The mammalian kidney is structurally composed of two layers: the outer, cortical, and the underlying medulla, which contains the outer and inner parts.
The structural unit of the kidney is the nephron; there are about 1 million of them in the human kidney (a diagram of one of the nephrons is shown in Fig. 1). Each nephron begins with a double-walled Shumlyansky-Bowman capsule, inside which there is a glomerulus of capillaries - the glomerulus.
Between the walls of the capsule there is a cavity from which the proximal tubule (PT) begins. The part of the nephron next to the proximal tubule is the descending part of the loop of Henle; it ends with a hairpin-shaped elbow and then passes into the ascending part of the loop, located parallel to the descending one; then comes the distal tubule (DC), which returns to the capsule of its nephron and lies between the afferent and efferent arterioles, so that its border with the thick ascending loop of Henle (the area of the macula densa) is close to the afferent arteriole. Next, urine enters the collecting ducts (CT), which in transit pass through all layers of the kidney and are located parallel to the loops of Henle. Strictly speaking, CTs are not part of the nephron, since they have a different embryonic origin, but from a physiological point of view they are considered an integral part of the nephron.
Figure 1 Diagram of the structure of the nephron
Remember: the location of each part of the nephron in the kidney, as well as their relative position, is important for understanding their participation in the process of urine formation.
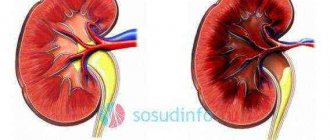
In the kidney of humans and mammals, there are several types of nephrons, differing in the location of the glomeruli: superficial, intracortical (lying inside the cortex) and juxtamedullary (their glomeruli are located at the border of the medulla cortex (Fig. 2). The difference between them lies in topography, loop length Henle and features of the blood supply. Thus, the juxtamedullary nephrons have a long loop of Henle, descending deep into the inner medulla. Due to these features, they will take part in the process of concentrating urine.
Figure 2 Types of nephrons
studopedia.ru
What is the structure of a nephron?
The structural unit of the kidney has a complex structure. It is noteworthy that each of its components performs a specific function.
- Malhypiean corpuscle of the kidney, consisting of a Shumlyansky-Bowman capsule with a diameter of 0.2 millimeters and a glomerulus of capillaries. The nephron begins from it. The cells surrounding the capillaries are arranged in such a way that they resemble a cap and are called renal corpuscles. It allows liquid to pass through, which is retained in the capsule. Infiltrate, which is a product of blood plasma filtration, also accumulates here. Bowman's capsule is a very important element of the nephron.
- Proximal convoluted tubule. Its feature is considered to be a brush border with villi that are turned inside the tubule. On the outside, the nephron section is covered with a basement membrane, collected in folds. When the kidney tubules become full, these folds straighten out and the tubules themselves become rounded. As the fluid exits, they narrow again, and the cells become prismatic. In the cytoplasm of tubule cells there are many mitochondria located on the basal side of the cell and providing it with energy to move various substances.
- Loop of Henle. After the proximal tubule has entered the medullary ray, it passes to the beginning of the loop of Henle, which descends into the medulla. But its upper part is attached to the cortex, connected to Bowman’s capsule. The loop is responsible for the reabsorption of water and ions into urea and is named after a famous pathologist from Germany.
The nephron is designed in such a way that the loop inside is initially no different from the proximal tubule. But a little lower, its lumen becomes narrower and acts as a filter for sodium entering the tissue fluid. After some time, this fluid turns into hypertonic fluid.
Next, the ascending segment expands and connects with the distal tubule.
- The distal tubule initially touches the capillary glomerulus in the place where the afferent and efferent arteries are located. This tubule is quite narrow, has no villi inside, and is covered with a folded basement membrane on the outside. It is in it that the process of reabsorption of Na and water and the secretion of hydrogen and ammonia ions occurs.
- The connecting tubule where urine enters from the distal portion and moves into the collecting duct.
- The collecting duct is considered the final part of the tubular system and is formed by an outgrowth of the ureter.
There are 3 types of tubules: cortical, outer medulla and inner medulla. In addition, experts note the presence of papillary ducts that empty into the small renal calyces. It is in the cortical and medullary parts of the tube that the process of formation of the final urine occurs.
Organ location
A healthy person has right and left kidneys. They are located on both sides of the spinal column. Normally, the upper border of the organ is adjacent to the 12th thoracic vertebra, and the lower border lies at the level of the 3rd lumbar vertebra. The left organ is located 2-3 cm above the right. The correct location of the kidneys in the human body is as follows:
- in women, the position of the organ is determined between Th11 and Th12 and below L3;
- in men - at the level of Th11 and above L3;
- the child's level is lower than usual.
The boundaries of the organ are individual, its apex can reach the upper edge of Th11, and the lower pole can descend by 1-½ vertebrae, which is not a pathology. The location of the kidney directly depends on the condition of the fat and muscle tissue around it, as well as its own fascia. Each kidney weighs up to 200 g.
The growth of a child’s body encourages the urinary system organ to strive upward towards Th12, but by the age of 10 it occupies a normal “adult” location. Until this time, the position of the child’s kidneys below is considered normal.
The kidneys have a rather complex structure, which is determined by the important functions they perform in human life.
Types of nephrons
Doctors distinguish 3 types of structural elements of the kidneys. It is worth describing each of them in more detail:
- Superficial or cortical nephron, which are kidney bodies located 1 millimeter from its capsule. They are distinguished by a shorter loop of Henle and make up about 80% of the total number of structural units.
- An intracortical nephron, the renal corpuscle of which is located in the middle part of the cortex. The loops of Henle are both long and short.
- Juxtamedullary nephron with renal corpuscle located at the top of the border of the cortex and medulla. This element has a long loop of Henle.
Due to the fact that nephrons are the structural and functional unit of the kidney and cleanse the body of waste products of substances entering it, a person lives without toxins and other harmful elements. If the nephron apparatus is damaged, this can provoke intoxication of the entire body, which threatens renal failure. This suggests that if there is the slightest malfunction in the kidneys, you should immediately seek qualified medical help.
What functions do nephrons perform?
The structure of the nephron is multifunctional: each individual nephron consists of functioning elements that work harmoniously and ensure the normal functioning of the kidney. The phenomena observed in the kidneys are conventionally divided into several stages:
Filtration. At the first stage, urine is formed in Shumlyansky’s capsule, which is filtered by blood plasma in the glomerulus of capillaries. This phenomenon occurs due to the difference between the pressure indicators inside the membrane and the capillary glomerulus.
The blood is filtered by a kind of membrane, after which it moves into the capsule. The composition of primary urine is almost identical to the composition of blood plasma, because it is rich in glucose, excess salts, creatinine, amino acids and several low molecular weight compounds. A certain amount of these inclusions is retained in the body, and some is excreted from it.
The structure of the nephron is multifunctional: each individual nephron consists of functioning elements that work harmoniously and ensure the normal functioning of the kidney. The phenomena observed in the kidneys are conventionally divided into several stages:
- Filtration. At the first stage, urine is formed in Shumlyansky’s capsule, which is filtered by blood plasma in the glomerulus of capillaries. This phenomenon occurs due to the difference between the pressure indicators inside the membrane and the capillary glomerulus.
The blood is filtered by a kind of membrane, after which it moves into the capsule. The composition of primary urine is almost identical to the composition of blood plasma, because it is rich in glucose, excess salts, creatinine, amino acids and several low molecular weight compounds. A certain amount of these inclusions is retained in the body, and some is excreted from it.
Taking into account how the nephron functions, it can be said that filtration occurs at a rate of 125 milliliters per minute. The pattern of its operation is never disrupted, which indicates the processing of 100 - 150 liters of primary urine every day.
- Reabsorption. At this stage, the primary urine is filtered again, which is necessary so that useful substances such as water, salt, glucose and amino acids return to the body. The main element here is the proximal tubule, the villi inside of which help to increase the volume and speed of absorption.
When primary urine flows through the tubule, almost all the liquid goes into the blood, resulting in no more than 2 liters of urine remaining.
All elements of the nephron structure take part in reabsorption, including the nephron capsule and the loop of Henle. Secondary urine does not contain substances needed by the body, but it can contain urea, uric acid and other toxic inclusions that need to be removed.
- Secretion. Hydrogen, potassium and ammonia ions contained in the blood appear in the urine. They may come from medications or other toxic compounds. Thanks to calcium secretion, the body gets rid of all these substances, and the acid-base balance is completely restored.
When urine passes the renal corpuscle, passes through filtration and processing, it collects in the renal pelvis, moves through the ureters to the bladder and is excreted from the body.
Features of the kidney filter
The nephron, the structure of which requires careful study by scientists seeking to recreate the kidney using modern technologies, carries a certain negative charge, which creates a limit on protein filtration. The size of the charge depends on the dimensions of the filter, and in fact the glomerular substance component itself depends on the quality of the basement membrane and epithelial coating.
The features of the barrier used as a filter can be implemented in a variety of variations; each nephron has individual parameters. If there are no disturbances in the functioning of the nephrons, then in the primary urine there will be only traces of proteins that are inherent in the blood plasma. Particularly large molecules can also penetrate through the pores, but in this case everything will depend on their parameters, as well as on the localization of the molecule and its contact with the forms that the pores take.
Nephrons are not able to regenerate, so if the kidneys are damaged or any diseases appear, their number gradually begins to decrease. The same thing happens naturally as the body begins to age. Nephron restoration is one of the most important tasks that biologists around the world are working on.
The kidneys carry out a large amount of useful functional work in the body, without which we cannot imagine our lives. The main one is the elimination of excess water and final metabolic products from the body. This happens in the smallest structures of the kidney - nephrons.
Preventive measures for nephron death
For the normal functioning of the body, a third of all the structural elements of the kidneys present in it is sufficient. The remaining particles are connected to work during increased load. An example of this is an operation during which one kidney was removed. This process involves placing the load on the remaining organ. In this case, all parts of the nephron that are in reserve become active and perform their required functions.
This mode of operation copes with the filtration of fluid and allows the body not to feel the absence of one kidney.
In order to prevent a dangerous phenomenon in which the nephron disappears, you should follow a few simple rules:
- Avoid or promptly treat diseases of the genitourinary system.
- Prevent the development of renal failure.
- Eat right and lead a healthy lifestyle.
- Seek medical help if you experience any alarming symptoms that indicate the development of a pathological process in the body.
- Observe basic rules of personal hygiene.
- Beware of sexually transmitted infections.
The functional unit of the kidney is not able to recover, so kidney disease, trauma and mechanical damage lead to the fact that the number of nephrons is reduced forever. This process explains the fact that modern scientists are trying to develop mechanisms that can restore nephron function and significantly improve kidney function.
Experts recommend not to neglect emerging diseases, because they are easier to prevent than to cure. Modern medicine has achieved great heights, so many diseases are successfully treated and do not leave serious complications.
pochki.guru
In the distal convoluted tubule
reabsorption of Na+ continues along with Cl− (Fig. 9-10 B).
Both of these ions from the lumen of the tubule enter the cells of the distal convoluted tubule through the mechanism of secondary active transport, causing the simultaneous transport of Na+ and Cl- (cotransport; carrier protein: TSC). NaCl enters the cell through the apical membrane through the Na+ and Cl- transporter localized on the luminal membrane (cotransport), while the Na+/K+ ATPase on the basolateral membrane actively removes Na+ from the cell, maintaining an electrochemical gradient that allows Na+ entry through the luminal membrane. This electrically neutral Na+-Cl— transporter is stimulated by aldosterone and inhibited by the diuretic thiacide. Therefore, it was named TSC (thiazid-sensitive co-transporter).
Cl— leaves the cell through Cl— channels (CLC-Kb type).
In the cortical collecting duct
(Fig. 9-10 D) Na+ enters the main cells through Na+ channels.
Rice. 9-10. Cellular models of Na+ reabsorption in different areas of the nephron.
A
- in the proximal convoluted tubule. B - in the distal straight tubule (thick ascending part of the loop of Henle). B - in the distal convoluted tubule. G — in the cortical communication tubule
Reabsorption of Cl— in various parts of the nephron
In the proximal convoluted tubule
Cl— is reabsorbed predominantly
intercellularly
(Fig. 9-11 A).
In the initial sections of the proximal tubule (S1), where the concentration of Cl— is 115 mmol, reabsorption of Cl— follows only water (the flow of water carries with it substances dissolved in it: transfer with the solvent
or
solvent drag).
As the filtrate moves through the tubules, despite the small reabsorption of Cl—, its concentration increases as water and Na+ leave the lumen of the tubule. Due to water reabsorption, the concentration of Cl- in the lumen of the tubule reaches 135 mmol, that is, it becomes greater than the concentration of Cl- in the interstitial fluid (for example, in the lumen of the proximal straight tubule). The difference in Cl− concentrations in the proximal tubule lumen compared with the Cl− concentrations in the interstitial fluid at each site of the tubule represents the driving force for the intercellular diffusion of Cl− from the tubule lumen toward the blood vessels. Thus, Cl— can leave the tubule lumen under the influence of a chemical driving force (∆[Cl—]): through tight junctions between the apical regions of the epithelial cell membrane (intercellular diffusion). In this way, part of the filtered Cl— is reabsorbed. As a result of this diffusion of Cl—, a transepithelial potential arises further along the proximal tubule, in which the fluid of the lumen of the tubule carries a positive charge (change in the sign of the potential), which in turn ensures the intercellular reabsorption of Na+, K+, Ca2+ and Mg2+ cations. The transepithelial potential is 2 mV.
vmede.org
The structural and functional unit of the kidney is the nephron, consisting of the vascular glomerulus, its capsule (renal corpuscle) and a system of tubules leading to the collecting ducts (Fig. 3). The latter morphologically do not belong to the nephron.
Figure 3. Diagram of the structure of the nephron (8).
Each human kidney has about 1 million nephrons; with age, their number gradually decreases. The glomeruli are located in the cortical layer of the kidney, 1/10-1/15 of them are located on the border with the medulla and are called juxtamedullary. They have long loops of Henle that extend into the medulla and help concentrate primary urine more efficiently. In infants, the glomeruli have a small diameter and their total filtering surface is much smaller than in adults.
The structure of the renal glomerulus
The glomerulus is covered with visceral epithelium (podocytes), which at the vascular pole of the glomerulus passes into the parietal epithelium of Bowman's capsule. Bowman's (urinary) space directly passes into the lumen of the proximal convoluted tubule. Blood enters the vascular pole of the glomerulus through the afferent (afferent) arteriole and, after passing through the capillary loops of the glomerulus, leaves it through the efferent (efferent) arteriole, which has a smaller lumen. Compression of the efferent arteriole increases hydrostatic pressure in the glomerulus, which promotes filtration. Within the glomerulus, the afferent arteriole is divided into several branches, which in turn give rise to the capillaries of several lobules (Fig. 4A). The glomerulus has about 50 capillary loops, between which anastomoses have been found that allow the glomerulus to function as a “dialysis system.” The glomerular capillary wall is a triple filter, including fenestrated endothelium, glomerular basement membrane, and slit diaphragms between the podocyte stalks (Fig. 4B).
A B
Figure 4. Structure of the glomerulus (9).
A – glomerulus, AA – afferent arteriole (electron microscopy).
B – diagram of the structure of the capillary loop of the glomerulus.
The passage of molecules through the filtration barrier depends on their size and electrical charge. Substances with a molecular weight >50,000 Yes are almost not filtered. Due to the negative charge in normal glomerular barrier structures, anions are retained to a greater extent than cations. Endothelial cells
have pores or fenestrae with a diameter of about 70 nm.
The pores are surrounded by glycoproteins that have a negative charge; they represent a kind of sieve through which ultrafiltration of plasma occurs, but the formed elements of the blood are retained. The glomerular basement membrane
(GBM) represents a continuous barrier between the blood and the capsule cavity, and in an adult it has a thickness of 300-390 nm (in children it is thinner - 150-250 nm) (Fig. 5). GBM also contains a large number of negatively charged glycoproteins. It consists of three layers: a) lamina rara externa; b) lamina densa and c) lamina rara interna. An important structural part of the GBM is type IV collagen. In children with hereditary nephritis, clinically manifested by hematuria, type IV collagen mutations are detected. The pathology of GBM is established by electron microscopic examination of a kidney biopsy.
Figure 5. The glomerular capillary wall is the glomerular filter (9).
Below is the fenestrated endothelium, above it is the GBM, on which regularly spaced podocyte stalks are clearly visible (electron microscopy).
Visceral epithelial cells of the glomerulus
, podocytes, maintain the architecture of the glomerulus, prevent the passage of protein into the urinary space, and also synthesize GBM. These are highly specialized cells of mesenchymal origin. Long primary processes (trabeculae) extend from the podocyte body, the ends of which have “legs” attached to the GBM. Small processes (pedicles) extend from the large ones almost perpendicularly and cover the space of the capillary free from the large processes (Fig. 6A). A filtration membrane, the slit diaphragm, is stretched between adjacent podocyte stalks, which has been the subject of numerous studies in recent decades (Fig. 6B).
A
B
Figure 6. Structure of a podocyte (9).
A – podocyte feet completely cover the GBM (electron microscopy).
B – diagram of the filtration barrier.
Slit diaphragms consist of the nephrin protein, which is closely related in structural and functional relationships to many other protein molecules: podocin, CD2AR, alpha-actinin-4, etc. Mutations of the genes encoding podocyte proteins have now been identified. For example, a defect in the NPHS1 gene leads to the absence of nephrin, which occurs in congenital nephrotic syndrome of the Finnish type. Damage to podocytes due to exposure to viral infections, toxins, immunological factors, and genetic mutations can lead to proteinuria and the development of nephrotic syndrome, the morphological equivalent of which, regardless of the cause, is the melting of the podocyte feet. The most common type of nephrotic syndrome in children is idiopathic minimal change nephrotic syndrome.
The glomerulus also includes mesangial cells, the main function of which is to provide mechanical fixation of capillary loops. Mesangial cells have contractility, influencing glomerular blood flow, as well as phagocytic activity (Fig. 4B).
Kidney tubules
Primary urine enters the proximal renal tubules and undergoes qualitative and quantitative changes there due to the secretion and reabsorption of substances. Proximal tubules
- the longest segment of the nephron, at the beginning it is strongly curved, and when passing into the loop of Henle it straightens.
The cells of the proximal tubule (a continuation of the parietal epithelium of the glomerular capsule) are cylindrical in shape, covered with microvilli (“brush border”) on the lumen side. Microvilli increase the working surface of epithelial cells, which have high enzymatic activity. They contain many mitochondria, ribosomes and lysosomes. Active reabsorption of many substances (glucose, amino acids, sodium ions, potassium, calcium and phosphates) occurs here. Approximately 180 L of glomerular ultrafiltrate enters the proximal tubules, and 65-80% of water and sodium are reabsorbed. Thus, as a result of this, the volume of primary urine is significantly reduced without changing its concentration. Loop of Henle.
The straight part of the proximal tubule passes into the descending limb of the loop of Henle.
The shape of epithelial cells becomes less elongated, and the number of microvilli decreases. The ascending section of the loop has a thin and thick part and ends in a dense spot. The cells of the walls of the thick segments of the loop of Henle are large and contain many mitochondria, which generate energy for the active transport of sodium and chlorine ions. The main ion transporter of these cells, NKCC2, is inhibited by furosemide. The juxtaglomerular apparatus (JGA)
includes 3 types of cells: cells of the distal tubular epithelium on the side adjacent to the glomerulus (macula densa), extraglomerular mesangial cells and granular cells in the walls of afferent arterioles that produce renin. (Fig. 7).
Distal tubule.
Behind the dense spot (macula densa), the distal tubule begins, which passes into the collecting duct.
About 5% Na of primary urine is absorbed in the distal tubules. The transporter is inhibited by diuretics from the thiazide group. The collecting ducts
have three sections: cortical, external and internal medullary. The internal medullary portions of the collecting duct empty into the papillary duct, which opens into the minor calyx. The collecting ducts contain two types of cells: main ("light") and intercalary ("dark"). As the cortical part of the tube transitions to the medullary part, the number of intercalary cells decreases. The main cells contain sodium channels, the work of which is inhibited by the diuretics amiloride and triamterene. Intercalary cells do not have Na+/K+-ATPase, but contain H+-ATPase. They carry out the secretion of H+ and the reabsorption of Cl-. Thus, the final stage of NaCl reabsorption occurs in the collecting ducts before urine exits the kidneys.
Interstitial cells of the kidneys.
In the renal cortex, the interstitium is weakly expressed, while in the medulla it is more noticeable. The renal cortex contains two types of interstitial cells - phagocytic and fibroblast-like. Fibroblast-like interstitial cells produce erythropoietin. There are three types of cells in the kidney medulla. The cytoplasm of one of these types of cells contains small lipid cells that serve as the starting material for the synthesis of prostaglandins.
biofile.ru
Kidney diseases
Pathologies of the kidneys and urinary system are more common in women. This is due to physiological characteristics. A short and wide urethra is more likely to become a target for pathogenic microorganisms. The situation is aggravated by the close location of the rectum, which is home to many microbes. In this regard, in men, pathology of the kidneys and bladder is detected less frequently.
Speaking about what types of kidney diseases there are and which possible pathologies of the urinary system are recorded more often, it is necessary to note the following diseases:
- Urolithiasis is the result of a metabolic disorder in the body, in which the formation of stones from salt crystals is observed.
- Nephroptosis – prolapse of the kidneys.
- Kidney failure is a violation of the functional capacity of an organ.
- Pyelonephritis is inflammation of the kidneys.
- Hydronephrosis.
- Renal colic.
Symptoms of kidney disease
Congenital kidney diseases and developmental anomalies are in most cases discovered during a random examination. Often, parents cannot understand why the baby is restless and often capricious. The first signs of possible pathology in such cases are a change in the nature and volume of urine excreted. Darkening, increase or decrease in the volume of urine, the appearance of an unpleasant odor, flakes or blood always indicates problems with the kidneys.
Other possible symptoms of kidney disease include:
- increased body temperature;
- increased blood pressure;
- swelling of the lower extremities;
- puffiness of the face;
- discomfort and pain in the area of the projection of the kidneys (right and left);
- nausea, vomiting;
- decreased appetite;
- increased fatigue;
- the appearance of skin rashes.
How to determine kidney pain?
Most patients do not know how to recognize kidney pain. Many people confuse it with the phenomena of rheumatism or osteochondrosis of the lumbar spine. With these pathologies, pain is also localized in the lumbar region, but there are no additional symptoms described above.
In addition, there are differences in the nature of the pain:
- With kidney pathology, the pain is aching, dull (with inflammation) or sharp (with renal colic).
- After changing body position, the pain does not disappear or intensify, as is the case with diseases of the musculoskeletal system.
Hardware diagnostics help determine that painful sensations are caused by kidney pathology:
- Ultrasound of the kidneys;
- endoscopy;
- X-ray with contrast agent.