Of all types of malignant lesions of paired organs of the excretory system, clear cell kidney cancer is the most common. It accounts for just over 80% of all cases of carcinogenic pathologies in this area.
Often in the literature you can find other names for this disease - hypernephroma or hypernephroid cancer - they all mean the same thing. The name is due to the appearance of the tumor - when cut, the tissue looks lighter due to the high concentration of accumulated fat in atypical cells.
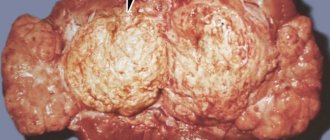
Macroscopic specimen of the kidney for clear cell carcinoma
Peculiarities
When talking about this type of cancer, it is important to mention the distinctive features that are characteristic only of hypernephroma. Typically, these tumors do not develop in pairs, i.e., only one kidney is affected. Early tumors are more successfully treated, but from the third stage the prognosis will be unfavorable.
It is important to highlight the following points:
- clear cell kidney cancer is more often registered in men, women get sick less often, which is associated with lifestyle and work;
- neoplasia, as a rule, is localized on one organ, and quite rarely spreads to a healthy kidney, which can happen in the later stages of carcinogenesis;
- the course of the disease is extremely difficult, which is especially true in the later stages;
- hyperneuroid cancer is much easier to treat than other kidney malignancies;
- the prognosis of stages 3 and 4 is unfavorable; in the latter case, treatment is exclusively palliative;
- the tumor in the early stages has a clearly visualized capsule separating it from healthy organs and tissues;
- the level of cancer malignancy remains the same at all stages of carcinogenesis (i.e., aggressiveness does not increase).
Note. Clear cell kidney cancer received its name due to the light yellow color when the tumor is cut. This is due to the accumulation of more lipids compared to healthy cells. When a removed tissue sample is treated with hematoxylin and eosin, it turns red or pink.
What is the prognosis for hypernephroid kidney cancer?
Kidney hypernephroma is a malignant tumor that can metastasize to a number of organs and lead to death. Depending on the stage of development at which the disease was diagnosed, the further prognosis depends:
- Detection of a tumor at the initial stage of development, subject to complete therapy, can cure 9 out of 10 patients.
- Treatment started from the second stage of the disease leads to long-term remission in 50% of patients.
- Metastasis to other organs allows only 15% of patients to live for more than five years.
- If the kidney grows and surrounding organs are damaged, the prognosis is unfavorable.
Causes
Clear cell kidney cancer
Hypernephroma often develops in older people (60-80 years). Residents of cities or regions with poor environmental conditions are more at risk of developing kidney carcinoma than people living in rural areas.
Risk factors are:
- environmental pollution with industrial waste;
- radioactive exposure;
- bad habits, especially smoking;
- poor quality nutrition, passion for fried, spicy, salted, smoked and food from fast food restaurants;
- work in hazardous enterprises, constant contact with toxic chemicals;
- chronic endocrine diseases, such as diabetes;
- long-term or uncontrolled use of certain groups of medications, for example, hormonal or diuretics;
- excess weight;
- genetic predisposition;
- gender (men get sick more often);
- elderly age;
- kidney injuries or protracted chronic processes that can cause malignancy of healthy cells (degeneration into cancer cells), long-term dialysis (provokes cyst formation, and this increases the risk of cancer).
Note. As medical practice shows, treatment of young people (up to 40 years of age) is much more difficult than that of elderly patients, therefore, when predicting survival, the age criterion must also be taken into account.
Clear cell renal cell carcinoma: treatment, diagnosis, prognosis
Over the last century, kidney cancer has changed several names: hypernephroma, clear cell carcinoma, renal cell carcinoma.
Today, its official name is renal cell carcinoma, and the clear cell variant is one of its morphological types, found in 80–90% of cases of all oncological pathologies of the kidneys.
The prognosis for this type depends both on the level of malignancy of the tumor itself and on the stage at which the disease is detected, and ten-year survival after removal of the tumor varies from 30 to 85%.
Clinical picture
Blood in urine is one of the signs of cancer
The initial stages proceed hidden. When the tumor is small, it can be detected only by chance, since there are no characteristic manifestations.
The first sign by which cancer can be suspected is hematuria, but earlier there may be various unpleasant sensations in the back. More often than not, they do not pay due attention to this, mistaking negative signs for sciatica or a muscle cold.
More pronounced symptoms are observed with tumor growth, when pathogenic cells spread beyond the capsule:
- presence of blood in the urine;
- pain of varying intensity in the lower back;
- renal colic;
- signs of intoxication: fever, nausea, weakness, dizziness and others;
- increased blood pressure due to increased formation of renin;
- causeless weight loss;
- loss of appetite;
- restless sleep;
- swelling of the lower extremities;
- increased urge to urinate.
Starting from the third stage, the metastatic process begins, therefore, as secondary foci form, additional signs begin to appear, for example, when the lungs are damaged, a cough occurs, pain in the spine indicates damage to bone tissue. At this time, there may be yellowing of the skin, hypertension, which is not controlled by medications, which may mean damage to the adrenal tissue. Mental disorders, deterioration of memory and mental functioning indicate secondary brain cancer.
Important. Varicose inflammation of the testicular veins in men can be a consequence of a kidney tumor. More often, such a sign appears on the right side before the main pathology, so in case of varicocele it is necessary to do an ultrasound of all organs of the excretory system. In women, one of the signs may be varicose veins on the legs. Less often, the development of hemorrhoids with open bleeding indicates malignant kidney damage.
In special cases, the neoplasm can be palpated, which can be done in thin patients. In addition, the manifestation of common symptoms for any type of oncology is typical: weakness, nausea, increased fatigue, loss of body weight, pallor of the skin, low-grade fever without the presence of an infectious component. In the latter case, the temperature is usually observed in the evening, but not in the morning.
What are the symptoms of the pathology?
With hypernephroid kidney cancer, symptoms can occur only at the last stage of pathology development, when metastasis occurs to other organs.
At the beginning of tumor development, there are no signs of the disease. Pathology can progress over decades without revealing itself. With a gradual increase in hypernephroid cancer, pain occurs in the kidney area, and blood periodically appears in the urine. If treatment is not started at this time, chronic renal colic may develop.
Oncological disease is manifested by a deterioration in the patient's appetite.
Along with this, it is observed:
- general weakness;
- loss of appetite;
- increased blood pressure;
- increased body temperature;
- a number of signs characteristic of damage by metastases to certain organs.
Classification
Bilateral kidney cancer
When considering the type of cancer, the histological picture, location features, metastases, and invasion into blood vessels are taken into account. Staging is determined according to the TNM system, which is standard in such cases, where the first letter indicates the presence of a neoplasm, the second - the involvement of the lymph nodes, and the third - the presence and number of metastases.
In a detailed description of clear cell kidney cancer, a classification is often used that shows the differentiation of pathogenic cells, which indicates the malignancy of the process. To do this, use the letter G and a number - the larger it is, the worse the forecast will be.
Ranking by degree of differentiation:
- G1 (high differentiation) – diagnosed quite rarely, in approximately 12-13% of cases on average. At the same time, the cells are similar to ordinary ones; they have small nuclear structures with fairly dense chromatin. The latter is a decondensed chromosome (DNA complexed with special proteins). This type develops slowly and, in comparison with other types of cancer, responds significantly better to the proposed therapy.
- G2 – occurs most often (35–55% of cases) . The cells of these tumors are characterized by slightly enlarged nuclei of not quite regular shape with small scattered chromatin. Carcinogenesis will have more aggressive forms, more often forms secondary foci in other organs, and is difficult to treat with cytostatic drugs and radiotherapy, which is due to the fact that neoplasias are capable of producing specific blocking components.
- G3 – poorly differentiated tumor . This form occurs in about a third of patients. Carcinogenic cells have large nuclear structures, nuclei in the form of an irregular ball or oval, uneven boundaries, chromatin is presented in the form of loose large globules.
- G4 (undifferentiated tumor) is a rare but very aggressive form of clear cell kidney cancer, reported in approximately 7-15% of patients. In this case, the nuclei will be the largest, and their contents will be presented in the form of large and clearly distinguishable block-like shapes. The tumor is characterized by rapid development and the fastest spread of metastases. The forecast is extremely negative.
As with other types of oncology, clear cell kidney cancer is divided into four stages and zero or precancer, which is almost impossible to detect. The latter happens extremely rarely and is a great success for the patient.
The main stages are as follows:
- the first (intracapsular tumor) – the size of the neoplasia does not exceed 7 cm, it does not spread beyond the organ;
- the second – the tumor is also no more than 7 cm, but its cells are already present in the kidney parenchyma;
- third - signs of metastases are recorded in regional lymph nodes or pathogenic cells affect blood vessels (the tumor grows into the fibrous capsule of the organ);
- fourth or terminal – metastases actively spread throughout the body, secondary tumors are registered in nearby and distant organs.
Stages
To treat renal cell carcinoma, it is necessary to know the stage of its development and the degree of malignancy of the cells. There are four stages of the disease:
- At the first stage, the size of the tumor does not exceed four centimeters, and the body of the neoplasm does not grow into the surrounding healthy tissue;
- The second stage is characterized by a tumor larger than seven centimeters, which also does not infiltrate into surrounding structures;
- During the third stage, the neoplasm extends beyond the affected kidney and spreads to nearby tissues, and sometimes affects one lymph node;
- At the fourth and last stage, metastases are detected in other organs distant from the kidneys, as well as in distant lymph nodes.
When determining the degree of malignancy of cells, doctors indicate the English letter G with a digital index indicating tumor differentiation. With a cytological examination of the tumor, doctors can detect the following:
- G1 almost no changes occur in the cells, the tissue is similar to healthy and highly differentiated;
- G2 renal cell carcinoma has a moderate degree of differentiation;
- G3 degree means the presence of poorly differentiated cells;
- G4 tumor tissue differs from normal - cells do not differentiate;
- Gx it is impossible to determine what degree of differentiation the neoplasm has.
We recommend reading Symptoms of thyroid cancer, its first signs, prognosis and treatment
A high number indicates a more aggressive tumor and a poor prognosis.
Diagnostics
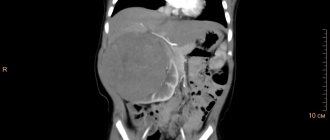
CT scanner
The doctor conducts a physical examination of the patient, listens to the medical history, and studies troubling symptoms. Signs of cancer may include curvature of the spine (indicating metastases), varicose veins of the scrotum in men, palpable kidney tumors in thin people.
Nonspecific tests include a general blood test (increased ESR, anemia) and urine (increased number of red blood cells with hematuria). Biochemical blood tests in people with cancer often reveal an increase in ferritin, haptoglobin, alkaline phosphatase and lactate dehydrogenase activity, as well as other abnormalities, which, however, cannot be considered specific. To clarify the circumstances of the disease and carry out differential diagnosis, the studies indicated in the table below are prescribed.
Table. Diagnosis of kidney cancer:
| Method | Comments |
| Allows you to evaluate the boundaries, density and homogeneity of the parenchyma, and identify anatomical anomalies of the organ. The method is safe. Low price and high information content make it a mandatory primary test for suspected cancer. |
| Static nephroscintigraphy is used. The principle of detecting carcinogenesis is based on the fact that radioactive substances do not accumulate in a malignant neoplasm, i.e., the image in the photo will be distorted or completely absent if the organ is completely damaged. |
| X-ray with contrast of renal blood vessels. The doctor can see abnormal enlargement of the arteries, abnormal vascularization in the tumor mass (in the form of a web-like mesh), aggregation of the radiopaque substance in the form of small clusters, and other pathologies. |
| Allows you to identify abnormal transformations in the tissue structure of the kidneys and the spread of carcinogenesis to neighboring organs. |
| These are modern high-precision diagnostic methods. The clinician receives multiple layer-by-layer images from different angles, which gives an idea of the smallest details of the cancer (up to 1-2 cm). If necessary, a contrast agent is used; magnetic resonance imaging does not use x-rays. Methods are important when searching for metastases. |
| The obtained tissue samples are subjected to cytohistological analysis, which makes it possible to confirm malignancy and determine the type of tumor. |
Important. Clear cell kidney cancer should be differentiated from solitary cysts, adrenal neoplasms (of varying quality), polycystic disease, tuberculosis, abscess and other pathological conditions.
Hypernephroma
Hypernephroma
is a malignant epithelial tumor of the kidney, a type of renal cell carcinoma. Manifested by local and paraplastic (general) symptoms: gross hematuria, pain in the kidney area, palpable tumor-like formation, deterioration of general condition, weakness, weight loss, etc.
To recognize hypernephroma and differential diagnosis, excretory urography, retrograde pyelography, renal angiography, renal ultrasound, CT and MRI, and fine-needle kidney biopsy are used. Treatment is carried out in compliance with oncological principles and includes nephrectomy with lymphadenectomy, radiation and drug chemotherapy.
Hypernephroma (clear cell adenocarcinoma, Gravitz tumor, hypernephroid cancer) accounts for 2-5% of malignant neoplasms in general, and in clinical urology - up to 85% of all cases of kidney cancer.
Hypernephroma refers to tumors of epithelial origin and can develop from almost any structure of the nephron: glomerular capsule, loop of Henle, distal and proximal tubules. In men, hypernephroma is detected 2.5-3 times more often than in women.
In 2/3 of cases it occurs in patients aged 40–70 years. The TNM stages of hypernephroma development are similar to those of renal cell carcinoma.
Hypernephroma
The reasons for the development of neoplasia remain unknown, but nephrologists identify certain factors, the influence of which significantly increases the likelihood of kidney cancer. It is known that hypernephroma is detected 2 times more often in males and smokers.
Smoking is considered the main risk factor for the occurrence of tumors of urological localization - bladder and kidney cancer. Meanwhile, quitting smoking leads to a reduction in this risk by 15% over 25 years.
The renal epithelium is adversely affected by various chemicals: gasoline, asbestos, cadmium, organic solvents, herbicides, phenacetin-containing drugs, etc.
It has been noted that the frequency of detection of hypernephroma correlates with diseases such as obesity, arterial hypertension, diabetes mellitus, as well as the pathology of the kidneys themselves (chronic pyelonephritis, nephrolithiasis, tuberculosis, dystopia, polycystic disease, nephrosclerosis, etc.).
Patients with renal failure who are forced to undergo long-term hemodialysis are more predisposed to the development of neoplasms.
There is an increased risk of hypernephroma in patients with genetic pathology (Hippel-Lindau disease) and a family history (hereditary papillary cell carcinoma, hypernephroid cancer).
Hypernephroma is a softish node of variegated color with a pseudocapsule, microscopic examination of which reveals light polygonal and polymorphic cells containing lipids and numerous mitoses. Tumor cells unite into alveoli and lobules, merging into tubular and papillary structures.
The stroma is poorly expressed, hemorrhages and tumor necrosis are typical. In 45% of cases, invasive growth of hypernephroma is detected, it invades the pelvis, and spreads in the form of tumor thrombi through the veins.
Metastasis of neoplasia is lymphogenous (to the lymph nodes) and hematogenous (to the lungs, contralateral kidney, liver, bones).
It may take several years from the moment a tumor appears in the kidney to the development of the first clinical symptoms.
The clinical picture of hypernephroma is characterized by the classic renal triad (hematuria, pain, palpable tumor) and extrarenal manifestations. The first thing that 2/3 of patients usually notice is the appearance of blood in the urine (hematuria).
As a rule, hematuria develops suddenly and is not accompanied by pain; may be transient, minor, total or profuse in nature.
Frequently recurring or intense hematuria leads to severe anemia of the patient. In some cases, microhematuria occurs, which can only be detected by urine examination.
The formation of blood clots can cause ureteral occlusion and an acute attack of renal colic. Very characteristic of hypernephroma is the appearance of pain after hematuria, and not before it, as with kidney stones.
More often the pain is constant and has a dull, aching character.
It is possible to palpate the altered kidney through the anterior abdominal wall or lower back only in half of the cases. Compression of the veins (renal, inferior vena cava, testicular) in men can lead to the development of varicocele. Paraplastic (general) manifestations of hypernephroma include causeless fever with chills, myalgia, arthralgia, weakness, loss of appetite, weight loss, nausea and vomiting.
Detection and differential diagnosis of hypernephroma requires a detailed urological examination, including excretory urography, retrograde pyelography, renal angiography, renal ultrasound, renal CT and MRI, fine-needle biopsy of the kidney and morphological analysis of the tumor. Already during the examination of the patient, characteristic asymmetry of the abdomen, increased venous pattern on the anterior abdominal wall in the form of a “jellyfish head”, dilation of the veins of the spermatic cord, and edema in the lower extremities can be identified.
A clinical blood test reveals an increase in ESR, anemia, polycythemia; in the general urine analysis - erythrocyturia.
To exclude the source of bleeding in the bladder (stones, diverticulum, tumors), cystoscopy may be necessary.
At the first stage, ultrasound and Doppler ultrasound of the renal vessels provide information about the location and size of the space-occupying lesion and the likelihood of vascular invasion.
Intravenous urography reveals a deformation or defect in the filling of the pyelocaliceal system, pushing the ureter towards the spinal column.
With a pronounced decrease in renal function and the impossibility of obtaining excretory urograms, retrograde pyelography is performed. To study the involvement of the renal vessels in tumor invasion, renal angiography and venography are performed.
Using CT or MRI, the size and extent of hypernephroma are detailed, and enlarged lymph nodes are identified.
For the purpose of preoperative morphological verification of the diagnosis and staging of the oncological process, a kidney biopsy or lymph node biopsy is performed to determine the histotype of the tumor formation. To exclude the possibility of hypernephroma metastases in distant organs, osteoscintigraphy, chest radiography, and liver ultrasound are performed.
If a tumor is detected, surgery, x-rays, or systemic chemotherapy may be undertaken.
If the function of the second kidney is satisfactory and the hypernephroma is operable, a radical nephrectomy is performed, including removal of the kidney with the adrenal gland, surrounding tissue and lymph nodes.
At stage I of the tumor process (neoplasia with a diameter of less than 7 cm, not extending beyond the capsule), poor functioning or absence of another kidney, a partial nephrectomy can be performed.
If radical intervention is not possible, arterial embolization may be attempted to block the kidney blood vessels supplying the tumor.
X-ray or chemotherapy for hypernephroma can be used alone or in combination with a surgical stage.
Methods such as cryotherapy, radiofrequency ablation, HIFU therapy with high-energy focused ultrasound are of experimental value.
In general, long-term results for hypernephroma are the same as for renal cell carcinoma.
For prevention, harmful carcinogenic effects (smoking, chemical and medicinal agents) should be excluded, and existing kidney pathology should be promptly eliminated.
The key to early detection of a neoplasm can be regular ultrasound examinations of the kidneys in practically healthy people. If blood appears in the urine or lower back pain, a detailed examination is necessary.
Source: https://www.KrasotaiMedicina.ru/diseases/zabolevanija_urology/hypernephroma
Treatment
Nephrectomy – removal of all or part of the kidney
Therapy for the hypernephroid type of cancer is characterized by certain features. Although it is complex in nature, it should be noted that the main and most effective method of treatment is radical removal of the tumor.
In parallel with this, chemotherapy is prescribed (both before and after surgery), but in this case its effectiveness will be low compared to other oncological diseases. The sensitivity of pathogenic cells to radiotherapy is even lower. The last two methods are more often used in later stages, as palliative measures.
Other types of treatment, such as targeted therapy, hormonal therapy, or immunotherapy, are rarely performed. There is evidence that for a certain circle of people they can improve the patient’s condition and prolong life expectancy by 15-20 percent.
Surgery
The choice of technique will depend on the type of clear cell cancer, its location and stage, and the presence of individual metastases, as a rule, is not a contraindication for surgery.
The techniques used may be the following:
- Nephrectomy is a total removal of the diseased kidney, adrenal gland, ureter, adjacent tissue together with regional lymph nodes. Indicated for significant tumor sizes and the absence of numerous closely located metastases. If there are distant secondary lesions, the operation is not performed.
- Partial removal of an organ (resection, partial nephrectomy) can be performed at an early stage, when the tumor is small and there is no invasion into adjacent tissues.
- Ablations are low-invasive methods of eliminating small tumors in the complete absence of metastatic process. There are several varieties: cryo-, radiofrequency and microwave ablation. The essence of the methods is quite similar - electrodes or small tubes are connected to the neoplasia, through which a detrimental effect is exerted on the cancer cells. All manipulations during the procedure are monitored using ultrasound or a tomograph.
The question of the advisability of partial resection is still debatable. A number of researchers note that the best results can be obtained exclusively after total nephrectomy.
Most doctors are inclined to carry out organ-preserving operations when the tumor size is up to four centimeters and there are no signs of metastasis, but some of them are of the opinion that cancer larger than two centimeters has a higher chance of recurrence. With any choice, clinicians must conduct numerous scrupulous studies and, based on detailed diagnostics, choose the method of surgical intervention.
Note. Surgeries for oncological lesions of the kidney can also be performed laparoscopically, however, this technique is not widely used at the moment.
Arterial embolization
Renal artery embolization
The essence of the method is to stop blood flow in the vessels feeding the cancerous tumor. This helps stabilize or significantly slow down the growth of neoplasia. Arterial blockage can act as an independent type of therapy, but more often precedes nephrectomy.
The essence of the procedure is to insert a catheter through the femoral artery, which delivers emboli, balloons or sclerosants to the desired location, blocking the blood flow in the vessel. All manipulations are monitored under the control of x-ray equipment.
Immunotherapy
The technique refers to conservative methods of treatment and is more used for late stages, when it is impossible to remove cancer surgically. Interleukin-2, alpha-interferon and their analogues are usually used (or the drugs are combined), which in certain cases makes it possible to increase the effectiveness of all treatment measures for clear cell cancer by up to 20% and increase the period of remission.
Important. For sarcomas, immune drugs are not effective.
Chemotherapy
Doxorubicin is a chemotherapy drug used for cancer.
The use of cytostatic drugs (Capecitabine, Doxorubicin, Sorafenib, Vinblastine and 5-Fluorouracil and others) in the treatment of kidney cancer is not as important as in other types of cancer, but in the presence of relapses and metastases, their use alleviates the patient’s condition. Such drugs are often used in combination with immunotherapeutic treatment.
The weak effectiveness of cytostatics in this case is due to multidrug resistance of tumors due to the presence of special genes. At this stage, researchers are studying this phenomenon through the use of special inhibitors (Verapamil and Cyclosporine derivatives).
Hormonal and radiotherapy
Previously, progesterone preparations were more widely used, but recently they have been practically abandoned due to low efficiency. The same applies to radiation. Malignant kidney tumors, as practice has shown, are persistently resistant to these types of therapy.
Forecast
With timely diagnosis and adequate treatment at the first stage of the disease, 90% of patients experience a complete recovery. The prognosis worsens when the tumor grows into the fascia, surrounding tissue, lymph nodes, and blood vessels.
In case of late detection of cancer, refusal of treatment or incomplete treatment, the prognosis is extremely unfavorable. A poor prognosis is also observed with some histological changes in clear cell carcinoma, for example in the presence of sarcomatoid or rhabdoid elements.
Prognosis and prevention
In the first and second stages of clear cell cancer, most of the operated patients live 5-10 years (70-88%), but in later stages the prognosis is unfavorable due to the spread of metastases and the high risk of relapses.
Prevention consists of giving up bad habits, maintaining a healthy lifestyle and proper nutrition, avoiding contact with radiation and chemical toxins, for example, asbestos, cadmium derivatives and others. Regular preventive examinations with a specialized doctor remain important. The latter is especially important for people at risk.
Risk factors
The main reasons that provoke tumor growth include:
- smoking for a long period (renal cell cancer is 4–5 times more common);
- hereditary factor;
- obesity, unhealthy diet with consumption of large amounts of quickly digestible carbohydrates (sugar, sweets, carbonated drinks), milk, fatty foods;
- industrial hazards;
- long-term use of antibiotics, cytostatics, corticosteroids and other drugs;
- arterial hypertension;
- renal failure.