A hemodialysis fistula is a device for repeated hemodialysis. As a result of impaired renal function, renal failure develops, accompanied by the removal of nitrogen metabolism products and toxins from the blood, an imbalance of electrolytes and acid-base balance. Patients who develop acute or chronic kidney failure are prescribed hemodialysis.
Reasons for the formation of arteriovenous fistulas
Depending on the etiological factor that caused the formation of a shunt between the arterial and venous networks, the following types of fistulas are distinguished:
- congenital (diagnosed in rare cases),
- traumatic (wounded by a bullet or knife),
- postoperative (including after organ biopsy),
- infectious genesis,
- artificial.
Arteriovenous fistula
The latter type is used when preparing a patient for hemodialysis in order to avoid daily puncture of the vein before purifying the blood. In case of renal failure, treatment with an artificial kidney device is used for a long period of time; if it is not necessary, the fistula is removed surgically.
We recommend reading the article about arteriovenous malformation. From it you will learn about the pathology and its symptoms, the threat to the patient, diagnosis and treatment of the disease.
And here is more information about radiofrequency ablation.
Advantages and disadvantages
The phenomenon under consideration has its advantages and disadvantages.
The first category includes:
- Easy installation operation.
- Easy rehabilitation period.
- Accessibility for every patient.
- The reality of withdrawal at any convenient time.
Disadvantages of this phenomenon:
- It is impossible to accurately predict the consequences in all cases.
- Difficulties in corrective surgery in some congenital pathologies.
- Risk of re-intervention.
Blood circulation in the area
The symptoms of the disease are associated with the location of the fistula, but there are also general hemodynamic disturbances characteristic of all such conditions:
- Arterial insufficiency (steal syndrome) - due to the flow of blood into the venous bed in the arteries, blood pressure drops, and tissues in the area of the blood supply experience a deficiency of nutrients and oxygen.
- A drop in systemic blood pressure with manifestations of circulatory failure, shortness of breath, and increased pulse rate.
- Formation of a venous aneurysm under the influence of pressure for which the resistance of the vein wall is not designed. Over time, rupture may occur with intense bleeding.
- Vessel thrombosis due to slower blood flow in the branches below the fistula area.
How to properly prick a fistula on hemodialysis
Rules for puncture:
- The puncture is carried out at a distance of 3-4 cm from the anastomosis.
- Place the arterial needle antegrade; in case of retrograde placement, hematoma may develop at the puncture site.
- The venous needle is placed only along the bloodstream.
- In the case of using a single-needle dialysis scheme, the needle is positioned along the blood flow.
- Puncture the fistula in a new place (an aneurysm is likely to develop due to thinning of the vessel walls).
Signs of arteriovenous fistulas of internal organs
The clinical picture for small formations is usually blurred. A large discharge of blood leads to a pronounced disruption of the functioning of the organ, as its nutrition and removal of metabolic products changes.
Dural
When there is a direct connection between an artery and a vein, which are located in the dura mater of the brain or spinal cord, dural (from the Latin durus, hard) fistulas arise. Unlike other anomalies of the structure of blood vessels, they are acquired.
Their formation is associated with injuries, infectious processes, and thrombosis of the vascular bed.
Arteriovenous fistula of the spinal cord
Its development involves branches of segmental arteries that arise from the aortic trunk and veins that flow into the common venous plexus. The most typical location is considered to be in the lumbar spine. The clinical picture is associated with compression of the nerve fibers or tissue of the spinal cord itself. The course of the disease is usually slowly progressive. Signs of a spinal dural fistula include:
- weakness in the legs, up to paresis or paralysis;
- reduction of all types of sensitivity;
- intestinal dysfunction;
- urinary incontinence;
- impotence in men.
Fistula between the arteries and veins of the brain
Cerebral fistulas form branches of the carotid or vertebral arteries, less often they are located in the cerebral sinuses. The danger of their occurrence is associated with a high risk of rupture and hemorrhage in the brain.
The following symptoms are observed in this condition:
- sharp and intense headache,
- nausea, vomiting,
- visual impairment,
- chaotic movements of the eyeballs (nystagmus),
- noise in ears,
- drop in blood pressure.
Cerebral fistula
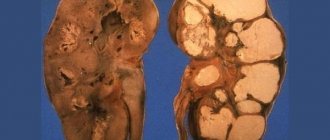
Fistula in the kidneys
The main manifestations of arteriovenous connection in kidney tissue are:
- high level of arterial and venous pressure,
- kidney bleeding,
- loss of red blood cells and protein in urine,
- heart failure,
- varicose veins of the spermatic cords or ovaries.
Vascular fistulas in the kidneys, as a rule, are congenital malformations. They are distributed throughout the parenchyma and often lead to intense bleeding, which may require removal of the organ.
Symptoms
Small fistulas are usually asymptomatic, clinically manifesting only as their size increases. In this case, the following occurs:
- redness and swelling of the skin;
- clearly visible swollen veins;
- swelling of the limbs;
- lowering blood pressure;
- weakness, decreased performance.
Swollen veins with arteriovenous fistula
With large fistulas, there is a significant decrease in blood pressure, which causes increased heart rate. This leads to the formation of heart failure, which is characterized by:
- cyanosis of the skin;
- feeling of lack of air;
- dyspnea;
- deformation of the fingers like drumsticks (thickening of the terminal phalanges).
The formation of a traumatic arteriovenous fistula occurs very quickly, literally within 2–5 hours.
Formation for hemodialysis
In chronic renal failure, the body cannot independently get rid of metabolic products due to the reduced filtration capabilities of the kidney tissue. In such cases, blood purification procedures are carried out artificially. The blood passes through the artificial kidney apparatus and then returns to the vascular bed.
The need for daily access to the circulatory network is greatly facilitated after suturing the artery with the vein. The formed fistula is located under the skin, it is easy to puncture, the walls are denser than those of a vein, and the blood circulation rate is higher.
Watch the video about creating an artriovenous fistula for hemodialysis:
Methods for diagnosing arteriovenous fistula
Magnetic resonance imaging
The doctor may hear the sound of blood flow over the area of the suspected arteriovenous fistula. The movement of blood through the AV fistula creates sounds similar to the noise of a car engine.
If the doctor hears this noise, then you will need to undergo additional examination methods, such as:
- Ultrasound
is the most effective and common method for identifying arteriovenous fistulas of the upper and lower extremities. In this study, an instrument called a transducer is placed against the skin. The transducer emits high-frequency sound waves that bounce off red blood cells, allowing the speed of blood flow to be measured. - Computed tomography (CT).
A CT scan allows you to see whether the blood flow is bypassing the capillaries. You will be given an injection of contrast, this is the drug that is visible on the CT scan. The CT scanner will then move to take pictures of the suspected diseased artery. After this, the images will be sent to a computer monitor for evaluation by your doctor. - Magnetic resonance angiography (MRA).
An MRA may be used if your doctor suspects you have an arteriovenous fistula in an artery deep under the skin. This study allows you to examine the soft tissues of the body. MRA works on the same principle as magnetic resonance imaging (MRI), but involves the use of a special drug (dye) to create images of blood vessels. During an MRA or MRI, you lie on a table inside a long tube-like machine that produces a magnetic field. An MRI machine uses a magnetic field and radio waves to create images of tissue in your body. Using these images, the doctor will be able to detect an arteriovenous fistula.
Positive and negative aspects of the installation
The formed fistula is located under the skin, it is easy to puncture, the walls are denser than those of a vein, and the blood circulation rate is higher. This makes it possible to quickly connect to the device and reduces the risk of blockage of a vessel at the site of permanent injury. The advantages of this technique also include:
- use of the patient’s own tissue (low risk of rejection and infection);
- can work for several years with proper care;
- there are no disturbances in systemic hemodynamics, since the connection is small.
The main disadvantage of installing a fistula is the period of its formation, which can last for 30–50 days. In some patients, due to weak current and low blood pressure, the fistula cannot fully mature, so this method has to be abandoned.
Advantages, disadvantages and possible complications
Despite the fact that the native arteriovenous fistula is today the gold standard in obtaining permanent vascular access, it, like any technique, has its advantages and disadvantages.
Advantages
The advantages include such indicators as:
- Convenient localization. The fistula is located close to the surface, which gives easy access to the vessels of the hand.
- The possibility of rejection is completely excluded, since only the patient’s own tissue is used.
- The internal location minimizes the possibility of infection.
- There is virtually no risk of blood clots.
- Durability.
Flaws
The most significant disadvantages are:
- The need to wait until the fistula matures in the fistula arm. Before vascular access can be used for dialysis, blood flow must thicken and dilate the vessel walls. Usually it takes 1.5 – 2 months. During this period, a permanent or cuffed CVC is used.
- The risk of fistula not maturing is quite high in patients suffering from hypotension or anemia. If there is a weak blood flow into the veins or low pressure in the anastomosis, the formation of a fistula will not occur.
It is also important for the patient to constantly monitor the condition of the AVF and competent care of the fistula arm.
Complications
It is also necessary to know that the creation of a fistula disrupts the normal flow of blood flow. Blood from the artery does not move slowly through the veins, thin vessels and capillaries, but quickly returns through the fistula, which creates additional stress on the heart. And this can affect your health. The following situations are possible:
- Steal syndrome. The limb below the fistula will be cold, and signs of necrosis or paresthesia may appear.
- Aneurysm formation. Then the risk of perforation and air penetration (embolism) increases.
- Oxygen starvation of the heart muscle, since most of the blood goes to the pulmonary artery.
- Carpal tunnel syndrome. Due to the significant expansion of the vein, the vessel can compress the median nerve at the wrist, which can lead to functional disability of the hand.
Preparing for treatment
In order to reduce the risk of postoperative complications before the patient is sent for surgery, the following examinations are required:
- ECG with functional tests,
- chest x-ray,
- Dopplerography of blood vessels,
- angiography,
- Ultrasound of the kidneys and heart,
- general blood tests, for HIV, viral hepatitis,
- biochemical study of kidney and liver tests, blood electrolytes,
- Analysis of urine.
All detected violations must be compensated, and the use of any medications must be agreed with the vascular surgeon.
Carrying out the operation
Creation of a fistula for hemodialysis
The forearm is most often chosen for installation of an arteriovenous fistula. The resulting anastomosis is called radiocephalic; the cephalic vein and radial artery are used for it. There may be the following types of connection of vessels:
- lateral surfaces of veins and arteries (first method);
- the side of the artery and the end segment of the vein (technically difficult, but the best result);
- end connection and use of the end of the artery and the side of the vein give little blood flow in the future.
First, the artery is ligated and crossed, and then the venous segment. After their communication, the surgeon sutures the vessels, then the wound. When listening above the anastomosis area, a characteristic noise in the form of a trill or a cat's purr is detected. When the fistula is applied correctly, it is long and has a low timbre.
Recovery after
Hemodialysis is possible only after the fistula has fully matured. The following signs indicate that she is ready for puncture:
- absence of redness, discharge or inflammatory infiltrate in the suture area;
- there is constant noise above the anastomosis or vibration, but no strong pulsation;
- the vessel has increased in diameter;
- there is tension and increased elasticity of the fistula vein.
At first, the patient is recommended to keep his hand in an elevated position and provide complete rest to speed up wound healing. Then a mandatory set of therapeutic exercises is prescribed, but lifting weights or doing strength exercises is not allowed.
How many years is it designed for?
Fistula is a long-term solution; with proper care, it can last for several decades. The service life depends on how the operation was performed, whether complications arose after the operation or during hemodialysis. In case of poor-quality anastomosis formation, ineffectiveness is possible due to insufficient blood flow velocity.
The service life may be shortened due to the development of complications of aneurysm, thrombosis of the fistula for hemodialysis.
As a result of injuries in the postoperative period, there is a possibility of damage to the formation. You need to treat your fistula hand with care and avoid overexertion with physical activity. If you take care of the condition, this will allow the anastomosis to work for a long time.
What information is missing from the article?
- Detailed review of medications
- More practical treatments
- Innovative developments in this area
- Qualified expert opinion
Fistula Care
In order to extend the service life of an artificial arteriovenous fistula, you need to adhere to the following recommendations:
- Wash the suture area daily before dialysis with antibacterial soap, then dry the skin completely;
- A noise should always be heard above the site of the fistula, so listen to it at least once a day, and report any changes to the doctor;
- touching the fistula should not be painful, and the skin over it should not be warmer than the surrounding one.
Thrombosis as a serious complication
If the arm is injured or the vessels are compressed, the fistula can become blocked due to the formation of a blood clot, so it is not recommended to bend the arm too much, and you should also avoid tight clothing, straps, and bracelets.
Temperature changes have a negative effect on the condition of the anastomosis. Therefore, it is not recommended to visit a sauna, bathhouse, sunbathe in the open sun, or be outside in very hot weather. You should also not engage in hardening or winter swimming, or wash clothes in cold or excessively hot water.
Thrombosis as a complication after fistula placement
To regulate blood pressure levels, take medications prescribed by your doctor; you need to monitor your readings at least once a day. Patients are advised to drink enough drinking water and limit strong tea and coffee.
Low and high blood pressure are equally dangerous for the patient, since weak blood flow increases the risk of thrombosis, and hypertension can lead to the formation of an aneurysm and bleeding after its rupture.
Lifestyle
In the first weeks after surgery, you need to provide rest to the fistula arm. During the day, you must wear a soft scarf orthosis; at night, you should place your hand on a hill.
As the fistula matures, you should constantly listen to the noise coming from it. During normal operation, the noise will be continuous and distinct, and each new sound should follow from the previous one.
You should not be too protective of your fistula arm; reasonable physical activity will only be beneficial. Complete inaction, as well as forceful movements that require tension, are unacceptable.
NB!
There is no need to be afraid to touch the fistula itself. A light touch should not cause any discomfort. This should be done constantly in order to feel the vibration from the advancement of blood flow, and at the same time check the temperature, which should not be higher or lower than other areas.
It is important to constantly monitor blood pressure and avoid sudden changes.
Carry out hygiene procedures regularly, using separate means from others.