aminophylline solution 1.0 ml/year of life per day IV;
2% solution of trental at a dose of 1-2 mg/kg IV or 0.5% solution of chirantil at a dose of 3-5 mg/kg IV.
https://malyok.ru/index.php/neotlozhnaya-pomochsh-detey/103-2011-12-04-12-02-43
Emergency care for acute cardiac arrest (clinical death) in children.
Cardiac arrest is a sudden and complete cessation of effective cardiac activity with or without bioelectrical activity.
⇐ Previous4
Recommended pages:
Proper nutrition
The pathophysiology of acute renal failure (protein deficiency, water-salt balance, fat metabolism) requires adherence to a special diet. The diet for acute renal failure is quite strict; it is difficult to adhere to due to the large number of restrictions. But this is one of the most effective ways to stop the development of pathology. What types of foods can you eat and what should you remove from your diet? The basic algorithm of dietary nutrition consists of reducing:
- squirrel;
- salt;
- phosphorus;
- potassium;
- liquids.
The second important task of the diet is to provide energy value. The emphasis is on vegetable fats, since proteins are prohibited. Porridges that are excellent for the diet include corn grits and rice. A small amount of wine is allowed. It is important to stimulate appetite; to do this, adhere to the following rules:
- frequent meals, in small portions;
- give preference to solid products first, and only then liquid ones;
- It is not recommended to drink before or after eating;
- Remove unpleasant taste in the mouth with lemon.
Symptomatic features
Severe progression of the listed diseases can lead to acute renal failure at any time. The dangerous condition goes through 4 stages of its development, each of which has characteristic symptoms.
The specificity of this period is the vivid manifestation of the background disease, the state of sepsis and renal colic. The duration of the phase is from 3 hours to 3 days. Intensive disruption of the blood supply to the kidneys begins. It is extremely important to provide emergency care for acute renal failure at this time. This way you can stop the development of pathology.
The period can last up to 3 weeks. Its characteristic feature is the rapid development of oliguria (diuresis less than 300 ml/m2 per day) or anuria (lack of urine). Laboratory tests will reveal the presence of proteins and red blood cells in the urine, and an increased amount of sodium. The concentration capabilities of the kidneys are rapidly declining. Blood pressure is higher than normal. Biochemical analysis will show increased concentrations of urea, phosphate and creatinine.
There are pronounced symptoms of intoxication:
The development of the septic process is accompanied by chills and fever. A general blood test reveals anemia and an extremely low platelet level against the background of pronounced leukocytosis.
Without the necessary help, swelling of the brain and lungs will occur.
The stage is called recovery. Its duration can reach 3 months. There is a gradual, persistent increase in urine production and excretion. Sometimes the secretion of biological fluid reaches 4 liters per day. The consequence of rapid fluid loss is dehydration, and the concentration of potassium and sodium decreases.
Lasts longer than all other stages - up to 2 years.
Systemic blood flow and kidney function are gradually restored. The causes of acute renal failure are completely eliminated. This time is devoted to rehabilitation therapy and sanatorium-resort treatment.
Prognosis for acute renal failure
Modern medicine has enough opportunities to restore the functionality of an organ. The kidneys are gradually able to restore their functionality. But renal failure is an exacerbation that often leads to death. The prognosis is influenced by the severity of the disease. In the acute stage of development of the process, in 20 to 50% of cases, treatment of the disease ends in death. Reasons for this outcome:
- sepsis;
- nervous system disorders;
- circulatory complications.
If you consult a doctor in a timely manner, avoiding complications, kidney function is restored in 90% of all cases. Chronic processes require constant monitoring, but after the introduction of hemodialysis and transplantation into therapy, the mortality rate of people with kidney problems has decreased significantly.
Description
Acute kidney failure, or AKI, as mentioned above, is a severe kidney disorder in which the organs' ability to filter and purify the blood is significantly impaired, to the point of complete loss of this function.
As a result of this disorder, a disruption in normal metabolism occurs:
- Normally, the products of nitrogen metabolism are filtered by the kidneys and excreted in the urine.
- If there is insufficiency, they accumulate in the blood, provoking further metabolic disorders.
The acute syndrome develops quite quickly after its onset. On average, the full manifestation of the clinical picture takes from a day to one week, but in particularly severe conditions the disease may progress in just a few hours.
Despite the severity and danger of the condition of renal failure, the prognosis for its treatment is quite favorable - subject to timely consultation with a doctor and adequate treatment. In this case, renal function is likely to be fully restored. If the acute condition is ignored, delaying the visit to the doctor, or the patient is treated incorrectly, there is a possibility of his death from acute intoxication with unresolved decomposition products. If the kidneys are damaged beyond repair, a person can only be cured by transplanting donor organs.
Acute renal failure does not appear on its own, as a separate pathology; the syndrome always accompanies some diseases and becomes their symptom.
Prevention
In order to prevent erroneous actions, national recommendations have been prescribed. The main prevention consists of timely treatment of diseases. The necessary treatment prevents or minimizes kidney damage. In addition, it is important to be careful when taking medications. You should not take medications without medical supervision. People with diabetes, hypertension, and glomerular nephritis are at risk. It is important for such people to be under constant medical supervision and undergo regular examinations.