Each stage of kidney cancer —the development of a malignant neoplasm—has its own characteristics. In modern medicine, the TNM classification is adopted, where T is the presence of the tumor itself, N is damage to the lymph nodes, M is the appearance of metastases.
The outcome of a disease such as kidney cancer is influenced by a very large number of different clinical factors. Of course, the best prognosis will always be for a patient whose tumor does not extend beyond the kidney. Since even minimal spread and invasion into neighboring organs is significantly more dangerous than a tumor. When the tumor spreads beyond Gerota's capsule, the risk of a negative outcome increases by more than 25%. The prognosis is even more negative for lesions of the inferior vena cava and renal vein. In these cases, two-year survival rate drops by another 40%.
This leads to the fact that people go to the doctor in serious condition, in the last stages of kidney cancer, when even radical surgery does not guarantee a high survival rate. Relapses and metastases to other organs are also likely.
Classification
There are several types of classification that are included in the diagnosis and are the main marker when choosing treatment methods. One type of classification is based on the study of cells from puncture or surgical material of the kidney. Depending on which cells initiated the growth of a cancerous tumor, the following are distinguished:
- Clear cell kidney cancer. It ranks first in frequency of occurrence among kidney cancers, the frequency is up to 85% of cases. Formed from atypical cells lining the proximal tubules of the nephron.
- Chromophobic cancer. The cancer grows from cells located in the collecting ducts, a rare form of cancer, diagnosis is possible in the early stages before metastasis.
- Chromophilic cancer. The development of pathology occurs from the cortical layer of the collecting system of the kidney.
- Papillary cancer. Carcinoma has spread to the pelvicalyceal apparatus. Aggressive course with rapid spread of metastases to internal organs.
- Undifferentiated kidney cancer. The most rapidly progressing and aggressive malignant kidney cancer is characterized by the fourth stage.
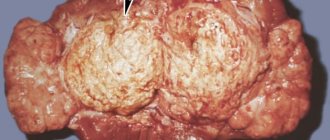
This is what kidney cancer looks like
Carcinomatosis of the excretory system, like all oncological nosologies, is divided into four stages of kidney cancer according to its activity:
- Stage I. It is characterized by a tumor up to 5 cm in size, which does not extend beyond the organ, without screening out metastases. The most favorable prognosis, but is rarely diagnosed due to the paucity of symptoms.
- Stage II. It is characterized by carcinoma exceeding 5 cm, but not more than 10 cm, which already affects the kidney capsule and does not metastasize.
- Stage III. It is a tumor more than 10 cm, which grows into adjacent organs and tissues, metastasizing to the lymph nodes through the lymphogenous route. A clear clinical picture allows you to quickly diagnose the pathology.
- Stage IV. The most unfavorable option for prognosis is undifferentiated cytosis in the histogram of punctate or postoperative material. Rapid growth, multiple metastasis by hematogenous and lymphogenous routes.
Epithelial origin. Adenoma
An adenoma is a solid formation of unknown origin. This neoplasia is the most common among all non-cancerous formations of renal tissue. It has a slow growth rate and is not invasive. There are no symptoms until the tumor reaches a large size. Then it begins to put pressure on the parenchyma of the organ, disrupting its functionality. Adenoma can be solid, cystic, papillary, tubular, mixed.
This benign kidney tumor requires timely diagnosis. Many experts are of the same opinion that an adenoma can be a precancerous condition, which means it must be treated immediately. Even in its histological structure, the adenoma is similar to low-grade squamous cell carcinoma. Most often, surgical diagnosis is performed to obtain a sample of the tumor. Diagnosis is also carried out using computed tomography and x-ray examination. However, using the last two methods, you can only obtain general information about the status of neoplasia.
Even if histological examination indicates that it is a benign kidney tumor, one cannot limit oneself to observing the dynamics of growth. Any delay can be dangerous to the patient's health. The adenoma is subject to surgical removal, possibly accompanied by hormone therapy. The prognosis is positive in almost all cases.
Clinical manifestations
Manifestations of kidney cancer in the early stages are nonspecific. In the first and second stages, there may be a slight deterioration in general well-being: increased fatigue, drowsiness, appetite decreases slightly, and the person loses weight. In the initial stages, the following symptoms of kidney cancer are possible:
- pain in the lumbar region;
- hyperhidrosis (increased sweating);
- chronic fatigue and the manifestation of other nonspecific markers.
At later stages - the third and fourth stages - the main signs of kidney cancer appear:
- Hematuria. The appearance of blood in the urine is the most important clinical landmark, which makes the patient alert and consult a doctor. Blood discharge occurs in the form of clots and may be accompanied by hepatic colic. In women, this clinical criterion is less informative than in men. So, in women, according to statistics, cancer is detected more often at later stages.
- Pain syndrome. It manifests itself as pronounced spasms in the lumbar region, simulating urolithiasis, but sometimes the pain is a constant pulling or pressing encircling character in the area of the right or left kidney. May radiate to the thigh on the affected side.
- Volumetric education. It is most often found in kidney cancer in children (Williams cancer is a malignant tumor of the kidney). The formation is most often lumpy on palpation, dense, can bulge, but more often it is motionless, rarely painful. There is asymmetry of the abdomen, most often the process is unilateral, but even with bilateral damage, asymmetry is observed due to uneven growth.
- Cachexia. A cancer patient quickly loses weight due to a sharp decrease in appetite.
- Intoxication syndrome. Increased body temperature, weakness, accompanied by drowsiness, apathy, chronic fatigue syndrome. The fourth stage is characterized by necrosis and severe inflammatory processes in the affected organ due to a decrease in the reactive properties of the body, infection occurs.
- Inferior vena cava compression syndrome. A volumetric formation in the retroperitoneal region can block the outflow of blood through the inferior vena cava, which leads to severe swelling in the legs and provokes the development of varicose veins in women and varicocele in men. It is possible to develop thrombosis in the lower extremities, often deep; upon palpation, an increase in parenchymal organs is observed: liver, spleen. On the anterior abdominal wall, a “jellyfish head” may be observed - dilated veins of the anterior abdominal wall protruding above the surface of the skin.
Causes
Predisposing risk factors:
- Heredity. The likelihood of getting sick doubles when parents are diagnosed.
- Floor. In men, pathology occurs 1.5 times more often than in women.
- Von Hipel-Lindau syndrome. This is a hereditary disease in which, in addition to various disorders of embryogenesis, there is also a genetic predisposition to RCC.
- Smoking (renal cell cancer is 1.5 times more common in smokers).
- Obesity. The risk increases by 20%.
- Condition after removal of the uterus. Women who have a hysterectomy are twice as likely to develop kidney cancer.
- Chronic hemodialysis in patients with chronic renal failure.
- Arterial hypertension. The likelihood of developing RCC increases by 20%.
- Long-term use of diuretics and analgesics. The risk is increased by approximately 30%.
- Contact with cyclic hydrocarbons, asbestos.
Diagnostic methods
Based on clinical data, a thorough history of the disease, life history and hereditary predisposition, additional research methods are prescribed to confirm or refute the preliminary diagnosis of kidney oncology:
- Clinical blood test. Nonspecific study, possible registration of anemia, slight lymphocytosis, significant increase in ESR.
- General urine analysis. Macrohematuria, macroproteinuria, leukocyturia, cylindruria.
- Ultrasound of the kidneys and bladder. Detection of space-occupying formations in the retroperitoneal space; it is possible to detect oncological nodes at an early stage.
- CT or MRI. It is carried out not only in the area of the abdominal organs. A tomography of the chest organs is recommended to exclude metastatic lesions.
- Renal angiography. The method is necessary for visualizing the blood supply to the tumor process.
- Excretory urography. Allows you to visualize a volumetric formation.
- Biochemical parameters. Renal parameters (urea, creatinine, glomerular filtration rate) reveal the degree of functional impairment of the kidney, chronic renal failure.
- Needle biopsy. An invasive method for diagnosing the histological structure of carcinoma, carried out under ultrasound control.
Mesenchymal origin. Lipoma
Benign tumors in the kidneys, such as lipomas, can reach 25 cm in length, while the neoplasia retains its shape and clear contours. Lipoma consists of fibrous material of the renal parenchyma, contains fat cells, a large number of vessels separated by fibrous septa. It grows slowly. As it grows, it compresses the parenchyma, blood vessels, and urinary tract. In this case, surgical treatment is indicated. The presence of a lipoma with no symptoms cannot be treated and does not pose a threat to life. The prognosis is always positive.
Treatment methods
Recently, progressive methods have been developed for the treatment of kidney cancer; the most effective regimens are selected individually, depending on the stage and type of cancer pathology. Most often, therapy is carried out by a combination of several types of therapeutic measures:
- Surgery;
- Chemotherapy treatment;
- Immunological treatment;
- Hormonal therapy;
- Targeted therapy for kidney cancer;
- Radioisotope radiation therapy, etc.
Surgery
Today it remains the most effective therapeutic method. At the first and second stages, radical operations are performed:
- Kidney resection for stage 1 cancer (partial removal);
- Removal of a kidney for stage 2–3 cancer with revision and excision of regional lymph nodes;
Palliative intervention at the fourth stage is carried out to reduce symptoms of urinary tract obstruction and compression of nearby organs, to prolong the patient’s life.
The prognosis after removal of kidney cancer at the first - second stages is relatively favorable: the first stage survival rate is about 90% of patients, the second - up to 70%. In parallel, chemotherapy, radiation therapy or other innovative treatment methods are carried out according to indications, which allow patients with cancer to live.
Of course, with stage 4 kidney cancer, how long patients live is impossible to predict; the five-year survival rate is no more than 4%. The main task of medicine in this case is to improve their quality of life as much as possible.
Chemotherapy treatment
Chemotherapy is based on the use of drugs that can suppress the growth of atypical cells, reduce the blood supply to the cancerous tumor (the drug Nexvar - used in palliative therapy to prevent the appearance of new vessels that feed kidney cancer) and other drugs.
It is recommended to carry out several courses, depending on the stage and histological structure of the tumor. In fact, chemotherapy drugs are not able to cure cancer, but are used to reduce the volume of the tumor. This method is often performed before surgery. After surgery, chemotherapeutic cytostatic drugs are prescribed to prevent recurrence of tumor growth.
Polychemotherapy is carried out during palliative treatment at the terminal stage to reduce the volume of formation and alleviate the patient's condition.
Radiation therapy
It is carried out as palliative treatment to reduce pain, thereby improving the quality of life.
Widely used for metastasis of cancer cells to bones, it causes a reduction in the volume of metastases, reduces pain and reduces the risk of developing many possible complications. It is carried out in courses of 7-14 days, the dose is calculated individually.
Often, to reduce the volume of a malignant neoplasm, a preoperative course of radiation therapy is performed. In this case, surgery must be performed within the next 48 hours.
Features of the disease
A benign kidney tumor is not a fatal disease and can be successfully treated, no matter what size it reaches. It grows slowly and does not have the ability to grow into surrounding tissues. However, being relatively asymptomatic, this neoplasm can exert significant pressure on the blood vessels, renal parenchyma, and urinary ducts. At the same time, the patient's condition deteriorates sharply and requires treatment using surgical methods.
Features of this neoplasia of renal tissue:
- the prognosis is positive;
- growth is slow;
- no metastasis;
- no ability to germinate into tissue;
- the functions of the paired organ are not impaired when the tumor is small;
- The patient's life is not in danger.
However, the possibility of degeneration into a malignant form should never be ruled out. That is why any neoplasm, even one that is safe for human life, must be strictly monitored by specialists.
Risk factors
It is impossible to accurately determine the reason why a particular cancer occurs. Doctors have only been able to identify a few risk factors that presumably cause renal cell carcinoma.
These include smoking, excess body weight and arterial hypertension. Heredity plays an important role in the occurrence of renal cell cancer.
It is necessary to warn about the increased risk of kidney cancer in patients who undergo hemodialysis for a long time. One of the side effects of this procedure is the formation of cysts, which can later degenerate into malignant formations.
Poor diet and exposure to carcinogens do not in any way increase the risk of developing renal cell carcinoma. Paradoxically, a small amount of alcohol consumption is a preventive measure in this case.
General information about the disease
Oncocytomas develop more often in men, but the reliable causes of their occurrence are not yet known to medicine. Perhaps the hereditary tendency of the genetic material of cells to mutations is important.
The morphological picture of the disease resembles the initial stages of malignant dysplasia (degeneration) of the kidneys, so some experts classify oncocytomas as precancerous (obligate) diseases. The difference between this disease and malignant cancer is that oncocytomas do not grow into nearby tissues and do not cause their pathogenic transformation.
For a long time from the moment of its occurrence, oncocytoma may not give any pronounced symptoms . Often a tumor is discovered completely by accident - during an examination of the abdominal cavity for another reason or during a routine ultrasound.
Fibroma
Can occur in single and multiple forms.
bromine consists of dense fibrous material (collagen), fibrocytes, fibroblasts, and blood vessels. Can reach 2 cm in length. This benign tumor in the kidney does not have a clear outline that would separate it from the kidney tissue. But, despite this, fibroma does not have the ability to grow into adjacent tissues. Like most similar neoplasias, it is dangerous as it grows, putting compressive pressure on the renal pelvis and calyces, deforming them.
Despite the accuracy of diagnosis in modern medicine, fibroids are often confused with cancer. Since it is asymptomatic, its discovery in most cases occurs by chance during a routine examination or investigation of another disease. For reasons of preventing the development of malignant neoplasia, they resort to surgical intervention. These benign kidney tumors are removed by resection or radical nephrectomy.
Course and prognosis
Benign tumors, when detected in a timely manner and properly treated, do not pose a threat to life and have a favorable outcome. Predicting the consequences of malignancy is much more difficult, since many factors must be taken into account.
The most dangerous formations are those in which cancer cells grow into veins and actively metastasize. Unfavorable outcome for patients who, for some reason, cannot undergo surgery.
In this case, death occurs due to the presence of serious complications and significant intoxication. The patient’s age also influences the outcome of the disease—older people are more likely to survive than younger patients.
- After surgical treatment, the prognosis is favorable.
Renal cyst. Cyst
Quite common formations of renal tissue are cysts. The cyst is a bubble of connective material, inside of which there is a yellow liquid. Like any other benign tumor in the kidney, the cyst has no symptoms, being small in size. Growing to a large size, the cyst causes significant discomfort. And as a result of pressure on the urinary tract, it can even cause kidney failure.
Diagnosis of a cyst is no different from diagnosis of other neoplasias. Such a benign kidney tumor is most often subject to dynamic observation. If malignancy is suspected, the cyst is surgically removed. Surgery is also used if the cyst has a large diameter and affects the functions of the organ.
urovrach.ru
Diet and nutrition
If renal angiomyolipoma is diagnosed, you should strictly adhere to a special diet that inhibits the development of the tumor and prevents exacerbation of the disease. In this case, it is necessary to minimize salt intake.
Dietary rules for angiomyolipoma boil down to complete abstinence from alcoholic beverages and coffee, eating small portions 6 times a day, and consuming at least 1.5 liters of fluid daily. It is allowed to consume low-fat dairy products, vegetable broths, lean soups/borscht, low-fat meat, cereals, pasta, eggs, vegetables, and steamed cutlets.
Weak tea is allowed. For sweets, dried fruits, baked apples, honey, and jam are allowed.
Diagnostics and therapy
At the 7th Congress of ROOU, the famous professor V.B. Matveeva presented a report that became a real breakthrough in the drug treatment of renal AML. Scientists have proven the fact that one of the targeted drugs, belonging to the group of mTOR inhibitors, reduces the volume of renal angiomyolipoma by 45-50% over a 12-month course.
Although there is currently no reliable data on the tolerability of this drug, it can be firmly stated that this is the greatest breakthrough in this field. After all, everyone knows that drug treatment is less traumatic for the human body.
It is important to know. If you have been diagnosed with kidney angiomyolipoma, it is strictly forbidden to resort to treatment with folk remedies.
Self-medication in such a case cannot be effective; moreover, it can lead to dire consequences, including
and to death. If you value your health, then first of all consult a doctor.
Only an experienced doctor will give you an accurate diagnosis and prescribe the correct treatment.