It is a well-known fact that protein is the basis for the creation of new cells, growth and development of a healthy body. Protein-rich foods are recommended for weakened people and patients with various pathologies for quick recovery. However, the appearance of protein in urine is a reason to consult a doctor. This is especially true for pregnant women, since proteinuria is a symptom that may indicate serious damage to internal organs that threaten the health and life of the fetus.
Causes of proteinuria in pregnant women
The kidneys in the human body play the role of a filter, purifying the blood of unnecessary products (ammonia, urea). Normally, proteins, due to their large size, are not able to penetrate the wall (membrane) of the tubules of these organs, which is somewhat reminiscent of a microscopic sieve, so the presence of proteins in urine may indicate a developing kidney pathology.
It should be understood that protein in the urine during pregnancy is not always a sign of illness. Due to the additional functional load on a woman’s urinary system, the efficiency of its work may change. The corresponding symptom should not cause panic in the expectant mother. It can be either a normal variant or a sign of pathology. The doctor’s task is to establish the safety of such a clinical situation.
Pathological
Possible causes of proteinuria during pregnancy:
- cystitis is inflammation of the bladder. The disease is additionally accompanied by discomfort when going to the toilet, increased body temperature;
- diabetes;
- pyelonephritis – a disease characterized by inflammation of the kidneys;
- oncology of the urinary system;
- gestosis is a pathological condition during pregnancy, accompanied by increased blood pressure, edema syndrome and the appearance of protein in urine;
- glomerulonephritis is a serious damage to the glomeruli of the kidneys with disruption of their function.
The above pathologies require appropriate treatment. Otherwise, the disease will progress, which threatens the health of the mother and child.
Physiological
It is also important to remember about situations when protein in the urine will be of a physiological nature:
- consumption of excess amounts of meat and dairy products;
- chronic stress;
- compression of the ureters by the fetus;
- improper collection of urine for analysis;
- increased body temperature of a woman;
- excessive physical activity.
These factors will also affect kidney function with increased concentrations of proteins in urine. When such effects on a woman’s body are eliminated, her condition quickly normalizes on its own.
Prevention of proteinuria
It is necessary to take preventive measures to avoid or alleviate proteinuria. The following recommendations should be followed:
- eat rationally and properly;
- Avoid excessive consumption of meat, fish, dairy products, fried and spicy foods, and do not drink coffee and chocolate;
- remove salt from the diet;
- limit the flow of fluid into the body;
- steam food or eat it boiled;
- monitor your weight;
- regularly measure blood pressure;
- avoid public places during outbreaks of viral diseases;
- monitor the cleanliness of the genitals and adherence to the rules of personal hygiene.
Routine examinations are intended for the timely detection of various pathologies. If the pregnancy is progressing normally, then you should take a urine test once a month, and after 30 weeks - weekly. With high blood pressure, blood circulation worsens. The placenta suffers and cannot provide the fetus with all the nutrients. Therefore, if protein is lost, a pregnant woman should be examined by her gynecologist for the entire 9 months. Even in a healthy woman, the kidneys, unable to withstand hormonal changes and enormous load, can fail.
( 8 ratings, average: 5.00 out of 5)
Characteristic symptoms
The severity of the clinical picture depends on the concentration of proteins secreted in urine and the underlying cause of the pathology. For example, traces of protein in urine during pregnancy may go unnoticed by the woman herself. The loss of a large number of them is accompanied by a number of characteristic signs:
- Constant fatigue is an early symptom that is often ignored.
- Deterioration in working capacity.
- Profuse vomiting in the first trimester.
- Violation of the standard urination schedule.
- Pain syndrome in the kidney projection area.
- Emotional lability.
- Marked fluctuations in blood pressure.
- Swelling under the eyes and on the face in the morning.
Advice! The appearance of the described symptoms requires consultation with a specialist. An early visit to a nephrologist or therapist will allow you to determine the type of pathology and begin its adequate treatment.
Causes
There are physiological reasons for increased protein content in the urine, associated with eating large amounts of protein foods, stress and physical activity. During pregnancy, this occurs due to the woman’s body adapting to bearing a fetus. An increase in the size of the uterus leads to compression of the kidneys and bladder. The organs of the urinary system work with double the load. Proteinuria caused by pregnancy occurs due to an increase in the level of hormones that affect the condition of the vascular membrane. Pathological causes are kidney disease, chronic or newly acquired vascular disorders.
The amount of protein in the urine indicates the state of the pregnant woman’s kidneys. The future health of the woman and child depends on this.
Reasons for the development of pathology:
- Pyelonephritis is an inflammatory disease of the kidneys that affects the parenchyma of the organ. The causative agents are pathogenic microorganisms that attack a woman’s weakened immune system during pregnancy. Proteinuria is observed in the presence of chronic pyelonephritis in the mother. The disease leads to disruption of the kidneys, in particular, the tubular urine filtration system.
- Glomerulonephritis is a kidney disease affecting the glomerular system of the organ. The transition to a chronic form of the course is dangerous for pregnant women.
- Hypertension is a persistent increase in blood pressure. The presence of vascular pathology in a woman’s history leads to the development of pregnancy complications with proteinuria in the analysis.
- Systemic autoimmune diseases. Diseases of this group are aggravated during pregnancy, there is a risk of impaired renal function, which is manifested by proteinuria.
- Diabetes mellitus is a disease of the endocrine system that leads to pathology of blood vessels. The filtration capacity of the kidneys depends on the condition of the walls of blood vessels.
- Preeclampsia is a pathological condition characterized by high blood pressure, vomiting and seizures. It is a complication of pregnancy. A urine test reveals a large amount of protein.
- Preeclampsia is a general definition of symptoms of toxicosis during pregnancy. The cause is chronic diseases of women, Rh conflict between mother and fetus, and hormonal imbalances.
Proteinuria in pregnant women is a dangerous condition and, when detected, requires a detailed examination of the woman.
How dangerous is this?
Proteinuria is not an independent disease, but a symptom that indicates dysfunction of internal organs. The danger of disruptions to the functioning of the relevant structures depends on the severity of the process and its localization. The sign cannot be ignored. In the absence of a clear understanding of the nature of the symptoms, the following complications may occur in a particular woman:
- attachment of pathogenic microorganisms (bacteria);
- dysfunction of the placenta, which provides normal nutrition to the child;
- development of acute or progression of chronic renal failure in the expectant mother;
- oxygen starvation of the fetus;
- developmental defects of the baby;
- premature placental abruption, childbirth.
An increase in protein concentration in urine during late pregnancy can be aggravated by the development of eclampsia. The pathology is accompanied by convulsions, a sharp rise in blood pressure and is an indication for a cesarean section.
Clinical manifestations
Diagnosis of proteinuria during pregnancy indicates the presence of the disease in the mother. Any violation affects the growth and development of the fetus and therefore requires medical intervention. Proteinuria in pregnant women is a symptom of many diseases, so the clinical manifestations of this disorder are as follows:
- increased body temperature;
- nausea and vomiting;
- high blood pressure;
- swelling;
- exacerbation of symptoms of chronic diseases;
- lower back pain.
The presence of proteinuria indicates the risk of developing severe gestosis. This condition is caused by insufficient functioning of a woman’s organs and systems due to the restructuring of the body for bearing a fetus. Toxicosis develops, which is a dangerous complication for the health of the mother and child. In the most difficult cases, eclampsia appears. The woman's condition is very serious, characterized by convulsive syndrome, high blood pressure, impaired urine outflow, and severe swelling. Possible loss of consciousness.
There are 4 stages of development of gestosis:
- Mild - minor swelling of the lower extremities, pressure rises to 150/90 mm Hg. Art. A woman often does not attach importance to the first signs of gestosis. The protein level is 0.033-0.1 g/l.
- Moderate - swelling intensifies and spreads to the abdominal area, sometimes the face, pressure rises to 170/100 mm Hg. Art. Protein level - up to 1 g/l.
- Severe - deterioration in general condition, swelling spreads to the whole body, pressure reaches 200/110 mm Hg. Art. More than 1 g of protein is found in the urine.
- Eclampsia - loss of consciousness, convulsions, vomiting, blood pressure 200/110. Lack of timely medical care is dangerous for the development of severe complications.
Severe gestosis is dangerous due to impaired blood supply to the brain, pathology of the nervous system, cardiovascular failure, loss of vision, and the development of coma.
Diagnostics
A woman can independently suspect the presence of increased protein in the urine during pregnancy. Turbid early urine indirectly indicates a violation of the filtration function of the kidneys. Such diagnostics are inaccurate. Therefore, to determine the amount of proteins in the urine, it is necessary to carry out appropriate laboratory tests (analyses).
Methods
At the moment, hospitals traditionally use two main tests to judge the concentration of proteins in urine:
- General urine analysis. A simple and accessible method that allows you to detect proteinuria. The procedure is one of the mandatory tests for pregnant women for a comprehensive diagnosis of their health.
- Biochemical urine analysis. A study that allows you to evaluate the concentration of protein in urine throughout the day.
Quality control of the appropriate analysis during pregnancy is an important aspect in the prevention of pathologies of the urinary system in expectant mothers. After registration, each woman must undergo a comprehensive examination using the above methods.
Urine collection rules
The reliability of the research depends on the quality of preparation of biological material for analysis. To minimize the risks of obtaining a false positive final result or distorting real data, you need to:
- Before collecting urine, prepare a clean, disposable container for liquid secretions. You can buy such a jar at any pharmacy;
- carry out hygiene of the external genitalia;
- determination of protein in urine involves assessing the morning portion of urine. All secretions are collected in a previously prepared container. After this, 100-200 ml is poured into a container, which is delivered to the laboratory within 2 hours;
- When collecting urine, the vagina must be covered with a cotton swab or a tampon. Otherwise, red blood cells (during menstruation), white blood cells or epithelial cells may enter the sample, which will distort the final results.
If a biochemical analysis is carried out, then daily urine must be collected. All the liquid is mixed in one container, and then the patient delivers 100-200 ml of a sample of biological material to the laboratory.
What additional research is being carried out?
Detection of protein in urine requires a more thorough diagnosis of the function of the urinary system. For this, doctors use additional procedures:
- Ultrasound of the abdominal organs and kidneys. The method allows you to estimate the size and shape of internal structures;
- excretory urography - an x-ray examination that can be used to judge the functional activity of the organs of the urinary system;
- Cystoscopy is an endoscopic technique that provides visualization of the bladder cavity.
If necessary, the doctor individually selects auxiliary diagnostic procedures to determine the cause of the appearance of protein in the liquid secretions of a pregnant woman.
How to prepare for a urine test
Let's look at how urine is collected for analysis. The bladder is emptied in the morning. The first portion of urine is not examined. The analysis requires urine, which will be collected throughout the day until the next morning. Urine must be delivered to the laboratory within 2 hours.
General recommendations before taking a urine test:
- You can't be nervous or worry. Due to stress, readings may change.
- The day before, you should exclude foods rich in proteins from your diet: eggs, meat, cottage cheese, milk and fish.
- Do not engage in physical labor or overexert yourself.
- Do not use medications.
- Do not overcool the body.
The urine collection container must be sterile. Before collecting urine, the genitals should be toileted. It is advisable to insert a tampon into the vagina so that the discharge does not accidentally get into the urine.
For analysis, average urine is needed, so the first and last stream goes down the toilet. You should try not to shake the container during transportation. If foam in the urine does not go away for a long time, this may be a sign of proteinuria.
Decoding the results
Urine analysis for the presence of protein is in most cases carried out automatically. This guarantees highly accurate final results. The norm of protein in urine during pregnancy:
| Index | Trimester | ||
| I | II | III | |
| Protein, g/l | |||
| Daily protein loss, mg | |||
If there are deviations from the figures indicated in the table, the doctor must correctly assess the clinical situation. For example, a slight increase in protein concentration in urine to 0.05 g/l against the background of preliminary physical activity without the presence of objective symptoms of pathology can be interpreted as a variant of the norm.
At the same time, 1 g of protein in the urine in combination with morning edema and general weakness indicates kidney dysfunction and requires appropriate treatment. Correctly deciphering the final results of the described laboratory test is the art of a doctor, which involves a comprehensive assessment of a woman’s condition, and not just an analysis of dry numbers.
Causes of high protein content in urine
Pregnancy is a physiological process that requires a woman’s body to adapt to changes in the functioning of all organs and systems.
Protein secretion increases due to:
- formation of lordotic posture (pronounced forward curvature of the lumbar spine, tilting back of the upper body, protrusion of the abdomen);
- increased functional load on the urinary system;
- physical pressure of the enlarged uterus on the kidneys and ureters;
- changes in venous outflow.
Proteinuria is predominantly a manifestation of exacerbation of pre-existing overt or latent chronic kidney diseases, as well as toxicosis of pregnancy.
Most often aggravated:
- pyelonephritis;
- glomerulonephritis;
- diabetes;
- polycystic kidney disease;
- hypertonic disease;
- urinary system infections;
- systemic diseases.
Proteinuria can be transient or permanent, associated with the functioning of the kidneys and independent of the condition of the renal tissue. It is important to eliminate as much as possible factors that provoke increased protein excretion in the urine.
Treatment methods
Proteinuria is a symptom indicating a dysfunction of a particular organ or entire system. Adequate therapy is based on identifying the root cause of the clinical symptom with further impact on it.
Medication
Treatment with tablets and injections is justified for moderate and severe proteinuria. Depending on the root cause of the symptom, doctors use the following groups of drugs:
- antibiotics. Antimicrobial agents are effective only if the presence of a pathogen in the patient’s body that causes the disease is confirmed. During pregnancy, penicillins (Amoxicillin, Ampicillin), macrolides (Erythromycin) and cephalosporins (Ceftriaxone, Cefepime) are allowed;
- insulin. Pancreatic hormone, which is used in patients with diabetes;
- diuretics. Drugs (“Furosemide”, “Hydrochlorothiazide”) are used for severe edema syndrome;
- antihypertensive drugs. Proteinuria is often accompanied by increased blood pressure. To reduce it in pregnant women, Labetalol, Amlodipine, and Methyldopa can be used.
The selection of medications is carried out on an individual basis depending on the severity of the patient’s condition.
Diet
Reducing the concentration of protein in the urine can also be achieved through dietary restrictions. Fried and smoked dishes are excluded from the menu. Salt consumption is reduced to a minimum. The drinking regime is selected by the doctor individually, depending on kidney function. In most cases, it is recommended to limit the amount of fluid consumed to 1.5-2 liters per day.
The therapeutic diet involves increasing the amount of fresh vegetables, fruits, cereals, and dairy products. At the same time, the volume of protein foods decreases.
Prognosis for recovery and undesirable consequences
In 90% of cases, proteinuria in pregnant women resolves spontaneously within a few weeks after birth. With timely initiation of therapy, it is possible to achieve stabilization of a woman’s condition by the last trimester. Complete restoration of the functions of the urogenital tract takes from 3 to 8 months, which is associated with the gradual healing of damaged areas and normalization of hormonal levels. The likelihood of developing complications is influenced by the following factors:
- multiple pregnancy (2 or more embryos);
- a child with developmental defects;
- the woman has serious diseases of the urinary and cardiovascular systems;
- bacterial, fungal and viral infections.
When I was doing an internship in the intensive care unit of one of the city clinics, a girl with proteinuria was admitted to us. The patient was only 18 years old and this was her first pregnancy, so she did not understand the danger of developing such a condition. The doctors insisted on hospitalization and planned delivery by caesarean section, but the girl wrote a refusal and went home to give birth to the child in other conditions. At the beginning of the contractions, she experienced premature detachment of the placenta (baby place), resulting in extensive bleeding. The patient was rushed to the hospital and operated on, but due to the risk of infection, the girl had her uterus removed.
What complications may occur in women with proteinuria during pregnancy:
- premature detachment of a normally located placenta;
- development of bleeding and hemorrhages in various organs and tissues (brain and spinal cord, eyeballs, kidneys, liver);
- the formation of uremic intoxication (accumulation of ammonia and urea in the mucous membranes);
- alveolar pulmonary edema;
- the occurrence of acute or chronic kidney failure;
- disruption of metabolic processes in the body;
- premature onset and weakness of labor;
- secondary infection and damage to the uterus, ovaries or tubes;
- infectious-toxic shock;
- hydronephrosis - stretching of the renal pelvis and its deformation;
- increased risk of developing a hypertensive crisis - a spontaneous increase in blood pressure;
- stroke is an acute disorder of cerebral circulation.
Photo gallery: undesirable consequences of the disease for a woman’s body
Hydronephrosis is stretching and deformation of the renal pelvis
Uremia is accompanied by the deposition of toxins in the internal organs
Premature placental abruption leads to bleeding
Lifestyle correction
During pregnancy, women can partially or completely stabilize the concentration of proteins in urine on their own. To do this you need:
- Visit your doctor regularly to monitor proteinuria;
- eliminate excessive physical activity;
- minimize stress;
- spend more time in the fresh air;
- use loose clothing;
- follow all doctor's orders.
Additionally, we must not forget about proper sleep and rest. Very often, the appearance of protein in the urine is not a serious problem. To stabilize kidney function, it is enough to exclude the influence of negative external and internal factors.
The formation of proteinuria in the human body
As part of their primary function, the kidneys filter small amounts of protein from the bloodstream. This is how it appears in primary urine.
Next, the mechanism of protein reabsorption in the renal tubules is triggered. The result of the functioning of healthy kidneys and the absence of excess proteins in the blood plasma is the presence of a small amount of protein in secondary urine (the fluid that is excreted from the body).
A laboratory test of urine does not detect proteins at this concentration, or gives a result of 0.033 g/l.
Exceeding this value is called proteinuria - the content of protein in urine in large quantities. This condition is a reason for further diagnosis in order to identify the causes of the disorder.
Kidney examination
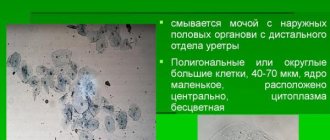
Microscopy of urine sediment
Detection of specific casts by microscopy of urine sediment often indicates the etiology of the disease.
- hyaline casts - concentrated urine after physical activity;
- red blood cell casts - glomerulonephritis;
- leukocyte casts - pyelonephritis, interstitial nephritis;
- cylinders of the renal tubules - acute tubular necrosis, interstitial nephritis.
Fractional sodium excretion (FENa%) and urine osmolality (UOsm)
Electrolyte levels and osmolality help in the differential diagnosis of prerenal azotemia and other kidney damage:
- prerenal azotemia - FENa 500;
- acute tubular necrosis - FENa >1, UOsm 250-300;
- glomerulonephritis - FENa 5 g/day diagnoses severe preeclampsia. However, proteinuria is not detected in all cases of preeclampsia, and it is not necessary for clinical diagnosis. In fact, proteinuria is absent in 14% of cases of eclampsia and 13% of cases of HELLP syndrome (hemolysis, increased liver enzymes and low platelet levels). In the absence of proteinuria, clinical diagnosis is made using hypertension and other clinical characteristics—newly diagnosed liver dysfunction, increased platelet count, and platelet count 30 mg/mmol. While 24-hour proteinuria remains the gold standard for diagnosing significant proteinuria, in pregnancy the urinary protein/creatinine ratio shows a reasonable correlation with 24-hour proteinuria and can be used to provide timely results in the treatment of new and outpatient patients. The advantage of determining the protein/creatinine ratio in urine is the possibility of excluding significant proteinuria and overdiagnosis of preeclampsia. Some authors have not found a specific cut-off point for excluding significant proteinuria, others have suggested a reasonable exclusion ratio of 0.2.
Although there is widespread agreement that the urinary protein/creatinine ratio is a valid alternative, there are still situations in which 24-hour proteinuria testing or serial measurement of the urinary protein/creatinine ratio may be recommended. It is believed that with high levels of proteinuria, the correlation of the protein/creatinine ratio in urine is lost, and daily proteinuria will improve the diagnosis of severe preeclampsia. In addition, serial determination of urinary protein/creatinine ratio or 24-hour proteinuria may confirm the progression of gestational hypertension to mild preeclampsia.
Glomerulonephritis
When admitting patients with edema, hypertension and acute renal failure, it is difficult to differentiate from preeclampsia. Edema is often found in the periorbital area, vulva and extremities. Since treatment of preeclampsia must be carried out according to an urgent special plan, the first task of the clinician is to exclude glomerulonephritis from the differential diagnosis. Urinalysis tests for hematuria, red blood cell casts, white blood cells, and mild to moderate proteinuria. Because of the characteristic etiology of glomerulonephritis, a comprehensive serologic evaluation and possibly a renal biopsy are necessary. The treatment plan depends solely on the specifics of the disease.
Acute tubular necrosis
Acute tubular necrosis usually occurs after hypovolemic or septic shock and is accompanied by sudden severe hypotension. However, tubular damage can be caused by nephrotoxic substances. They come exogenously, as with the administration of aminoglycosides or radiological contrast agents, or endogenously due to rhabdomyolysis. A history of turbid brown urine or the presence of renal tubular casts and FENa >1 in the urine can distinguish acute tubular necrosis from other renal disease.
Treatment is strict fluid balance to avoid overload and supportive care. Although large doses of furosemide are commonly used to improve diuresis, randomized trials have found that such treatment has no effect on the rate of recovery.
Prerenal azotemia
Prerenal azotemia is the most common type of renal failure in the absence of pregnancy. Prerenal azotemia in pregnancy is the result of decreased intravascular volume or changes in vascular resistance; decreased intravascular volume occurs with bleeding, dehydration, GI losses, or trauma. Renal vascular resistance increases when taking various drugs - NSAIDs or when perfusion decreases due to renal artery stenosis. Urinalysis, FENa, and blood urea nitrogen/creatinine ratio (usually >20:1) help differentiate between prerenal azotemia and kidney disease. Treatment is correction of intravascular volume deficiency or removal of the etiological agent.
Obstructive uropathy
The importance of identifying urinary tract obstruction as a cause of proteinuria is that the problem can be easily remedied. Patients usually present with complaints of pain in the lower abdomen or girdle pain. Urine electrolyte testing reveals low FENa, high osmolality, and a high blood urea nitrogen/creatinine ratio. Ultrasound reveals bilateral hydronephrosis or enlarged bladder. The severity of hydronephrosis allows for differential diagnosis with physiological hydronephrosis, observed in most pregnant women. Once the obstruction is removed, post-obstructive diuresis occurs and fluid balance must be monitored to prevent hypovolemia.