The term leukocyturia refers to a condition in which there is an increase in the number of leukocyte cells in a urine test. This condition is not a variant of the physiological norm, therefore the laboratory technique for determining leukocytes in urine is used as an informative method that allows one to identify certain diseases, infectious and non-infectious in nature. If leukocyturia was detected in the results of the urine analysis, then this criterion indicates the development of an inflammatory process in the body.
Causes of leukocyturia
Leukocyturia usually occurs during inflammatory processes in the following organs:
- Bladder . In this case, the patient has cystitis. The infectious form develops due to chlamydia, ureplasma, E. coli, and candida fungi entering the organ. In addition, the development of this disease is facilitated by problems with blood circulation in the pelvic area due to frequent sitting, diabetes, menopause, tight underwear, frequent constipation and deterioration of the immune system.
- Pelvis . In this case, the person has pyelonephritis. Inflammatory processes can be caused by Escherichia coli and Pseudomonas aeruginosa, staphylococci, enterococci, and Proteus. They penetrate the kidney from the source of infection in a hematogenous manner, although descending pyelonephritis is also possible when the infection passes from the urinary tract or ureter.
- Interstitial tissue of the kidneys . In this case, the patient has interstitial nephritis. The cause may be a viral or bacterial infection, an autoimmune reaction, or toxic-allergic processes.
In addition, leukocyturia is detected in prostatitis, tuberculosis of the kidneys and bladder, urolithiasis and other urological ailments. Pyuria (the so-called severe form of leukocyturia) is found in purulent pyelonephritis and hydronephrosis.
A minor form of deviation is usually present in renal failure (chronic), nephrotic syndrome, early stage of glomerulonephritis, helminthic infestation, allergies, fever. Leukocyturia can be caused by drugs such as Kanamycin , Ampicillin , Aspirin .
In pregnant women, the presence of pus in the urine occurs due to infectious processes in the kidneys, urinary tract, and vagina. In children, leukocyturia is often false. It is caused by poor personal hygiene.
WHAT CAN LEUKOCYTES TELL US
Leukocyturia in origin can be extrarenal - with pathology of the urinary or (in men) reproductive system and renal - with damage to the glomeruli and tubules. The nephron source of leukocytes is indicated by the presence of leukocyte or leukocyte-epithelial casts .
allows for topical diagnosis .
three-glass Thompson test
The cause of minor (up to 40 in the field of view) or moderate (50–100) leukocyturia may be the onset of acute glomerulonephritis , often chronic renal failure, nephrotic syndrome .
A moderate increase in the number of leukocytes may be aseptic in nature. While pyuria - cloudy urine, leukocytes cover the entire field of view or form clusters - in almost all cases it has an infectious genesis (apostematous nephritis, rupture of border abscesses, purulent inflammation of the urinary tract).
Features of the leukocyte profile of urine are determined by the etiology and pathogenesis of diseases leading to the development of leukocyturia.
Polymorphonuclear neutrophils accompany glomerulo-, pyelonephritis, inflammatory diseases of the urinary tract, chronic renal failure, chronic prostatitis.
Lymphocytes (abacterial or autoimmune damage) are characteristic of primary and lupus glomerulonephritis, interstitial nephritis, amyloidosis, kidney cancer, chronic host-versus-graft reaction.
Eosinophils (>1% in urine) are found in acute interstitial nephritis of drug (allergic) origin, cholesterol embolism of the kidneys, acute host-versus-graft reactions; possible with acute tubular necrosis, glomerulonephritis, diabetic nephropathy, urinary tract infection, polycystic disease, renal thromboembolism.
If there is a persistent increase in the number of leukocytes in the urine against the background of low pH values, tuberculous kidney damage .
“Active” leukocytes are characteristic primarily of acute inflammation of the kidney tissue. However, the method of identifying them, as well as provocative tests to detect latent leukocyturia, are currently practically not used. A replacement can be the test strip method, which is based on the active response of leukocytes (esterase level) to a bacterial pathogen.
Leukocyturia without bacteriuria can be observed with:
- high body temperature (not associated with kidney disease),
- pregnancy,
- the use of glucocorticoids, allopurinol, acetylsalicylic acid, iron salts, levodopa, after exercise,
- antibiotic therapy (ampicillin, methicillin, kanamycin),
- with interstitial nephritis,
- prostatitis,
- host versus graft reactions.
Simultaneous detection of leukocyturia and bacteriuria (>104 CFU/ml) plays an important role in the diagnosis of inflammatory diseases of the kidneys and urinary tract, even in the absence of symptoms.
Types of leukocyturia
True and false leukocyturia are distinguished The first is characterized by the formation of leukocytes directly in the urinary system, and the second is due to the release of secretions from the genital organs into the urine.
Depending on the pathogen, the pathology can be infectious or non-infectious . If the number of leukocytes is increased, but there are no bacteria in the urine, then such leukocyturia is considered sterile (aseptic).
Depending on the type of cellular structures identified, neutrophilic , mononuclear , eosinophilic and lymphocytic forms of pathology are distinguished. In terms of quantity, it can be insignificant (up to 40 cells in the field of view), moderate (up to 100 units) and pronounced (the entire space is covered with leukocytes).
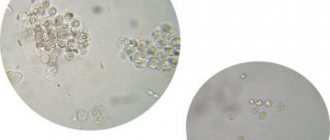
Leukocyturia in urine - what does it mean?
Leukocyturia is the most common abnormality in laboratory tests. This result means an increase in the level of leukocytes in the urine, however, there is a clear boundary between normality and pathology - if a laboratory technician sees a maximum of 6 leukocytes, then we are talking about normality. Exceeding this indicator even by one is a reason to conduct additional examinations of the patient to find out the cause of leukocyturia.
Why does the level of leukocytes increase in urine? The mechanism is explained simply: if an inflammatory process occurs in the organs of the urinary system and in nearby organs, then leukocytes will be present in large quantities in the urine.
According to the International Classification of Diseases (ICD 10), the condition in question has code 39.0.
Symptoms
With a pathological increase in leukocytes, discomfort and pain appear when urinating. The liquid itself has a cloudy tint, and whitish flakes of pus are clearly visible in it.
Secondary symptoms are:
There are symptoms that indicate the presence of infections in the urethra. To those already listed, you can add pain and discomfort in the lower abdomen and groin, dysuria (difficulty or frequent urination), and unpleasant odor of urine.
Diagnostics
For diagnosis, 2 main methods are used - the two-glass and three-glass test method. In the first case, when collecting urine, the liquid is immediately divided into 2 parts. If the number of leukocytes in the first part is increased, then inflammatory processes develop in the urethra or prostate, and if in the second part, then this is associated with the kidneys, bladder or ureters.
As for the three-glass sample method, in this case the urine is divided into 3 portions. If purulent accumulations are present in the first, then this is the initial stage of pyuria, in the last - the final stage. If there is sediment in all portions, then this is a manifestation of complete pyuria.
The following methods are known for collecting urine:
In addition, the doctor examines not only the amount of urine and sediment in it, but also the color and size of leukocytes (they can be 2-3 times larger than normal and have a blue color). Additionally, an ultrasound of the bladder and kidneys is performed.
How to collect urine from infants
Collecting urine from a small child is not as easy as it might seem at first glance. This process can be accompanied by many errors, especially if the parents are young and do not know how to properly collect tests for their baby. Often inappropriate methods are used, which is why test results are completely disappointing and make parents think that something is wrong with their child. Let's look at all the possible methods of collecting urine and figure out why some of them are completely unacceptable to use.
- Wringing out a diaper or diaper . Yes, yes, this method may seem strange to many. But there are also many parents who can’t think of anything better than this kind of squeezing. So, this method is completely unsuitable, so forget about it forever! The fact is that the diapers are filled with gel, which absorbs all incoming moisture. And even if your attempts at push-ups end in success, you will be able to collect not the baby’s urine, but the dissolved gel. The situation is the same with a diaper: passing through the material, urine is filtered and many components do not get analyzed. What kind of accuracy of analyzes can we talk about? They will certainly show that the baby has a lot of leukocytes in the urine.
- Pouring from a pot . Another wrong option. Of course, if you are using an old enamel pot, you can boil it before collecting urine. But most night vases today are plastic, and it is not possible to properly disinfect them. And even if you wash it well, the tests will still not show the best results.
- Using a jar . This option is more acceptable. But before collecting urine, such dishes should be thoroughly washed, boiled, or doused with boiling water several times, and then dried thoroughly.
- Using a urine collector. This is the most convenient and acceptable way to collect tests from infants. However, it also has some disadvantages. Such urine collectors are presented in the form of plastic bags that have a teardrop-shaped hole and an adhesive substance that makes it possible to attach the urine collector wherever necessary. Before using it, the baby should be thoroughly washed. The most important thing is that you should not leave the urine collector on the child’s body all night, because during this time the baby will urinate more than once, which will greatly complicate the correct diagnosis. And, of course, we cannot rule out the fact that the urine bag may simply come off, and it can certainly disturb the baby, so it is possible that he will remove it himself. Therefore, when using such devices, be careful, try to monitor the child until he does his business, and then immediately disconnect the bag.
Treatment of leukocyturia
Once a pathology is detected, a detailed diagnosis of the human body is required to determine the underlying disease. After the type of leukocyturia is differentiated, the doctor will develop a treatment strategy.
If it is caused by infections, then antibacterial therapy , that is, antibiotics are used. As a rule, drugs from the cephalosporin group are used. Penicillin-type antibiotics and fluoroquinolones are also suitable. In addition, the patient is prescribed enzymatic agents that help reduce the risk of side effects. If the presence of pus in the urine is caused by urogenital pathologies in which ureoplasma or chlamydia are detected, then tetracycline medications are prescribed.
Pregnant women are prescribed only new generation cephalosporins, as they do not have serious side effects and are relatively safe for the woman and the fetus.
If leukocyturia is aseptic, then treatment will be local. The doctor prescribes antiseptics. They are used for douching and irrigation. Patients are also recommended to use immunomodulators, ascorbic acid and B vitamins. It is imperative to observe the rules of personal hygiene.
To reduce the likelihood of recurrent leukocyturia, it is necessary to carry out therapy again: antibiotics are prescribed for 7 days for prophylactic purposes. As a rule, this is carried out a month after the main treatment.
How to distinguish normality from pathology?
There is no consensus on the definition of normal limits for the number of leukocytes.
Some researchers argue that the following should be considered normal:
- for girls up to 10 cells;
- for boys – up to 6.
Others insist that this figure approaches zero in a healthy person, but admit:
- for boys – 0–2;
- girls – 0–3.
With diathesis in a child, leukocyturia can increase to 5–7. The upper limit for women is considered to be 8 in the field of view, for men – 6 (according to other sources, 6 and 3, respectively).
The appearance of leukocyturia without pathology is explained by:
- the ability of a small number of cells to penetrate the wall of blood vessels and enter the urine;
- the presence of observation cells for the state of organ protection;
- in children, increased permeability of glomerular membranes due to functional underdevelopment.
Increased standards for girls and women are determined by anatomical features. Their urethral outlet lies close to the anus, so there is always the possibility of intestinal flora entering and requires additional protection.
In diagnosis, one cannot rely on the absence of characteristic symptoms of diseases, because a latent course is possible when a person feels completely healthy. The appearance of asymptomatic leukocyturia means that it is necessary to prove the absence of pathological changes by additional studies.