Emergency medicine
Physiology of the hypothalamus. The hypothalamus is part of the hypothalamus-pituitary-adrenal system; where it plays the role of a higher subcortical endocrine regulator. The mediator in the performance of this function is neurosecretion - the release of factors that stimulate the function of the pituitary gland. These substances were discovered by R. Guillemin and E. Shelley and were initially called releasing factors, i.e. releasing, disinhibiting the hormonal function of the pituitary gland. It is now known that the hypothalamus produces both neuropeptides that enhance and inhibit the function of the pituitary gland (liberins and statins). In particular, somatostatin inhibits the production of growth hormone, and somatoliberin stimulates its formation by the pituitary gland. This occurs due to the enhancement or inhibition of the formation of cyclic AMP in the cells of the pituitary gland. Statins inhibit the formation of c-AMP and reduce the content of free Ca2+ cations in pituitary cells. As a result, the biosynthesis of growth hormone and its release from pituitary cells is reduced.
The hypothalamus produces factors that stimulate the formation of pituitary tropic hormones.
Physiology of the pituitary gland. The pituitary gland is connected to the gray tubercle and the anterior nuclei of the hypothalamus (supraoptic and paraventricular) through the infundibulum and the stalk, which determines its close morphofunctional connection with the highest subcortical regulator of endocrine function.
The pituitary gland consists of glandular and nervous tissue. In embryogenesis, glandular tissues develop from the fold on the wall of the oral cavity - the anterior and intermediate lobes (adenohypophysis). The second part of the pituitary gland, the neurohypophysis, consists of nervous tissue. The anterior lobe of the pituitary gland is connected to the hypothalamus by a network of blood vessels through which releasing (disinhibiting the function of the anterior lobe) or inhibitory factors of the hypothalamus enter. In the posterior lobe of the pituitary gland, the axons of the nerve cells of the hypothalamus that produce hormones end.
The anterior lobe of the pituitary gland produces growth hormone - somatotropin and a group of tropic hormones that provide a triggering effect on the adrenal gland, gonads, and thyroid gland. Somatotropin stimulates the biosynthesis of proteins in the cells and tissues of a growing organism (increases RNA synthesis, enhances the transport of amino acids from the blood to the cells and tissues of the body).
Indirectly, through somatomedin hormones, somatotronin increases the permeability of cell membranes to nutrients and biologically active substances. Consequently, metabolism as a whole is associated with the secretion of somatotropin, and disruption of its function leads to extremely complex changes in both the growing and mature organism.
Increased production of somatotropin in childhood and adolescence leads to gigantism. With the artificial administration of growth hormone to children suffering from insufficiency of pituitary gland function, their height increased during 6 months of treatment by 5-6 cm. With hyperfunction of the pituitary gland, the height of people, as a rule, exceeds 2 m (Fig. 90). It is known that the Roman Emperor Maximilian had a height of 2.5 m, and the Russian godfather Makhnov - 2.85 m. Among women, the Swiss woman Ama had the greatest height - 2.35 m. The tallest person in the world described in literature had a height of 3 ,20 m.
Gigantism, as a rule, is accompanied by acromegaly - the growth of the bones of the face, hands and feet (Fig. 91). Hypofunction of the anterior pituitary gland leads to growth retardation. Patients in this case have a height from several tens of centimeters to 1 m (pituitary dwarfs). The Egyptian dwarf Agibe was 38 cm tall.
The anterior lobe of the pituitary gland secretes a group of triple hormones. A group of gonadotropic hormones (follicle-stimulating hormone, luteinizing hormone, prolactin) stimulate the formative and sectoral functions of the gonads.
The follicle-stimulating hormone of the pituitary gland causes cyclicity in the maturation of female germ cells and the formation of follicles. In men, this hormone enhances spermatogenesis. Under its influence, spermatogenic tissue grows and sperm development is enhanced.
Luteinizing hormone in women regulates ovulation and the formation of the corpus luteum. In men, it acts as a regulator of the production of sex hormones - androgens. Prolactin stimulates lactation in women, as well as the development of the corpus luteum of pregnancy.
Thyrotropic hormone thyrotropin increases the production of thyroid hormones. It affects the growth of glandular epithelium and enhances its secretion.
Adrenocorticotropic hormone (ACTH causes increased biosynthesis of hormones of the zona fasciculata and zona reticularis of the adrenal cortex. ACTH production increases under the influence of stressful stimuli. In the practice of physical education, these are competitive and high training loads, as well as pre-start excitement associated with performances in competitions. In the physiological mechanisms of stimulating effects physical activity, an important place is occupied by an increase in the production of adrenaline under the influence of stress stimuli.Adrenaline acts on the nuclei of the hypothalamus, which produce ACTH - a releasing factor.
Hormones of the anterior pituitary gland have a nonspecific effect on metabolism, acting as regulators of protein, fat and carbohydrate metabolism. Extracts from the tissues of the anterior pituitary gland enhance the synthesis of glycogen from fats and proteins and accelerate the deamination of proteins by the liver.
, enter the posterior lobe of the pituitary gland (neurohypophysis) through the long processes of the nerve cells of the hypothalamus. Vasopressin is also called antidiuretic hormone (ADH). It enhances the reabsorption of water in the distal renal tubules and collecting ducts, increasing their permeability to water. With hypofunction of the posterior lobe of the pituitary gland, diabetes insipidus develops. The patient's daily diuresis reaches several tens of liters. The side effect of ADH is an increase in blood pressure.
Oxytocin has different effects on the uterus at different stages of pregnancy. At the beginning of pregnancy, the uterus is insensitive to oxytocin. By the time labor occurs, the sensitivity of the uterus to oxytocin increases. This is due to the extinction of the hormonal function of the corpus luteum. Labor activity increases under the influence of oxytocin.
The middle (intermediate) lobe of the pituitary gland secretes melanophore (pigment-stimulating) intermedia hormone. Its effect is manifested in enhancing the pigment-forming function of the skin.
Physiology of the adrenal glands. In 1855, the English physician Addison first described a patient suffering from bronze disease. This disease, later called Addison's disease, is the result of atrophic changes in both adrenal glands. Atrophy of the adrenal glands is accompanied by chronic insufficiency of the function of their cortical layer. Adcison's disease is characterized by a general metabolic disorder, lack of appetite, nausea, vomiting, and abdominal pain. The patient's weight quickly decreases, exhaustion sets in, and dark spots appear on the mucous membranes of the lips and gums. The skin of the face and exposed parts of the body takes on the color of old bronze.
The adrenal glands play the role of the most important regulator of the complex relationships between the body and the environment in stressful situations. The stress response, manifested in a sharp increase in energy production and stimulation of human physical performance, is closely related to the strengthening of the hormonal function of the adrenal glands.
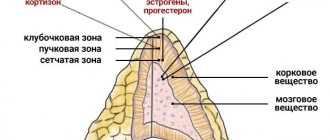
The adrenal glands consist of a cortex and medulla. The cortex, in turn, has three zones: the inner - reticular, the middle - fascicular and the outer - glomerular. The reticular zone produces sex hormones: androgens, estrogens, progesterone. The zona fasciculata produces glucocorticoids (cortisone, hydrocortisone). The external (glomerular) zone produces mineralocorticoids (aldosterone, etc.).
The reticular lobe of the adrenal glands is a source of sex hormones in childhood, when the intrasecretory function of the gonads is practically absent. At the end of life, after the onset of menopause, the zona reticularis of the adrenal glands remains the only place where sex hormones are formed.
Glucocorticoids (cortisone, corticosterone, dehydrocorticosterone) regulate carbohydrate metabolism, especially its intermediate stages. Cortisone regulates the formation of glycogen, delays the breakdown of carbohydrates and their conversion into fat. Corticosterone and dehydrocorticosterone increase blood sugar levels. Cortical steroid hormones stimulate physical performance and reduce skeletal muscle fatigue. Cortisone has high anti-inflammatory activity and can be successfully used in the treatment of certain types of inflammation.
Mineralocorticoids regulate water and mineral metabolism. Thus, aldosterone increases the reabsorption of Na+ and the excretion of K+ in the urine. Aldosterone also has an antidiuretic effect. Reabsorption of Na+ leads to an increase in its concentration in the capillaries of the renal tissue and interstitial fluid of the renal medulla. This leads to increased reabsorption of water from the renal canals and collecting ducts. The amount of definitive (final) urine decreases.
The common precursor of corticoid and sex hormones is cholesterol. Hormones of the adrenal medulla (adrenaline and norepinephrine) have a pronounced stimulating effect on muscle performance. It is supported by the mobilization of liver and muscle glycogen, activation of the functions of the cardiovascular and respiratory systems. Increased secretion of adrenaline and norepinephrine stimulates the synthesis of steroid hormones.
Fomin A.F. Human physiology, 1995
basic information
Under the influence of certain factors, the amount of hormones produced by the adrenal glands can be significantly reduced, causing serious harm to human health.
Pathology can affect all hormones at once or only one specific substance. There are two forms of adrenal hypofunction:
- Acute (Addisonian crisis). Characterized by a sudden cessation of hormone production, for example, under the influence of severe infections.
- Chronic (Addison's disease). It can last for years, worsening after illness, prolonged stress or injury.
Also, depending on the location of the root cause of the pathology, it is usually divided into:
- Primary (occurs in 90% of all cases). It develops as a result of damage to the adrenal glands themselves.
- Secondary . A malfunction occurs as a consequence of problems with the pituitary gland, under the influence of which the level of ACTH, or adrenocorticotropic hormone, which is responsible for stimulating the activity of the adrenal glands, sharply drops.
- Tertiary . The pathology is based on disturbances in the functioning of the hypothalamus, which stops sending the pituitary gland the signals necessary to regulate the functioning of the adrenal glands.
It is also customary to classify drug-induced, or iatrogenic, deficiency as a separate form, which develops after abrupt discontinuation of long-term hormonal therapy, but it is quite rare, in only 4-11 cases per 100 thousand patients.
Etiology of the disease
In almost 98% of cases, decreased adrenal activity is a consequence of autoimmune diseases, in which antibodies attack organ tissue.
Other causes of primary hypocortisolism are much less common:
- infectious diseases of the adrenal glands, primarily tuberculosis;
- congenital pathologies;
- malignant neoplasms and metastases;
- complications after surgery;
- irreversible tissue damage due to HIV infection, etc.
The development of secondary or tertiary hypofunction can be provoked by:
- disturbances in the functioning of the endocrine system;
- hemorrhages in the adrenal glands as a result of injuries;
- brain tumors;
- congenital anomalies of the pituitary gland and hypothalamus.
In addition, Addisonian crises may be based on severe infectious diseases, for example, herpes or diphtheria, thrombosis, adrenal cancer, and even sudden drug withdrawal syndrome. And in children under 3 years of age, a common cold or severe stress can reduce the activity of the adrenal glands.
Diagnostic methods
To make a correct diagnosis, patients with suspected adrenal hypofunction are prescribed a number of tests and examinations, among which the most revealing is determining the level of cortisol and aldosterone in the blood. In addition, a general blood test is performed to identify metabolic disorders, a diagnosis of ACTH levels in the blood, and a urine test to determine the amount of cortisol metabolites. In addition, an important part of the diagnosis is ultrasound of the adrenal glands, as well as CT and MRI of the brain.
This approach allows you to find out the true cause of hypofunction and select treatment aimed at eliminating it.
In addition, immunological tests are taken from patients to identify possible autoimmune diseases, the likelihood of tuberculosis is assessed, and an ECG of the heart is prescribed to determine whether problems with the adrenal glands have affected its functioning.
Location in the brain
Now let's discuss where exactly these structures are located in the brain - the pituitary gland, hypothalamus, pineal gland. The pituitary gland is located at the base of the brain, down in a bony pocket called the sella turcica. It is located close to the spinal cord. Through its ducts, all substances produced by the hypothalamic-pituitary system enter the body.
Hypothalamus - hypothalamus, from Greek. department or room. It is part of the intermediate section of the brain and is the main regulator of nervous processes. It is located under the optic thalamus, behind the midbrain.
Table. Pituitary hormones
| Full name of the hormone | Abbreviated name for hormone |
| Tropic hormones | |
| Follicle stimulating hormone | FSH |
| Luteinizing hormone | LH |
| Thyroid-stimulating hormone | TSH |
| Adrenocorticotropic hormone | ACTH |
| Effector hormones | |
| Growth hormone, somatotropic hormone | GR, STG |
| Prolactin (luteotropic hormone) | BPD (LTG) |
| Melanocyte-stimulating hormone | MSG |
When the pituitary gland is removed, symptoms of hormonal deficiency develop in the body, since the hormones of the adenohypophysis in this case do not have a stimulating effect on a number of endocrine glands and functions.
Methods of therapeutic therapy
Stabilizing a patient’s condition with chronic sluggish hypocortisolism first of all involves prescribing replacement therapy, which, by taking synthetic drugs, makes it possible to bring the amount of hormones produced by the adrenal glands closer to the required level.
The treatment regimen is always selected individually, depending on the degree of development of hypofunction in the adrenal glands and the general well-being of the patient.
Thus, at the initial stage of the disease, taking cortisone alone may be sufficient, but with a significant decrease in the activity of the adrenal glands, it is necessary to use a whole complex of hormonal drugs.
At the same time, attention is paid to those pathological factors that provoked the development of hypofunction, for example, treatment of infectious diseases or surgical removal of tumors is carried out.
In the acute form of the disease, the patient requires immediate hospitalization with further intensive treatment - intravenous administration of hormones and anti-shock therapy.
In addition, patients with adrenal hypofunction are recommended to adhere to a diet throughout their lives, paying special attention to foods with a high content of proteins and fatty acids, avoid stress, excessive physical activity, control weight and blood pressure, maintaining it at the required level.
Sphere of influence
The endocrine system is a coherent structure that supplies the body with the amount of hormones required to maintain life. The following are directly involved in the production of biologically active substances:
- thyroid;
- adrenal glands;
- ovaries;
- epithelial body;
- testes and testes;
- hypothalamus;
- pancreas.
The pituitary gland is at the head of this list. It is this small formation, weighing no more than 0.6 g and with a pituitary stalk, that is responsible for the production of hormones in the quantities needed by the body. Numerous anterior pituitary hormones have a direct effect on human behavior and appearance. They affect the physical ability to feel comfortable every day.
What the pituitary gland is responsible for is of interest to many.