A set of specific symptoms (syndrome) that appear as a result of disruption of the proper functioning of the kidneys is called renal failure. This condition is serious, and with rapid or prolonged development, it threatens the patient’s life.
Many patients are interested in symptoms and folk remedies for the treatment of kidney failure in order to carry out therapy at home. It is important to understand that the clinical picture of kidney failure can be quite non-specific, so it is important to consult with a specialist before starting to take medications or folk remedies.
Criteria for chronic renal failure
The diagnosis of chronic renal failure is made if the patient has one of two types of renal disorders for 3 months or more:
- Damage to the kidneys with disruption of their structure and function, which are determined by laboratory or instrumental diagnostic methods. In this case, GFR may decrease or remain normal.
- There is a decrease in GFR of less than 60 ml per minute in combination with or without kidney damage. This rate of filtration corresponds to the death of about half of the nephrons of the kidneys.
What leads to chronic renal failure
Almost any chronic kidney disease without treatment can sooner or later lead to nephrosclerosis with the failure of the kidneys to function normally. That is, without timely treatment, such an outcome of any kidney disease such as chronic renal failure is just a matter of time. However, cardiovascular pathologies, endocrine diseases, and systemic diseases can lead to renal failure.
- Kidney diseases: chronic glomerulonephritis, chronic tubulointerstitial nephritis, renal tuberculosis, hydronephrosis, polycystic kidney disease, nephrolithiasis.
- Pathologies of the urinary tract: urolithiasis, urethral strictures.
- Cardiovascular diseases: arterial hypertension, atherosclerosis, incl. angiosclerosis of the renal vessels.
- Endocrine pathologies: diabetes mellitus.
- Systemic diseases: renal amyloidosis,.
How does chronic renal failure develop?
The process of replacing the affected glomeruli of the kidney with scar tissue is simultaneously accompanied by functional compensatory changes in the remaining ones. Therefore, chronic renal failure develops gradually, passing through several stages in its course. The main reason for pathological changes in the body is a decrease in the rate of blood filtration in the glomerulus. The normal glomerular filtration rate is 100-120 ml per minute. An indirect indicator by which one can judge GFR is blood creatinine.
- The first stage of chronic renal failure is initial
At the same time, the glomerular filtration rate remains at the level of 90 ml per minute (normal variant). There is confirmed kidney damage.
- Second stage
It suggests kidney damage with a slight decrease in GFR in the range of 89-60. For older people, in the absence of structural damage to the kidneys, such indicators are considered normal.
- Third stage
In the third moderate stage, GFR drops to 60-30 ml per minute. At the same time, the process occurring in the kidneys is often hidden from view. There is no bright clinic. There may be an increase in the volume of urine excreted, a moderate decrease in the number of red blood cells and hemoglobin (anemia) and associated weakness, lethargy, decreased performance, pale skin and mucous membranes, brittle nails, hair loss, dry skin, decreased appetite. About half of the patients experience an increase in blood pressure (mainly diastolic, i.e. lower).
- Fourth stage
It is called conservative because it can be controlled by medications and, like the first, does not require blood purification using hardware methods (hemodialysis). At the same time, glomerular filtration is maintained at a level of 15-29 ml per minute. Clinical signs of renal failure appear: severe weakness, decreased ability to work due to anemia. The volume of urine excreted increases, significant urination at night with frequent urges at night (nocturia). Approximately half of patients suffer from high blood pressure.
- Fifth stage
The fifth stage of renal failure is called terminal, i.e. final. When glomerular filtration decreases below 15 ml per minute, the amount of urine excreted drops (oliguria) until it is completely absent in the outcome of the condition (anuria). All signs of poisoning of the body with nitrogenous wastes (uremia) appear against the background of water-electrolyte imbalance, damage to all organs and systems (primarily the nervous system, heart muscle). With this development of events, the patient’s life directly depends on blood dialysis (cleaning it bypassing non-functioning kidneys). Without hemodialysis or kidney transplantation, patients die.
Chemical composition of urine in pregnant women
| Amount of urine per day | 800-1500 ml |
| Protein in the morning portion | Missing or traces |
| Protein per day | 0-0.300 g/day |
| Amino acids | 0.1-0.3 g/day |
| Total nitrogen | 10-20 g/day |
| Urea | 330-580 mmol/l |
| Uric acid | 2.4-6.0 mmol/l |
| Creatinine | 53-159 µmol/day |
| Sodium | 135 (100-170) mol/l |
| Potassium | 45 (35-60) mol/l |
| Chlorine | 135 (100-170) mol/l |
| Medium molecule level | 0.3-0.33 units. |
DETAILS: Protein in a child’s urine is normal. Increased protein in the urine of a child - causes, treatment
Table 11
| Total protein | 70 (60-80) g/l |
| Albumin | 40 (30-50) g/l |
| Globulins | 30 (20-40) g/l |
| Albumin-globulin ratio | 1,3 (1,2-1,4) |
| Sodium | 141 (130-150) mmol/l |
| Potassium | 4.5 (3.6-5.4) mmol/l |
| Calcium | 2.5 (2.2-2.7) mmol/l |
| Chlorides | 101 (98-106) mmol/l |
| Bicarbonates | 27 (24-33) mmol/l |
| Glucose | 5.3 (4.4-5.8) mmol/l |
| Bilirubin | 8.5-20.5 µmol/l |
| Residual nitrogen | 0.2-0.4 g/l |
| Urea | 2.65-6.84 mmol/l |
| Creatinine | 44-97 µmol/l |
| Uric acid | 0.16-0.4 mmol/l |
| Cholesterol | 4.5 (3.1-7.8) mol/l |
| Medium molecule level | 0.22-0.26 units. |
Symptoms of chronic renal failure
Appearance of patients
The appearance does not suffer until the stage when glomerular filtration is significantly reduced.
- Due to anemia, pallor appears, due to water and electrolyte disturbances, dry skin.
- As the process progresses, yellowness of the skin and mucous membranes appears and their elasticity decreases.
- Spontaneous bleeding and bruising may occur.
- This causes scratching.
- Characterized by so-called renal edema with puffiness of the face, up to the common type of anasarca.
- The muscles also lose tone and become flabby, which causes fatigue to increase and the ability of patients to work decreases.
Nervous system lesions
This is manifested by apathy, night sleep disorders and daytime sleepiness. Decreased memory and learning ability. As chronic renal failure increases, severe inhibition and disturbances in the ability to remember and think appear.
Disturbances in the peripheral part of the nervous system affect the limbs with chilliness, tingling sensations, and crawling sensations. Later, movement disorders in the arms and legs develop.
Urinary function
She first suffers from polyuria (increased urine volume) with a predominance of nighttime urination. Further, chronic renal failure develops along the path of a decrease in urine volume and the development of edematous syndrome until the complete absence of excretion.
Water-salt balance
- salt imbalance manifests itself as increased thirst, dry mouth
- weakness, darkening of the eyes when standing up suddenly (due to sodium loss)
- Excess potassium may cause muscle paralysis
- breathing problems
- slowing of heartbeats, arrhythmias, intracardiac blockades up to cardiac arrest.
Against the background of increased production of parathyroid hormone by the parathyroid glands, high levels of phosphorus and low levels of calcium appear in the blood. This leads to softening of the bones, spontaneous fractures, and itchy skin.
Nitrogen balance disorders
They cause an increase in blood creatinine, uric acid and urea, resulting in:
- when GFR is less than 40 ml per minute, enterocolitis develops (damage to the small and large intestines with pain, bloating, frequent loose stools)
- ammonia odor from the mouth
- secondary articular lesions such as gout.
The cardiovascular system
- firstly, it responds by increasing blood pressure
- secondly, damage to the heart (muscles - pericarditis, pericarditis)
- Dull pain in the heart, heart rhythm disturbances, shortness of breath, swelling in the legs, and enlarged liver appear.
- If myocarditis progresses unfavorably, the patient may die due to acute heart failure.
- pericarditis can occur with the accumulation of fluid in the pericardial sac or the loss of uric acid crystals in it, which, in addition to pain and expansion of the borders of the heart, when listening to the chest, gives a characteristic (“funeral”) pericardial friction noise.
Hematopoiesis
Against the background of a deficiency in the production of erythropoietin by the kidneys, hematopoiesis slows down. The result is anemia, which manifests itself very early in weakness, lethargy, and decreased performance.
Pulmonary complications
characteristic of late stages of chronic renal failure. This is uremic lung - interstitial edema and bacterial inflammation of the lung against the background of a decrease in immune defense.
Digestive system
She reacts with decreased appetite, nausea, vomiting, inflammation of the oral mucosa and salivary glands. With uremia, erosive and ulcerative defects of the stomach and intestines appear, fraught with bleeding. Acute hepatitis is a frequent accompaniment of uremia.
Kidney failure during pregnancy
Even a physiologically occurring pregnancy significantly increases the load on the kidneys. In chronic kidney disease, pregnancy aggravates the course of the pathology and can contribute to its rapid progression. This is due to the fact that:
- during pregnancy, increased renal blood flow stimulates overstrain of the renal glomeruli and the death of some of them,
- deterioration of conditions for reabsorption of salts in the renal tubules leads to losses of high volumes of protein, which is toxic to renal tissue,
- increased functioning of the blood coagulation system contributes to the formation of small blood clots in the capillaries of the kidneys,
- worsening arterial hypertension during pregnancy contributes to glomerular necrosis.
The worse the filtration in the kidneys and the higher the creatinine numbers, the more unfavorable the conditions for pregnancy and its gestation. A pregnant woman with chronic renal failure and her fetus face a number of pregnancy complications:
- Arterial hypertension
- Nephrotic syndrome with edema
- Preeclampsia and eclampsia
- Severe anemia
- and fetal hypoxia
- Delays and malformations of the fetus
- and premature birth
- Infectious diseases of the urinary system of a pregnant woman
To resolve the issue of the advisability of pregnancy for each specific patient with chronic renal failure, nephrologists and obstetricians-gynecologists are involved. In this case, it is necessary to assess the risks for the patient and the fetus and correlate them with the risks that the progression of chronic renal failure every year reduces the likelihood of a new pregnancy and its successful resolution.
Treatment methods
The beginning of the fight against chronic renal failure is always the regulation of diet and water-salt balance
- Patients are recommended to eat a diet limiting their protein intake to 60 grams per day and predominantly consuming plant proteins. As chronic renal failure progresses to stage 3-5, protein is limited to 40-30 g per day. At the same time, the proportion of animal proteins is slightly increased, giving preference to beef, eggs and lean fish. The egg-potato diet is popular.
- At the same time, the consumption of foods containing phosphorus (legumes, mushrooms, milk, white bread, nuts, cocoa, rice) is limited.
- Excess potassium requires reducing the consumption of black bread, potatoes, bananas, dates, raisins, parsley, figs).
- Patients have to manage with a drinking regimen of 2-2.5 liters per day (including soup and taking pills) in the presence of severe edema or intractable arterial hypertension.
- It is useful to keep a food diary, which makes it easier to track the protein and microelements in food.
- Sometimes specialized mixtures, enriched with fats and containing a fixed amount of soy proteins and balanced in microelements, are introduced into the diet.
- Along with the diet, patients may be prescribed an amino acid substitute - Ketosteril, which is usually added when GFR is less than 25 ml per minute.
- A low-protein diet is not indicated for exhaustion, infectious complications of chronic renal failure, uncontrolled arterial hypertension, with GFR less than 5 ml per minute, increased protein breakdown, after surgery, severe nephrotic syndrome, terminal uremia with damage to the heart and nervous system, and poor diet tolerance.
- Salt is not limited to patients without severe arterial hypertension and edema. In the presence of these syndromes, salt is limited to 3-5 grams per day.
Enterosorbents
They can somewhat reduce the severity of uremia by binding in the intestines and removing nitrogenous wastes. This works in the early stages of chronic renal failure with relative preservation of glomerular filtration. Polyphepan, Enterodes, Enterosgel, Activated carbon, are used.
Treatment of anemia
To relieve anemia, Erythropoietin is administered, which stimulates the production of red blood cells. Uncontrolled arterial hypertension becomes a limitation to its use. Since iron deficiency may occur during treatment with erythropoietin (especially in menstruating women), therapy is supplemented with oral iron supplements (Sorbifer Durules, Maltofer, etc., see).
Bleeding disorder
Correction of blood clotting disorders is carried out with Clopidogrel. Ticlopedin, Aspirin.
Treatment of arterial hypertension
Drugs for the treatment of arterial hypertension: ACE inhibitors (Ramipril, Enalapril, Lisinopril) and sartans (Valsartan, Candesartan, Losartan, Eprosartan, Telmisartan), as well as Moxonidine, Felodipine, Diltiazem. in combinations with saluretics (Indapamide, Arifon, Furosemide, Bumetanide).
Phosphorus and calcium metabolism disorders
It is stopped with calcium carbonate, which prevents the absorption of phosphorus. Lack of calcium - synthetic vitamin D preparations.
Correction of water and electrolyte disorders
is carried out in the same way as the treatment of acute renal failure. The main thing is to relieve the patient from dehydration due to restrictions in the diet of water and sodium, as well as eliminating blood acidification, which is fraught with severe shortness of breath and weakness. Solutions with bicarbonates and citrates, sodium bicarbonate are introduced. A 5% glucose solution and Trisamine are also used.
Secondary infections in chronic renal failure
This requires the prescription of antibiotics, antiviral or antifungal drugs.
Hemodialysis
With a critical decrease in glomerular filtration, blood purification from substances of nitrogen metabolism is carried out by hemodialysis, when waste products pass into the dialysis solution through a membrane. The most commonly used device is an “artificial kidney”; less commonly, peritoneal dialysis is performed, when the solution is poured into the abdominal cavity, and the peritoneum plays the role of a membrane. Hemodialysis for chronic renal failure is carried out in a chronic mode. For this, patients travel for several hours a day to a specialized center or hospital. In this case, it is important to prepare an arteriovenous shunt in a timely manner, which is prepared at a GFR of 30-15 ml per minute. From the moment the GFR drops to less than 15 ml, dialysis begins in children and patients with diabetes mellitus; when the GFR falls below 10 ml per minute, dialysis is carried out in other patients. In addition, indications for hemodialysis will be:
- Severe intoxication with nitrogenous products: nausea, vomiting, enterocolitis, unstable blood pressure.
- Treatment-resistant edema and electrolyte disturbances. Cerebral edema or pulmonary edema.
- Severe blood acidification.
Contraindications to hemodialysis:
- bleeding disorders
- persistent severe hypotension
- tumors with metastases
- decompensation of cardiovascular diseases
- active infectious inflammation
- mental illness.
Kidney transplant
This is a radical solution to the problem of chronic kidney disease. After this, the patient has to use cytostatics and hormones for life. There are cases of repeated transplants if for some reason the graft is rejected. Renal failure during pregnancy with a transplanted kidney is not an indication for termination of pregnancy. pregnancy can be carried to the required term and is usually resolved by cesarean section at 35-37 weeks.
Thus, Chronic kidney disease, which today has replaced the concept of “chronic renal failure,” allows doctors to see the problem in a more timely manner (often when there are still no external symptoms) and respond by starting therapy. Adequate treatment can prolong or even save the patient’s life, improve his prognosis and quality of life.
Pregnancy is an amazing period in a woman’s life. Her body is changing, new taste preferences and habits are being formed. However, the expectant mother’s body is not always able to bear a baby without medical help. Some serious disturbances in the functioning of the genitourinary system can lead to the fact that the kidneys simply stop functioning. Renal failure during pregnancy is a dangerous pathology that requires immediate intervention from specialists when diagnosed. Therefore, during pregnancy it is very important to closely monitor your health and undergo regular examinations.
How to treat?
If your kidneys hurt during pregnancy, treatment should be carried out after the first symptoms appear. Medicines or folk remedies are suitable for this. You need to be under the supervision of a nephrologist or urologist.
Drug treatment
The use of medications is aimed at reducing pain and eliminating spasms. Therefore, the doctor prescribes safe drugs - No-shpa, Papaverine. If stones have formed in the kidney area, drugs that dissolve them are prescribed to remove them - Cyston, Canephron.
Antibacterial drugs are prescribed only in extreme cases. They are necessary to relieve the inflammatory process and destroy pathogenic microorganisms. The doctor prescribes antibiotics with a reduced dosage to reduce their negative effect on the fetus. Ofloxacin, Amoxicillin, Claforan and other drugs may be prescribed.
To increase the effectiveness of drug therapy, it is necessary to follow a special diet. Salty foods - sausages, canned foods - have a negative effect on the kidneys. They contribute to the stagnation of fluid in the body, leading to the appearance of edema. It is also recommended to exclude protein foods - legumes, meat and fish. It is necessary to give up chocolate, seasonings, parsley, onions, and garlic. Alcoholic drinks are prohibited.
You need to eat often and in small portions. The amount of liquid you drink must be limited to a maximum of 1.5 liters per day. These are soups, water, tea, kefir. The amount of salt consumed must be reduced or eliminated altogether.
Fresh or steamed vegetables without salt are allowed. You can also consume low-fat dairy products, eggs, dried fruits, freshly squeezed juices, honey, teas, and boiled meat.
Traditional methods
Folk remedies can be an excellent addition to traditional therapy. But before using them, you need to consult a nephrologist. Here are the most effective methods:
- Burdock root remedy. It helps very well if the patient has kidney failure. The root should be prepared in the summer or purchased at the pharmacy. Grind the dry raw materials in a mortar to a powdery state. 1 tbsp. pour 200 ml of boiling water over the resulting powder and leave for 10-12 hours. Strain, otherwise the infusion may contain foreign particles, the entry of which into the woman’s body is undesirable. Drink the received amount per day. You also need to maintain a water regime.
- Pomegranate juice. It contains many useful microelements that normalize the functions of the urinary system. It contains potassium, which has a positive effect on the kidneys, improves a woman’s condition and relieves pain. The pectins contained in pomegranate remove harmful substances from the body. You can only drink freshly squeezed juice. It must be taken for 2 months in the morning and evening, 150 ml.
- Corn silk. Infusions, decoctions and extracts are prepared from them. They are used to remove kidney stones. This product has a gentle effect on the body, has no contraindications, and does not have a negative effect on the fetus. To prepare the healing product you need 3 tbsp. corn silk with a liter of boiling water. Boil the product for 30 minutes, leave for 30 minutes and strain. Drink 50 ml 4 times a day. This drink must be prepared daily, as it spoils quickly. Store in the refrigerator for no more than 2 days.
The above remedies can also be used for not very advanced diseases as an independent remedy, so as not to burden the body with medications.
Types of kidney failure
There are acute and chronic forms of the disease. In case of a chronic course, it is very important, even at the planning stage, to contact specialists who, based on the results of tests and studies, will be able to assess the chances of a successful pregnancy and childbirth. Unfortunately, medicine is also aware of cases where, due to serious complications, doctors were forced to terminate a pregnancy at an early stage in order to save the woman’s life. In later stages, emergency delivery is carried out in situations associated with the risk of bleeding in the mother and intrauterine fetal death, as well as in the presence of other abnormalities requiring surgical intervention.
Since the kidney is a kind of filter for the human body, additional load on this organ can lead to the appearance and development of diseases such as:
- Pyelonephritis (kidney inflammation);
- glomerulonephritis (damage to the glomeruli);
- formation of stones and the presence of sand in the kidneys and ureter;
- cystitis (bladder infection).
All of the above painful conditions can provoke acute renal failure in pregnant women. The development of this type of disease is most often diagnosed in the first and last trimester. Depending on the symptoms, prerenal, renal and postrenal forms are determined.
Urostasis of the kidney: what is it, symptoms of stagnation of urine in the kidneys and bladder - About the Kidneys
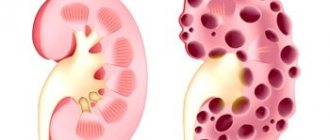
Hydronephrosis is stagnation of urine in the kidneys, enlargement of the renal system and its calyces. According to statistics, the disease affects women more often than men. The development of hydronephrosis in men most often ends with prostate cancer, urethral stricture, and in young people the disease is caused by urolithiasis.
Congestion in the kidneys is characterized by the accumulation of fluid in the renal cups, as a result of which the functionality of the renal system is disrupted and a pyelocaliceal pathology is formed. Hydronephrosis can be infected or aseptic.
In this article we will tell you why urine stagnation occurs in the kidneys, we will analyze the symptoms, diagnosis and treatment of the pathology.
Reasons for the formation of stagnant urine
Hydronephrosis is stagnation of urine in the kidneys, enlargement of the renal system and its calyxes
Impaired functioning of the renal system and the formation of stagnation of urine can occur due to the following reasons:
- the presence of pathological processes in the urethra and bladder; such a disorder can be provoked by tumor processes, previous infectious diseases, phimosis;
- external compression of the ureter, which is formed due to a violation of the lymphatic system, cysts, after surgery;
- changes in the lumen of the ureter caused by urolithiasis, torsion or kinking of the ureter caused by injury or congenital disorder;
- congenital anomaly or the presence of VUR, which can impair the functioning of the renal system and pelvis.
For information! There are congenital hydronephrosis, which forms in fetal development, and acquired hydronephrosis, which occurs as a result of damage to a previously healthy kidney.
Stagnation of urine in the kidneys during pregnancy is considered a fairly common phenomenon. The disorder occurs due to changes in hormonal levels, which affect the rhythmic contractions of the ureter.
The last trimester is dangerous because due to the increase in the size of the uterus, mechanical compression of the ureter occurs.
To monitor the situation and the health of a pregnant woman, a urine test is taken on a regular basis for culture, and if obvious deviations from the norm are confirmed, therapy is carried out.
Symptoms of hydronephrosis
With chronic stagnation of urine in the kidneys, the patient feels attacks of severe pain in the lumbar region
At the initial stage of hydronephrosis, a person does not feel any symptoms or changes in his health. There may be a feeling of general malaise, tiredness or increased fatigue. It is precisely because of the absence of symptoms that it is quite difficult to identify the problem, however, it is possible with a random examination. The main symptoms of congestion include:
- the organ increases in size and weight;
- the organ acquires a blue-red color;
- the appearance of yellow spots;
- tense state of the renal capsule;
- pronounced venous pattern;
- connective tissue shrinks as a result of which the organ acquires an uneven surface;
- with enlargement of the glomeruli, red spots are observed;
- during a period of prolonged stagnation, atrophy of the renal substance occurs and its replacement with connective tissue;
- the kidney substance changes to fat.
With chronic stagnation of urine in the kidneys, the patient experiences the following symptoms:
- attacks of severe pain in the lumbar region;
- intense pain attacks radiating to the genitals appear after eating food;
- irregular attacks of nausea and vomiting;
- temperature rise to 39C degrees;
- presence of blood clots in urine.
For information! In urological practice there is such a thing as a congestive kidney. This condition is accompanied by poor circulation, resulting in heart failure.
Most often, the chronic form passes without permanent symptoms; attacks are increasing and intermittent. If you feel discomfort and notice changes, contact a specialist for advice.
Diagnosis of the disease
The purpose of diagnostic measures is determined based on the patient’s complaints
The purpose of diagnostic measures is determined based on the patient’s complaints and includes:
- general urine analysis;
- biochemical and general blood test;
- ultrasound examination of the bladder and renal system;
- examination of the urinary system using magnetic resonance imaging;
- intravenous urography;
- CT scan;
- retrograde pyelogram;
- radionuclide research.
For information! Diagnostics allows you to determine the pathological disorder of the internal structure of the organ, and also reflects the general condition of the vessels and ureter.
Microscopic examination reveals how dilated the vessels are, as well as the presence of protein in the collapsed capillaries and tubules.
Treatment of hydronephrosis
To reduce and prevent pain, the patient is prescribed painkillers and antibacterial medications.
Long-term morphology of the disease significantly impairs the functionality of the renal system and causes renal failure. Stagnation of urine in the kidneys causes the following complications:
- pyelonephritis of all forms;
- stone formation;
- progression of inflammatory processes throughout the body, which can result in death;
- secondary reduction in kidney size;
- a sharp increase in blood pressure.
If the disease is confirmed, treatment should be started immediately. To reduce and prevent pain, the patient is prescribed painkillers and antibacterial medications. Normalization and restoration of urine outflow is carried out using surgical intervention. The choice of surgery depends entirely on the cause of congestion in the kidneys.
Catheterization
This operation is performed in the presence of a malignant or benign tumor in the prostate gland, as well as in the presence of sclerosis of the bladder neck
This operation is performed in the presence of a malignant or benign tumor in the prostate gland, as well as in the presence of sclerosis of the bladder neck. The site of narrowing of the ureter is widened using a ureteral stent and an endoscope is inserted to perform retrograde pyelography.
Percutaneous nephrostomy
Using ultrasound, an external drainage is installed into the cavity system of the organ; the drainage helps urine flow into the external collection system.
Carrying out open surgery
Open surgery is performed if there are indications:
- the presence of a tumor in the retroperitoneal region;
- the presence of stones that cannot be eliminated endoscopically or with shock wave therapy;
- presence of retroperitoneal fibrosis;
- with pathological dilatation of a blood vessel.
Endoscopic method
Used in the presence of stones that prevent normal urine flow. Any surgical intervention can partially or completely remove the cause of the formation of compression of the kidney, however, the result of the operation completely depends on the stage and form of the disease.
Disease prevention
Timely and high-quality implementation of preventive measures to eliminate the causes of hydronephrosis contributes to the complete and rapid restoration of the functioning of the renal system.
With a long-term and bilateral course of the pathology, the prognosis of the pathology ends with the appointment of hemodialysis or a kidney transplant.
The main preventive measures for the formation of stagnation in the kidneys include:
- daily observance of personal hygiene rules;
- maintaining a healthy lifestyle;
- prevention of pathologies of the genitourinary system;
- timely treatment and prevention of infectious diseases, including sexually transmitted diseases;
- following a diet with a reduced amount of table salt, as well as a complete abstinence from alcoholic beverages.
Remember, the development of the disease and its complications can be prevented only by strictly following all recommendations, timely examination and treatment.
Source:
Kidney urostasis - what it is, symptoms, diagnosis and treatment
A person suffering from kidney urostasis has difficulty passing urine. With this disease, quite unpleasant consequences can occur. That is why, with its acute development, you should immediately seek help from a specialist.
Urostasis (from the Greek “urinary cessation”) is a pathology in which urinary stagnation . Complications begin during its outflow, and sometimes there is a complete absence of its release. This disease can be triggered by various factors and develop in either one or two kidneys.
Classification of urostasis
The disease is divided into two groups, taking into account the complexity of its course:
- Chronic urostasis.
- Acute urostasis.
- Pain in the lumbar region.
- Itching, burning and pain when urinating.
- Swelling of the face and legs.
In the first case, the disease actively develops over many months or years. During the course of the disease, favorable conditions appear for the emergence of any infectious or atrophic processes.
The acute form is characterized by a high rate of development and requires immediate attention to the clinic.
Symptoms
The most noticeable sign, at the very beginning of the disease, is a decrease in the amount of fluid secreted . Patients begin to notice a partial or complete absence of urine. After this, other symptoms appear, namely:
Diagnostics
Examination of the patient allows the doctor to determine the type and form of the resulting pathology. To complete the clinical picture, it is necessary to use the following additional diagnostic methods:
Treatment
With mechanical urostasis, surgical intervention is often resorted to. Thus, if congenital anomalies are detected, adhesions are dissected and areas of stenosis of the renal tubules and ureters are expanded.
During pregnancy, ureteral stenting before labor begins.
Also, in this case, they may recommend performing special physical exercises that have a beneficial effect on the rehabilitation of the excretory function.
For urolithiasis, laser equipment is used to crush stones or get rid of them through surgery.
Neoplasms are eliminated or radiation and chemotherapy .
Regarding the dynamic causes of urostasis, in such cases, a conservative method of treatment . For example, they are involved in correcting the functioning of the central nervous system.
Consequences
To avoid undesirable consequences of urostasis, do not hesitate to visit a doctor and promptly get rid of all the causes that can provoke it.
Refusal of a specialist’s instructions entails such consequences as: kidney deformation, reflux nephropathy, pyelonephritis, glomerulonephritis, arterial hypertension and cystitis. However, the most unpleasant thing, in addition to the above, is kidney failure .
Only strict adherence to the specialist’s instructions makes it possible to protect yourself from the negative consequences of urostasis.
Source: https://uroscope.ru/diagnostika/urostaz-pochki-chto-eto-takoe-simptomy-zastoya-mochi-v-pochkah-i-mochevom-puzyre.html
Signs of the disease
In addition to pain in the area where the kidneys are located, against the background of a general deterioration in well-being, swelling of the lower extremities, drowsiness, and fatigue are also possible. Complaints of severe headache and high blood pressure, difficult and painful urination, dry mouth, nausea and repeated vomiting, in turn, are a reason to immediately contact the antenatal clinic or the nearest clinic. If a patient with a history of any diseases, one way or another related to the kidneys, is not promptly provided with all the necessary assistance for such symptoms, then the probability of death is almost 100%. Failure of one or both kidneys simultaneously leads to severe intoxication of the body. The state of pregnancy against the background of the general clinical picture only aggravates the situation.
Treatment methods
After the disease is diagnosed, the doctor will prescribe complex therapy. Since not all medications intended to relieve pain and eliminate the causes of their occurrence can be used while waiting for a baby, urologists are very careful when prescribing many medications. The main methods of treatment in this case are:
- Nutrition adjustments. In case of kidney failure, patients are advised to drink at least 2 liters of water daily and eat foods that are easily absorbed by the body. It is advisable to exclude white bread products and products rich in potassium from the diet.
- Medication support. To prevent the consequences of intoxication, drugs are used that remove toxins from the body. "Canephron" and "Brusniver" have an anti-inflammatory effect and do not have any negative effect on the fetus. However, this does not mean that you can take them on your own!
It is strictly prohibited to use any medicines on your own initiative!
Unfortunately, the chronic form of the disease cannot be cured. To relieve symptoms and stabilize the general condition of the body, the doctor may prescribe systematic dialysis. In addition, the patient is strictly prohibited from any type of physical activity and bed rest is indicated in case of exacerbation.
Diagnostics
Symptoms of the development of the pathological process are not enough to make a diagnosis, so a number of diagnostic procedures are performed:
- General urine analysis with quantitative determination of protein and microscopic examination of urine sediment.
- Detailed analysis of capillary blood + ESR.
- Biochemical blood test. Required: glucose, protein, urea, uric acid and creatinine. It would be useful to determine CRP and procalcitonin, as well as the acid-base composition of the blood.
- Bacteriological examination of urine.
- Study of venous blood coagulation factors.
Laboratory research allows you to determine the type and type of pathological process. But for the final diagnosis, emergency ultrasound and magnetic resonance imaging are performed.
Kidney failure is detected and treated by urologists or nephrologists. Specialists choose the tactics and treatment regimen.
There are no drugs for PN. Treatment involves the complex use of medications approved during gestation.
Drug therapy:
- Anti-inflammatory drugs (Canephron).
- Drugs that prevent intoxication (for example, a group of sorbent drugs).
- Antibiotic therapy (Amoxiclav, but if the bacteria are sensitive to this type of antibiotic).
- Taking antiviral drugs (feron-containing drugs).
- Anabolics.
- Antifungal drugs if necessary.
Surgical intervention is possible, and in a critical situation, transfusion of blood, plasma and formed elements.
The chronic form of PN during pregnancy (and in principle) cannot be cured. For normal prolongation of pregnancy, an individual treatment regimen for the patient is selected.
Diet for kidney failure is part of a comprehensive treatment.
- Drink plenty of fluids (at least 2.5 liters per day, excluding liquid foods).
- Restriction: milk, mushrooms, nuts, cocoa, white bread.
- Limited intake of “animal” protein.
- Foods high in potassium (bananas, dates, raisins).
Allowed:
- lean boiled fish;
- milk soups;
- berries and fruits;
- lean meat (steamed or boiled);
- raw vegetables (not all).
Cooking meals for acute renal failure and chronic renal failure should be accompanied by a complete abstinence from salt.
Complications of kidney failure
Delayed diagnosis can lead to the acute form of the disease progressing to an incurable (chronic) stage. In addition to such disappointing prognoses, there is a risk of developing uremic coma and sepsis.
Even if a woman has no apparent reason to worry, planning a pregnancy is an ideal scenario. With this approach, you can avoid many serious health problems even before conception, because the expectant mother is responsible not only for herself, but also for the little representative of the new generation.
Kidney problems are one of the most common pathologies among expectant mothers. Due to the increased stress on the body during pregnancy, doctors regularly monitor how the kidneys are working. Violations can appear for various reasons.
Why do kidneys fail in pregnant women?
Most often, pregnant women's kidneys fail midterm or in the last weeks of pregnancy. The increased work of the maternal body and the active release of progesterone leads to an increase in the volume of blood pumped through the kidneys. As a result, the calyces and pelvis noticeably expand. Against the background of such changes, the risk of infection of the urinary system increases.
Inflamed kidneys in pregnant women are the cause of general malaise
The impetus for kidney failure can be:
- An infection enters the bladder, under the influence of which the kidneys work harder. The inflammatory process often leads to kidney failure.
- Active growth of the uterus, which compresses the internal organs. As a result, the outflow of urine is disrupted, creating favorable conditions for the development of a bacterial infection.
- The presence of inflammatory processes in the oral cavity and nasopharynx. Tonsillitis, frequent colds and caries have a negative impact on kidney function.
- Noticeable weakening of the immune system.
If even before pregnancy problems with the kidneys made themselves felt, when carrying a child you need to be especially vigilant about your condition. Any warning signs deserve attention.
Stagnation of urine (hydronephrosis)
Stagnation of urine, or hydronephrosis, is a rather unpleasant and dangerous condition that occurs when the natural outflow of fluid from the kidneys is disrupted.
This paired organ of the human body has a rather complex structure and performs the function of removing toxins in the urine.
Fluid accumulates in the renal calyces, located under a fibrous capsule formed from connective tissue.
Then it enters the renal pelvis, then into the bladder and is naturally excreted from the body. Hydronephrosis and improper, disturbed urine discharge disrupt the natural function of the kidneys, causing pathology of the expansion of the collecting system, and there are 2 types: aseptic and infected.
The first stage of this disease occurs with virtually no visible symptoms. In the case of an aseptic type, changes in the structure of the cups and pelvis, disruption of their functionality directly depend on the time and degree of compression; in another situation, infection joins these processes and inflammation develops.
Most often, stagnation of urine in the kidneys occurs in women: during pregnancy or the development of oncology in the gynecological organs. In men, this pathology develops at a much older age and is most often associated with the formation of kidney stones, urethral stricture or various diseases of the prostate gland.
Reasons for the development of fluid stagnation in the kidneys
The causes of the development of an unpleasant and quite dangerous phenomenon - stagnation of urine - are pathologies and dysfunctions of the bladder and ureter - tumor neoplasms, phimosis or complications from previous infections.
In the presence of any tumor formations in the abdominal cavity located near the kidneys, with enlarged lymph nodes or pathological changes in the peritoneal tissues, compression of the ureters occurs, which also leads to fluid stagnation.
Disturbances in the ureter that develop with urolithiasis, its torsion or kinking due to congenital pathologies or injury, blockage of the ureter by a formed calculus lead to stagnation of urine. When vesicoureteral reflux is disturbed, urine is released back into the pelvis, which causes pathological disruption of the kidney.
Symptomatic manifestations
Stagnation of urine in the bladder for a long time develops practically asymptomatically; only in the presence of infection or the occurrence of urolithiasis may signs of hydronephrosis appear. They are as follows:
Hydronephrosis of the kidneys
- Renal stasis - often accompanied by renal colic, which manifests itself as sharp pain in the lower back, at the location of the kidneys and along the ureter. It radiates to the perineum and the entire surface of the thigh.
- The contraction of the renal pelvis, overgrown with connective tissue, is disrupted, which causes dull and aching pain in the lumbar region. Such sensations are not constant, they arise and intensify during physical activity.
- During the pain syndrome, urination disturbances are observed and hematuria occurs - the appearance of bloody discharge in the fluid and its turbidity.
- An infectious process developing in the kidneys is often accompanied by a sharp increase in body temperature, a deterioration in the general condition, a decrease in the usual performance and increased fatigue of the patient. Sometimes there is an increase in blood pressure.
Violation of urine outflow has acute and chronic forms.
In the first case, the patient’s rather severe pain in the lower back turns into discomfort throughout the entire abdominal cavity, especially after eating. They also affect the genital area. The patient may observe cloudy urine and the presence of blood in it. Such symptoms are accompanied by nausea and vomiting. The chronic form of the disease is practically asymptomatic, but in some cases a gradual increase in manifestations may be observed.
Separately, it should be said about stagnation of urine in pregnant women. When carrying a child, a woman's hormonal background changes greatly, which leads to malfunctions of many internal organs. Disturbances in hormonal levels lead to dysfunction of ureteral contraction, which contributes to urinary stagnation. In the last trimester of pregnancy, the enlarged uterus puts pressure on the ureter, blocking its lumen.
During pregnancy, stagnation of urine most often occurs in the right kidney, since the anatomical location of a woman’s internal organs changes during pregnancy.
The risk of kidney prolapse on the right side increases.
Since these pathologies usually occur in the seventh or eighth month of pregnancy and after childbirth, the functioning of all internal organs is normalized naturally; no special treatment is required.
The only complication that can arise with this condition is pyelonephritis; with regular laboratory monitoring of culture and urine and blood tests, it can be treated quite easily with drug therapy.
Diagnostic measures
Prolonged course of the disease without timely treatment leads to deterioration and disruption of the natural functions of the kidneys and increases the risk of developing acute renal failure.
Stagnation of urine causes a disease such as pyelonephritis, increases and accelerates the formation of stones - stones in the kidneys and ureter, reduces the size and normal functioning of the kidneys, leads to increased blood pressure and contributes to the spread of the inflammatory process in the body, which causes death.
Therefore, if any pain in the lumbar region occurs, you should immediately consult a doctor who, based on the patient’s complaints, will conduct laboratory tests. These will include:
- general and biochemical urine and blood tests;
- Ultrasound of the genitourinary system;
- MRI, intravenous urography, CT, retrograde pyelogram and radionuclide studies of the pelvic organs and genitourinary system.
The results of these studies will help to study pathological disorders of the internal structure of the kidneys and identify the condition of the ureter and blood vessels.
During pregnancy, many examination methods cannot be performed, so the expectant mother is diagnosed based on her complaints, laboratory tests of blood and urine, as well as the results of an ultrasound of the bladder and abdominal organs.
After the studies have been carried out, it is quite important not to delay treatment, since this disease leads to the development of serious complications.
Therapy for hydronephrosis is based on treating the cause that causes congestion and disrupts the natural outflow of urine.
In the acute stage, to reduce pain and prevent the occurrence and development of infection, the patient is prescribed antibacterial and painkillers.
To restore the performance and functionality of the affected kidneys, special medications are prescribed that restore their microcirculation. To normalize the natural outflow of urine, surgical or instrumental intervention is necessary, the chosen methods of which directly depend on the cause and degree of stagnation.
The purpose of this operation is to strive to preserve and restore the functionality of the organ as much as possible. Sometimes such intervention must be quite urgent, in other cases, for some reason, it becomes impossible. The surgical operation includes:
- Bladder catheterization. It is often carried out with the development of neoplasms of any nature in the prostate gland or cervical sclerosis and consists of expanding the ureter at the site of its narrowing using a special stent.
- Percutaneous nephrectomy. It is carried out if it is impossible to install a stent and consists of introducing a drainage system into the kidney.
- Open surgery. It is performed for fibrosis in the peritoneum, fairly large stones in the ureter, aortic aneurysm, or the presence of tumors in the peritoneal cavity.
- Endoscopic intervention. It is used to remove small stones that interfere with the natural passage of urine and is most often used during pregnancy.
The main preventive measures for the occurrence of such a condition as urinary stagnation are:
- prevention and timely treatment of viral and bacterial infections of the whole body, as well as sexually transmitted diseases;
- prevention of diseases of the genitourinary system of the body;
- prevention of the development of urolithiasis;
- compliance with hygiene rules;
- healthy and active lifestyle.
A good way to both treat and prevent stagnation of fluid in the urinary tract is a proper diet with a low salt content in the food consumed and avoidance of alcohol and smoking.
Source: https://sochi-mebel.ru/bolezni/zastoy-mochi-gidronefroz
How do kidney problems manifest themselves in pregnant women?
An expectant mother may suspect kidney failure based on the following symptoms:
- feeling of extreme weakness;
- worsening night sleep;
- the appearance of severe headache;
- feeling of constant dry mouth and thirst;
- the appearance of pain in the lumbar region;
- swelling of the legs and arms;
- the appearance of shortness of breath even with slight exertion.
If at least one of these signs is present, you should immediately go to see a doctor. The specialist will prescribe the necessary tests to confirm or exclude the diagnosis. Failure kidneys can only be treated in a hospital setting. The consequences of the disorder are increased blood pressure, fluid retention in the body, malnutrition of the fetus, and even miscarriage or premature birth. If such a pathology appears in the third trimester, an emergency caesarean section is usually performed.
• Diseases of the genitourinary tract in women • Pregnancy with chronic renal failure
Typically, pregnancy with chronic renal failure is difficult, although advances in prenatal care have made the prognosis more favorable than before. This primarily applies to women whose kidney pathology is moderate. Today, nine out of 10 pregnant women with chronic renal failure have a chance to safely carry and give birth to a healthy child. With severe insufficiency, the chances of carrying the pregnancy to term and successful childbirth are less. The situation is even more unfavorable for patients who, along with renal failure, have severe hypertension. In such a situation, the risk of miscarriage, stillbirth, intrauterine fetal death, premature birth (often artificially induced to save the life of the mother and child), premature placental abruption, and congenital disorders in the development of the fetus is much higher.
Impaired renal function usually progresses during pregnancy in women suffering from glomerulonephritis, as well as moderate or severe renal failure. Experts are still not clear whether this is caused by pregnancy itself or associated hypertension.
Kidney function worsens whether the pregnancy is terminated or not. In chronic renal failure, obstetricians often suggest the first option due to the risk to the lives of mother and child. Such a decision (made by the woman herself) should first of all be based on an assessment of the pregnant woman’s condition and the potential consequences for her health and life. The problem is that the choice has to be made on the basis of far from complete information, since even today doctors do not have a consensus about the danger of complications during pregnancy in patients with moderate or severe renal failure. It is only known that pregnancy is not associated with major troubles with mild renal failure.
S. Aizenshtat
“Pregnancy in chronic renal failure”
- article from the section
We have not encountered pregnant women with a decompensated stage of chronic renal failure, since conception does not occur in such patients. The preclinical (latent) stage of renal failure is not so rarely diagnosed in patients with chronic pyelonephritis and chronic glomerulonephritis, with abnormalities of kidney development. Pregnancy at this stage of renal failure usually proceeds as with risk degree II (see sections “Glomerulonephritis”, “Pyelonephritis”). At the compensated stage of chronic renal failure, complications of pregnancy and childbirth for women and the fetus are frequent and severe (III degree of risk), therefore pregnancy at this stage of chronic renal failure is contraindicated. In addition, as already indicated, in such patients after childbirth, chronic renal failure progresses or develops acute renal failure. S. How et al. concluded that pregnancy in women with moderate renal impairment may worsen renal function, but fetal survival is higher than previously reported.
Symptoms of the disease
Chronic renal failure during pregnancy - symptoms
- latent phase (hidden): fatigue, weakness, dry mouth. Minor abnormalities in urine analysis;
- compensated phase: increased diuresis to 2.5 l, severe apathy and weakness;
- intermittent phase: a persistent change in nitrogen metabolism in the biochemical analysis of venous blood. Nausea, vomiting, tremors, increased thirst and unpleasant taste in the mouth. The skin turns yellow and a specific urinary odor appears.
- terminal phase: complete absence of urine, puffiness of the face, skin acquires a gray-yellow tint, defecation is disrupted. Fatal disorders of the internal secretion organs, nervous system disorders, encephalopathy, irreversible changes in the coagulation system.
Acute renal failure during pregnancy - symptoms
- nagging pain in the lower back;
- cessation of urine output;
- adynamia;
- lethargy;
- proteinuria;
- azotemia;
- body hyperthermia;
- muscle weakness;
- change in the color of urine (when it is excreted);
- ari smell from a pregnant woman;
- change in skin color.
A pregnant woman can determine the initial symptoms herself and immediately contact a gynecologist.
6.4. Treatment of chronic kidney disease in pregnant women
Treatment of patients with signs of chronic renal failure if they refuse an abortion or termination of pregnancy at a later date consists of creating a regimen, prescribing a diet and conducting drug therapy.
Pregnant women with chronic renal failure need to limit physical activity and should mainly stay in the hospital; they should be prescribed a diet that meets certain requirements: protein restriction along with the introduction of sufficient amino acids; high calorie content due to the additional introduction of fats and carbohydrates; consumption of a significant amount of vegetables and fruits, taking into account the characteristics of water and electrolyte disorders. The main feature of the diet is protein restriction. Outside of pregnancy, this recommendation is to constantly consume 50-60 and even 35 g of protein per day. A woman who remains pregnant, in the interests of the child, cannot be on such a diet and should receive up to 80-100 g of protein per day, not only from plant proteins (potatoes, legumes), but also from animals (meat, cottage cheese). Deliberate violation of the most important principle of diet does not contribute to the elimination of azotemia, and this, in particular, worsens the prognosis of kidney disease after childbirth.
Fats and carbohydrates are not limited. Due to lipid metabolism disorders characteristic of chronic renal failure, leading to early atherosclerosis with a high risk of developing coronary heart disease and cerebrovascular pathology, it is useful to enrich a low-protein diet with polyunsaturated fatty acids (vegetable oil, seafood, fish oil). Calorie content should not be lower than 2100-2200 kcal/day, which is achieved by increasing the content of carbohydrates and fats. Patients can consume vegetables and fruits, juices, bread, and cereals depending on their appetite. Patients should receive no more than 5 g of salt. If there is a tendency to acidosis and hypernatremia (in the absence of hyperkalemia), it is advisable to increase the amount of potassium-containing foods (apricots, walnuts, fruit juices) in the diet. If the excretory function of the kidneys is preserved, it is useful to increase the amount of fluid consumed to 2 liters through compotes, juices, and mineral waters.
Drug treatment should be carried out under mandatory monitoring of blood electrolytes. To alkalize the plasma and compensate for sodium losses, a 5% sodium bicarbonate solution (300-500 ml), a 5-20% glucose solution (300-500 ml) should be administered; for persistent vomiting - 3% sodium chloride solution (200-300 ml) or isotonic sodium chloride solution. For hypocalcemia, use a 10% solution of calcium gluconate (50 ml/day intramuscularly). The administration of glucose and insulin is indicated for hyperkalemia and severe liver dysfunction.
Lespenefril 10 ml 2 times a day intravenously or 10 ml 3 times a day orally, neocompensan (100 ml intravenously), hemodez (400 ml intravenously) can be used. Anabolic hormones are contraindicated for pregnant women. To stimulate diuresis, a 10-20% solution of glucose with insulin and 500 ml of mannitol are administered intravenously or furosemide.
Washing the stomach and intestines with a 2% sodium bicarbonate solution is performed in case of nausea and vomiting in order to remove nitrogenous waste from the digestive tract. This procedure is performed on an empty stomach, it can be repeated 2-4 times before meals. Microenemas with a weak solution of sodium bicarbonate and a hypertonic solution of sodium chloride help quite well.
In addition to the indicated drug therapy, treatment of arterial hypertension is continued. There is no need to strive to reduce blood pressure to normal levels, since in this case renal blood flow decreases and kidney activity deteriorates. It is enough to maintain the pressure at 150/100 mm Hg. This pressure slightly impairs kidney function, but can affect the uteroplacental circulation and fetal development.
The desire to improve uteroplacental blood flow by normalizing blood pressure can lead to the progression of uremia. For the treatment of arterial hypertension in patients with chronic renal failure, the most suitable drugs are dopegit and clonidine, which combine well with saluretics. Due to its slow elimination, the dose of dopegyt should be reduced by 1.5-2 times. Peripheral arteriolodilators (minoxidil, hydralazine), combined with saluretics and small doses of beta-blockers, are characterized by a stronger hypotensive effect and a beneficial effect on renal blood flow. Calcium antagonists, which do not cause sodium and water retention or a decrease in renal blood flow, do not activate the renin-angiotensin-aldosterone system and therefore can be used for chronic renal failure. The administration of magnesium sulfate is contraindicated to avoid an increase in hypermagnesemia characteristic of chronic renal failure.
Cardiac glycosides are prescribed with caution, reduced to 50-70% of the therapeutic dose, since the time it takes for them to be eliminated from the body
slow, and they can cause glycoside intoxication. In case of severe hypokalemia, cardiac glycosides are contraindicated.
To combat anemia, iron and cobalt supplements are used (preferably parenterally). If there is a sharp decrease in hemoglobin content, transfusions of red blood cells or freshly citrated blood are indicated. You should not strive to increase the hemoglobin content exceeding 90 g/l. Frequent blood transfusions contribute to the suppression of hematopoiesis, so they should be done once a week while using calcium supplements and desensitizing agents (diprazine, suprastin, etc.).
Among the hemostatic agents for major bleeding, in addition to calcium and vitamin K preparations, a fibrinolysis inhibitor is used -
ε-aminocaproic acid (300 ml of 10% solution intravenously or 2 g orally 4-6 times a day).
Anticoagulants are contraindicated even in the initial stages of chronic renal failure.
Antibacterial drugs can be used in normal or reduced doses. Penicillin, oxacillin, erythromycin are used in full dose; ampicillin - half; kanamycin, monomycin, colimycin, polymyxin are contraindicated due to their nephrotoxicity. Gentamicin and cephalosporins are used only in extreme cases, reducing the dose by 50-70% of the usual one. If there is a threat of hyperkalemia, in particular with oligoanuria, crystalline penicillin should not be administered due to its high potassium content.
Conservative therapy is effective for moderately severe renal failure. In more severe cases, hemodialysis treatment must be used. Hemodialysis for chronic renal failure is indicated in the terminal stage, when threatening hyperkalemia (more than 7 mmol/l), acidosis (pH less than 7.28) develops, nitrogenous wastes in the blood are very high (urea - 50 mmol/l, creatinine - 1400 µmol/ l). In pregnant women, chronic renal failure is not so severe, so hemodialysis is used only for acute renal failure. The enterosorption method is also not used in pregnant women with chronic renal failure.
Women with early stages of chronic renal failure should be protected from pregnancy by using intrauterine contraceptives. Intrauterine contraceptives in women with chronic glomerulonephritis and chronic pyelonephritis do not cause exacerbation of the disease, infectious processes in the genitals and hemorrhagic complications.
Treatment
Treatment of acute renal failure consists of immediate hospitalization in the intensive care unit and the use of emergency medications. The goal of therapy will be to cleanse the body of toxins and restore kidney function. For this use:
- hemodialysis - blood purification using an “artificial kidney” device;
- hemosorption - carrying blood through a “column” with an absorbent, often activated carbon;
- plasmapheresis - blood sampling, followed by purification and re-infusion to the patient.
To restore the balance (water-salt, electrolyte), potassium, calcium, and sodium preparations are used. If there is a primary or secondary inflammatory process in the kidneys, antibiotics (Amoxiclav) are prescribed. When treating acute renal failure, only very mild diuretics, Diacarb, Gyrothiazide, are used.
How to treat kidney failure in people if it has become chronic? Therapy of chronic renal failure requires a long period of time and includes a large number of techniques and drugs used.
Self-medication in the presence of signs of chronic renal failure is strictly prohibited! Incorrectly chosen tactics can aggravate the patient’s condition and cause irreparable harm to health!
Medicines
The prescription of drugs depends on the patient’s condition and test results.
Antibiotics are prescribed only according to indications and strictly at the discretion of the treating specialist. Penicillin drugs and cephalosporins are suitable. However, the dosage and course are adjusted, since these indicators should be less than when treating an ordinary patient. Recommend: Cefalotin, Cefuroxime, Cefixime and others. Gentamicin is not recommended due to nephrotoxicity.
Sorbents help remove “slags” and decay products from the body, that is, they slightly compensate for the functioning of the kidneys. Recommend: Filtrum-STI, Enterodes, Enterosgel.
Plasma replacement agents help restore blood flow, reduce intoxication, lower blood pressure, and have a diuretic effect. Recommend: Reogluman, Sorbilact.
Diuretics or diuretics help remove fluid accumulated in tissues, eliminate edema, and lower blood pressure. Recommend: Furosemide, Lasix, Trigrim.
Antihypertensive drugs for chronic renal failure should be prescribed with caution. There is ongoing debate among experts regarding the use of these drugs. One group of doctors considers lowering blood pressure with antihypertensive drugs not advisable. Another group advocates this group of drugs.
Conclusion, it is necessary to lower blood pressure gradually, and this requires the qualified opinion of the attending physician and an individual approach to each patient. The following drugs can be prescribed: Corinfar, Lomir, Lorista, Aprovel, Carvedilol.
Patients in the terminal phase are referred for hemodialysis twice a week. The blood is purified from accumulated decay products and “toxins” using an “artificial kidney” apparatus. The procedure does not require hospitalization; once the procedures are completed, you can leave the hospital. The disadvantage is regular and long-term (lifelong) visits to hemodialysis.
An alternative option is transplantation surgery, in which a donor kidney can be transplanted.
Diet therapy
The basis of therapy for chronic renal failure will be the correct therapeutic diet. In patients with impaired renal function, there is an urgent need to prescribe treatment table No. 7, No. 7a, No. 7b. The treating specialist prescribes nutrition based on the condition of the affected organ and the duration of the pathological process.
Therapeutic nutrition allows you to minimize the load on the kidneys, thereby facilitating the restoration of their function.
Limit or completely eliminate:
- Smoked, salted and pickled products.
- Sausages, canned food, cheese, salted cottage cheese.
- Semi-finished products, fast food.
- Legumes, onions, garlic, spinach, sorrel, radishes, radishes.
- Fatty meats, fish high in fat.
- Sweet carbonated drinks.
- Black tea and coffee.
- Energy.
- Alcohol.
- Chocolate, confectionery.
You need to include in your diet:
- Green tea, compotes, clean drinking water, herbal teas.
- Vegetables (except forbidden ones), fruits and berries (avoid sour ones).
- Butter, sour cream, yogurt.
- Boiled lean meat, boiled eggs, fish.
- Crackers, bread, preserves, jams, honey.
- Dried fruits.
Cooking: boiling, steaming, stewing, baking. The calculation of the required protein, liquid and salt occurs individually, in each specific case. Food is prepared without salt, and the patient receives the required amount, an average of 3 grams, in his or her hands.
In case of a pronounced pathological process, salt is completely excluded, and the norm of protein products is sharply reduced. The presence of chronic renal failure obliges the patient to follow a therapeutic diet throughout his life.
During the period of early detection of the pathological process, all therapeutic measures are aimed at eliminating the underlying disease that provokes chronic renal failure. For example, in the presence of hypertension, medications that eliminate high blood pressure. If the ureters are blocked, procedures are used to restore the normal flow of urine (for example, removal of a stone or tumor).
Folk
In case of renal failure, treatment with folk remedies can be carried out only after consultation with a doctor. Traditional methods can significantly improve the patient’s condition, get rid of high blood pressure and edema, and increase urine output.
How to use herbs in treating kidney failure:
Recipe No. 1. Mix 50 grams of birch buds, oak and birch bark. Brew 3 tablespoons of the mixture in a liter teapot. Wrap and leave for 60 minutes. Strain. Divide the resulting infusion into 6 doses.
Recipe No. 2. Pour a tablespoon of lingonberry leaves into a glass of boiling water. Insist. Drink instead of tea.
Recipe No. 3. Make a mixture of mint leaves, lemon balm and calendula flowers, chop. Place 4 tablespoons of the resulting mixture in an enamel container and pour half a liter of cold water. Simmer over low heat for 5 minutes. Pour the resulting decoction (along with the leaves) into a thermos or earthenware teapot. Leave for at least 6 hours. Take 0.5 cups, 1 time per day.
Recipe No. 4. Prepare 100 grams of sea buckthorn and rose hips. Wash the rose hips and put them in a thermos, add the ground sea buckthorn fruits. Pour boiling water over and leave for 2-3 hours. Take 0.5 cups three times a day.
Recipe No. 5. Place 3 tablespoons of horsetail in an enamel container and add 500 ml of cold water. Simmer over low heat for 20 minutes. Cool and strain. Drink during the day.