The Latin term “hematuria” refers to the presence of blood in the urine. Patients notice the appearance of a reddish color to the urine. The intensity of the color depends on the volume of blood. It is customary to distinguish:
- microhematuria – the presence of blood (erythrocytes) is confirmed only by microscopic examination of the sediment;
- macrohematuria - urine becomes similar to meat slop and has a dark red color.
Normally, in a healthy person, no more than 2 red blood cells can be detected in the field of view. In urine collected over 12 hours, the number of cells should not exceed 105. If more are detected in the laboratory, the symptom is regarded as a possible pathology, and the doctor is obliged to identify the causes of hematuria.
Microhematuria as a variant of normal and incorrect collection of urine analysis
The presence of microhematuria does not always indicate illness. A slight increase in the number of red blood cells in the urine is possible when collecting an analysis:
- after alcohol abuse, eating spicy and salty foods;
- visiting a steam room or sauna;
- prolonged overheating in the sun;
- unrest suffered.
Microhematuria may appear after walking or running long distances in athletes. A similar condition is known among soldiers during a forced march; there is even a name for “march hematuria.” What this is, from the point of view of the development mechanism, remains unclear. Long-term observation of men with previously identified marching form indicates the absence of a connection with any renal changes.
This symptom lasts a short time and quickly disappears on its own if you stop physical activity.
Persistent red color of urine may indicate pathology. Sometimes patients mistake this color for hematuria after eating foods with dyes, beets, and carrots.
Repeated analysis after dietary restrictions reveals the truth
On the other hand, there are known diseases in which microhematuria does not manifest itself consistently. An example is nephroptosis (prolapse of the kidney), pathological mobility: red blood cells enter the urine when the patient is in an upright position, and disappear when lying down. Macrohematuria does not occur in a healthy person. Most often it indicates damage to the kidneys or urinary tract.
Discharge from the genitals is mistakenly taken for hematuria. For women it is:
- prolonged menstruation;
- cervical erosion;
- uterine bleeding due to fibroids;
- postpartum disorders.
Hematuria in men may be associated with exacerbation of prostatitis, benign prostatic hyperplasia.
Causes of changes in urine color that are not hematuria
Bloody urine coloration may occur in other conditions that are not related to kidney or urological diseases. For example, the color of urine can change color depending on the consumption of certain foods (beets, rhubarb), and medications. In this case, even if the urine is colored red, it will not be called hematuria, since this phenomenon is due to other known causes.
Nitrofuran preparations color urine yellow, senna preparations color it brown.
Extrarenal hematuria
The mechanism of blood getting into the urine may be due to:
- Destruction of the fibrous capsule of the kidney or the lining of the urinary tract due to injury, tumor disintegration - bladder cancer is the most common cause of hematuria in elderly men, and in young and middle-aged men - prostate adenocarcinoma.
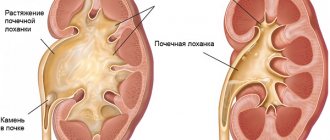
- Urolithiasis - accompanied by the passage of stones and their movement through the ureters.
- Massive inflammation with ulceration of the bladder wall - hematuria in women is caused by chronic cystitis, inflammation increases the permeability of the vascular wall, loosens the tissue of both arteries and veins entering the vascular bundle of the urinary organs (bacterial damage, schistomatosis, tuberculosis, chlamydia).
- Mechanical compression of blood vessels by a growing tumor or enlarged pelvis (hydronephrosis), which causes local stagnation and increased permeability due to pressure drop.
- Blood diseases with coagulation disorders (hemophilia), overdose of anticoagulants are a factor in damage to any organ, including the urinary system.
Oxalate stones, which have sharp edges, are especially damaging to the walls of the ureters.
In diseases accompanied by cardiac decompensation, hematuria manifests itself as a sign of general congestion in the venous network of the pelvis. Phlebitis and minor thrombosis in the veins form, they increase the pressure from inside the vessel and move red blood cells into the urine.
Treatment
According to existing standards, urethrorrhagia and gross hematuria are indications for hospitalization of a patient in a surgical hospital where a urology clinic is located, sometimes even for emergency reasons. The purpose of such hospitalization will be conservative therapy aimed at preventing possible blood loss, stopping bleeding and examination. If the presence of extraglomerular hematuria is proven, treatment of the underlying disease is necessary. But much more often the source of bleeding is trauma, tumors, urolithiasis and other urological causes. In this case, hemostatic drugs, vitamins, calcium supplements, etamsylate are prescribed, and in severe cases, blood plasma transfusion of the same group is prescribed, or the necessary surgical intervention is performed.
In conclusion, it should be said that “treating urine with blood” never ends with actually stopping the bleeding. A certain category of people asks in a search engine such queries as, for example, “treatment of hematuria with folk remedies” or “blood in urine treatment drugs,” which is quite illiterate. Such requests are completely meaningless. In addition, they are very harmful to those who asked them, since they indicate that the patient does not know the cause of the development of the pathology and wants to cure only the symptom, which may be a manifestation of injury, cancer, inflammation, urolithiasis or systemic pathology. You need to understand that only an urgent consultation with a urologist will answer these questions.
Renal hematuria
The mechanism of renal hematuria is associated with disruption of the structural components:
- Destruction of the nephron membrane. It filters urine and normally retains red blood cells in the glomeruli. The process occurs with any type of inflammation of the parenchyma (pyelonephritis, glomerulonephritis). The basement membrane is affected both by nonspecific infectious and autoimmune inflammation.
- Toxic effect on the tubules, interstitial tissue of toxic substances, medications in case of overdose (Cyclophosphamide, Heparin, Warfarin), poisoning, individual intolerance, polycystic kidney disease.
- Increased intravascular coagulation against the background of antiphospholipid and disseminated intravascular coagulation syndromes.
- Systemic diseases that occur with damage to the capillary wall (hemorrhagic fevers, diathesis, blood diseases). They cause local destruction of glomerular filtration and increase the permeability of the basement membrane.
Destruction of the glomerular apparatus underlies hematuria in diseases with a hereditary form of transmission. These include:
- essential and HCV-associated mixed cryoglobulinemia;
- Fabry disease;
- IgA nephropathy;
- Goodpasture's syndrome.
Tissue necrosis with hematuria accompanies sickle cell anemia, renal vein thrombosis, renal infarction, and malignant hypertension.
According to another classification, the causes of hematuria are divided into:
- on prerenal – arose without connection with kidney pathology (in infectious diseases, sepsis, food poisoning);
- renal or renal - necessarily associated with the kidneys;
- postrenal - depend on destructive processes in the underlying urinary tract (stone in the ureter, bladder tumor, anomalies, cystitis, urethritis).
The above facts confirm the need to determine the cause of blood in the urine using modern diagnostic methods.
Probable causes of pathology development
The urine of a healthy person is a light yellow or transparent liquid with a specific odor. Any changes in the color of urine or the presence of impurities are a sign of a problem in the patient’s body. If urination is accompanied by attacks of pain, then, most likely, hematuria is associated with the release of stones, the flow. A painless process of emptying may indicate the presence of cancer or damage to internal organs.
It is difficult to independently determine the cause of the appearance of blood in the urine; specific studies are required to make a diagnosis. Today, there are more than 150 types of diseases that lead to the appearance of blood in the urine. All pathological conditions require treatment and lifestyle adjustments. Lack of medical care leads to severe complications, including death.
Doctors identify several probable causes of the formation of pathology:
- The most common disease leading to hematuria is urolithiasis. Damage to the walls of the excretory tract occurs against the background of the movement of stones. Urination with this disease is almost in all cases accompanied by pain;
- Inflammatory processes take second place. Pathogenic microorganisms damage the walls of blood vessels, red blood cells easily penetrate the urethra. The course of the inflammatory process is accompanied by an increase in body temperature, pain in the lumbar region;
- oncological formations. Tumors in the urinary system grow, damage the walls of the canals, which leads to the release of not only blood, but patients also find clots of red blood cells in the urine. The course of the oncological processes shows almost no signs of itself, urination occurs as usual, there is no discomfort;
- various injuries to the urinary system. Fresh blood clots appear in the urine;
- . An inflammatory process in the bladder is often diagnosed in women due to the specific structure of the urethra. Bacteria easily penetrate into it, then into the bladder, leading to cystitis. Blood in the urine characterizes the hemorrhagic form of the pathology; it is also characterized by the patient’s general malaise and pain during bowel movements;
- taking hormonal contraceptives. In some cases, drugs provoke blood stagnation and inflammatory processes in organs, which leads to the release of blood along with urine;
- Eating beets in large quantities, foods/medicines rich in dyes can lead to coloration of urine. Some patients perceive the color change as blood;
- menstrual irregularities. In such a situation, blood may be released from the vagina, and the woman will decide that red blood cells were in the urine. A similar situation is observed during pregnancy; many women mistake a small amount of blood in the urine for disturbances in the functioning of the excretory system, rather than the genital organs.
Hematuria code according to ICD 10 - N02 (recurrent stable), R31 (nonspecific hematuria).
What are the symptoms of hematuria?
Hematuria itself is not a disease, but a symptom. Its appearance alarms the attending physician, since it is often accompanied by an exacerbation of the disease. This is especially true for gross hematuria.
In case of massive bleeding from the kidney due to injury, neoplasm, from the bladder due to prostate cancer and adenocarcinoma, intensely colored urine with clots appears against the background of urination
It is possible that the ureteric openings and bladder neck may be blocked by clots. A significant amount of urine mixed with blood accumulates. The muscles are overstretched. The condition is called "bladder tamponade." Clinically accompanied by acute urinary retention:
- with pain above the pubis, radiating to the lower back, side wall of the abdomen;
- constant urge to urinate;
- urine leakage;
- nausea;
- temperature rise.
Hematuria (usually gross hematuria) is part of the nephrotic syndrome along with arterial hypertension and edema. The appearance of this combination indicates acute glomerulonephritis or exacerbation of chronic.
At the same time, signs of renal failure are detected:
- oligo- and anuria;
- increase in creatinine in the blood;
- protein in urine.
If renal hypertension causes acute heart failure, then the following appear:
- dyspnea;
- swelling in the legs;
- cough with phlegm;
- tachycardia.
A decrease in hematuria or its disappearance indicates the subsidence of the inflammatory process and the transition of chronic nephritis to the remission stage. Metabolic disorders caused by changes in the function of tubular reabsorption (accumulation of calcium, urea) contribute to prolonged microhematuria.
End-stage renal failure occurs:
- with hematuria,
- anemia,
- diarrhea,
- impaired brain function (confusion, seizures),
- ulcerative stomatitis,
- urea secretions on the skin.
Gross hematuria in bladder cancer is combined with prolonged fever and pain
Urolithiasis is characterized by acute colic, the pain is very intense, spreading to the lower back, half of the abdomen, groin, and external genitalia. Hematuria occurs after pain and is accompanied by increased urination. Usually there is a connection between the attack:
- with long walking or shaking in transport;
- drinking alcohol.
Asymptomatic hematuria complicates the diagnostic task. When the etiology of bleeding in the urine is unclear or the hematuria is not permanent, the patient must undergo a comprehensive examination to exclude diseases that cause this manifestation.
Prevention
There are several ways to prevent hematuria in females:
- promptly treat inflammatory and infectious processes of the genitourinary system;
- drink at least 1.5 liters of water per day, watch your diet (most diseases of the urinary system are associated with the abuse of harmful foods);
- If any unpleasant symptoms appear, immediately visit a doctor, identify the cause of the pathology, and begin treating the disease.
Hematuria in the fair sex is a common occurrence. It is important to consult a doctor in time to cure the pathology. Most diseases that lead to the appearance of blood in the urine can lead to serious complications. You can avoid negative consequences by taking care of your health.
Find out more about what bladder hematuria is in women, about the types and methods of treating pathology after watching the following video:
Causes of hematuria
underlie the understanding that hematuria is a symptom of
kidney and urinary tract diseases
. Blood in the urine is more often detected during laboratory tests; patients rarely complain about its appearance on their own.
Blood in the urine is visible to the naked eye at a concentration of 5 ml per 1000 ml. It gives the urine a red color, characteristic of bleeding, only during the first few hours, then the urine becomes brown. In this regard, this symptom cannot be reliably excluded only on the basis of the patient’s complaints.
Urine may turn red when taking certain medications (phenindione, rifampicin) and foods (beets). With intravascular hemolysis, free hemoglobin appears in the urine, and with rhabdomyolysis, myoglobin is determined.
Henoch-Schönlein purpura
Pathological changes resemble manifestations of IgA nephropathy. Red blood cells and urinary casts are also detected in the urine. The diagnosis is usually made by suspected skin and joint manifestations. In adults, renal pathology is more pronounced.
Benign familial hematuria
The disease manifests itself with recurrent episodes of hematuria against the background of preserved renal function. Subsequently, persistent microhematuria occurs. Kidney function usually does not change. As a rule, there is a family history of the disease. Kidney biopsy, which is not necessary if there is a family history, reveals thin basement membranes without signs of inflammation.
Alport syndrome
Alport syndrome is a rarer variant of familial glomerular pathology, manifested by hematuria, glomerulonephritis and bilateral sensorineural deafness. The disease is usually inherited in an X-linked dominant manner. As a rule, the syndrome manifests itself with massive hematuria in the first years of life, followed by microhematuria and proteinuria. Kidney pathology often develops to deafness.
Schistosomiasis
In African patients, the possibility of this disease should be kept in mind, especially if hematuria occurs at the end of urination. Eggs of Schistosoma haematobium are found in centrifuged urine.
Sickle cell anemia
People of African descent also have a higher prevalence of this disease, which is considered a risk factor for papillary necrosis. The screening test is positive if, during electrophoresis, 30-50% of hemoglobin is represented by the HbS form.
Diseases of the glomeruli of the kidneys
If erythrocyte or leukocyte casts are found in the urine in combination with altered erythrocytes, the likelihood of glomerular disease is extremely high.
The presence of protein further confirms this assumption. Renal dysfunction may occur. In some cases, if the process is suspected to be localized in the glomeruli and in the absence of a clear family history, a kidney biopsy is required to make a diagnosis.
In the absence of casts and altered red blood cells, cystoscopy and excretory urography with intravenous contrast are usually performed, however, in patients of European origin under 40 years of age, the cause of hematuria most often cannot be detected.
Tumors as causes of hematuria
Patients with hematuria over 40 years of age have a much higher risk of having a tumor detected. The most common is renal cell carcinoma, or hypernephroma. The tumor usually manifests as hematuria or groin pain. During examination, it is sometimes possible to palpate the tumor. Systemic manifestations include fever, hypercalcemia, and erythrocytosis. The diagnosis is confirmed by ultrasound examination of the kidneys.
Transitional cell carcinoma can develop from the renal medulla, along the ureter or in the bladder. The clinical picture of the disease typically begins with hematuria and pain, especially if the tumor obstructs the ureter. Bladder polyps often bleed. Prostate cancer can invade the ureter and cause bleeding.
In each case, the bleeding is fresh blood without casts or deformation of red blood cells and, usually, without significant proteinuria in the absence of massive bleeding. The examination plan must include ultrasound examination of the kidneys, cystoscopy, biopsy and, in some cases, intravenous urography.
Diagnostics
If macrohematuria is visible to the eye, then microhematuria can only be detected by microscopy of urine sediment. The study of cell structure indicates the level of possible damage to the urinary tract:
- with glomerulonephritis, leached forms of red blood cells are detected;
- at a lower level, the red blood cell wall does not undergo changes.
What does blood in urine mean in women?
Using a two-glass test, a practitioner can approximately determine the source of bleeding.
The patient needs to urinate into two containers without interruption. Approximately 1/3 of the urine is released into the first, and the remaining 2/3 into the second.
Decoding the sample divides the portions:
- to primary, hematuria in it is called “initial” - it is observed when the source of bleeding is in the damaged urethra (to be distinguished from urethrorrhagia in injuries, they are not associated with the act of urination, they occur involuntarily);
- in the first vessel there is no hematuria, but in the second portion there is - perhaps in the presence of damage to the posterior part of the urethra, bladder (cystitis, cancer), adenoma and prostate cancer, such hematuria is called “terminal”;
- there is an admixture of blood in both glasses - “total” hematuria indicates damage to the renal pelvis, calyces, and ureters.
Total hematuria often determines the unfavorable prognosis and method of treatment of the disease. It occurs with kidney tuberculosis, ulcerative cystitis, papillary necrosis, and urolithiasis.
The sample is used if it is not possible to quickly conduct other studies
The simultaneous presence of clots indicates the destruction of a large vessel. The shape of the clots varies:
- in renal or ureteral ones - worm-shaped;
- in the bladder - there is no typical shape, just “pieces”.
Laboratory tests confirm hematuria:
- special tests for erythrocyte hemoglobin;
- microscopy of urinary sediment;
- According to Nechiporenko’s method, red blood cells, casts and leukocytes are counted in 1 ml of urine; the number of red blood cells should not exceed 2 thousand cells.
For the purpose of differential diagnosis of hematuria and confirmation of its renal origin, the following is carried out:
- urine analysis (protein, casts, leukocytes, bacteria, salt crystals);
- biochemical blood tests (creatinine, electrolytes, alkaline phosphatase);
- immunological blood tests (for an increase in the content of IgA, cryoglobulins, antinuclear antibodies).
Phase contrast microscopy allows one to distinguish glomerular (glomerular) renal hematuria from non-glomerular hematuria.
The method helps in differential diagnosis:
- with glomerular - differences in shape and size are revealed in more than 80% of red blood cells (dysmorphism), their membranes are torn, the contours are uneven;
- with non-glomerular - on the contrary, more than 80% of erythrocyte cells have the same size and shape (isomorphism).
- mixed form possible.
Use instrumental methods:
- cystoscopy;
- Ultrasound of the kidneys and abdominal cavity, TRUS of the prostate gland in men;
- computed tomography and MRI of the abdominal cavity and pelvis;
- excretory urography;
- kidney biopsy.
Based on the results of a patient interview and primary tests, the attending physician prescribes the most indicated examination method. To decide the stage of the disease and choose a treatment method, it is necessary to identify not only the source of bleeding, but also its unilateral or bilateral origin, intensity, and degree of danger to the body.
Symptoms
There are no characteristic signs of hematuria; symptoms depend on the underlying disease. Localization of pain can help in diagnosing pathology.
Clinical picture:
- characteristic of urolithiasis, cystitis. Hematuria without other symptoms often indicates cancer;
- inflammatory, traumatic pathologies are accompanied by elongated blood clots in brown urine;
- inability to defecate, the appearance of blood instead of urine means blockage of the urethra;
- a yellowish or greenish tint to the skin that accompanies hematuria indicates problems with the liver/gallbladder;
- pain in the side, in the area of the shoulder blades may indicate traumatic damage to the organ;
- large clots of red blood cells are characteristic of bladder ailments; oblong clots are characteristic of kidney problems;
- the discharge of blood along with stones or sand indicates the progression of urolithiasis.
Why does hematuria occur in pregnant women?
Hematuria during pregnancy is provoked by the following reasons:
- diseases listed above, kidney injuries;
- altered hormonal levels;
- fetal growth, compression of the bladder in the third trimester, which contributes to the formation of stones;
- increased possibility of urinary tract infection due to impaired urine outflow.
Pregnancy causes disruption of the remission stage and activation of such chronic diseases as anemia, systemic lupus erythematosus, diabetes mellitus, and hemorrhagic diathesis. Observation and management of pregnancy in women with these diseases is carried out simultaneously by obstetricians and specialists in the field.