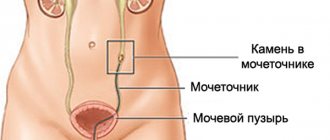
Angiomyolipoma is a benign tumor with a complex structure. It consists of adipose tissue, muscle fibers and modified blood vessels. This tumor is usually located in the kidneys, but can also be located in the pancreas.
There are two types of renal angiomyolipoma:
1. Sporadic or isolated. This is the most common type of disease. It is observed in 90% of cases;
2. Congenital. With this type of renal angiomyolipoma, it occurs against the background of a hereditary form of tuberous sclerosis (Bourneville-Pryn disease). In this case, neoplasms are usually localized on both kidneys and in large numbers.
The transformation of angiomyolipoma into a malignant tumor (malignancy) is extremely rare.
Causes of the disease
To date, no confirmed causes of AML have been established, with the exception of a hereditary factor.
Most experts agree that, in addition to heredity, some kidney diseases (pyelonephritis) and tumors that are not necessarily localized in the genitourinary system (angiofibroma, etc.) can lead to angiomyolipoma.
The triggering factor for AML is pregnancy. This is due to the presence in angiomyolipoma of receptors for the sex hormones progesterone and estrogen, the level of which increases during pregnancy.
Contributing Factors
The following factors may contribute to the formation of angiomyolipoma in humans:
• Tuberous sclerosis is a hereditary pathology associated with mutations in the TSC1 and TSC2 genes. This disease causes various tumors to form, including rhabdomyomas, oncocytomas, and angiofibromas, in different locations of the body.
Other pathologies that increase the likelihood of developing renal angiomyolipoma include:
• Von Recklinghausen's disease (neurofibromatosis); • Von Hippel-Lindau disease; • Sturge (Sturge)-Weber syndrome; • Autosomal dominant polycystic kidney disease.
Does the pathology pose a danger to life?
AML is a serious disease, in some cases life-threatening. Angiomyolipomas are benign formations, but in very rare cases they can become malignant.
There have also been cases where angiomyolipomas were primarily cancerous.
The main danger of angiomyolipomas is internal hemorrhages and necrosis, sometimes leading to infections and even sepsis.
The blood vessels in AML are altered, have a weak wall, muscle fibers grow faster than them, so there is a risk of rupture of the vessels and the tumor itself with retroperitoneal or intrarenal bleeding, requiring emergency surgical intervention.
The likelihood of kidney rupture increases as the tumor grows. The reasons leading to bleeding also include the increasing need for oxygen in rapidly growing AML.
This leads to increased stress on the vascular wall, aneurysms and breakthrough. 15% of patients who first consult a doctor about AML experience bleeding.
Why education is dangerous
Angiomyolipoma tends to grow. An advanced disease can lead to various complications. If the tumor reaches a large size, there is a chance that it will burst. Against the background of this situation, the patient experiences severe internal bleeding; lack of medical assistance leads to death.
The formation is considered benign and treatable, but under unfavorable circumstances, angiomyolipoma can degenerate into a malignant tumor. Intensive growth of the formation leads to compression of the liver and appendix, provoking the appearance of blood clots. Angiomyolipoma can put pressure on nearby organs, leading to tissue death. This phenomenon is dangerous due to kidney failure and subsequent death of the patient.
Treat the pathological formation in a timely manner to avoid serious complications. Avoid home therapy and follow your doctor's instructions.
Manifestation of the clinical picture
The symptoms of angiomyolipomas directly depend on the size of the tumor. For small (up to 4 cm) tumors, in 80% of cases the disease is asymptomatic.
When the size increases beyond 5 cm, more than 70-80% of patients begin to feel the clinical manifestations of the disease, forcing them to see a doctor, namely:
- dull pain in the lower back and lateral areas of the abdomen, aggravated by turns and bending; according to various sources, the pain symptom is observed in 40-70% of patients;
- frequent and sudden changes in blood pressure levels – in 12% of cases;
- palpable (in some cases by the patient himself) neoplasm – in 22%;
- weakness.
When the tumor size reaches 10 cm in 80% of patients, normal renal symptoms occur.
Bleeding (blood in the urine) due to rupture of a tumor or its vessel usually occurs with large tumors. However, in some cases, hemorrhagic manifestations can be observed even with relatively small sizes of AML.
Tumor rupture is accompanied by internal hemorrhage, severe acute pain and hemorrhagic shock (pallor, arterial hypotension, tachycardia, dizziness, fainting). A picture emerges of a growing palpable tumor.
Risk factors for angiomyolipoma
Genetic abnormalities that cause the growth of angiomyolipoma are either inherited or appear after a viral infection. Risk factors include:
• female gender/hormone dependence; • concomitant oncological processes in the urogenital tract; • age over 40 years; • pregnancy (during gestation, active tumor growth occurs); • chronic urological pathology.
Differential diagnosis is carried out with retroperitoneal liposarcoma with invasion into the kidney, adrenal myelolipoma, renal cell carcinoma, Wilms tumor, oncocytoma.
Diagnostic methods
- Ultrasound is a highly informative method for homogeneous, medium-sized (more than 5-7 mm) formations limited to the liver parenchyma. It manifests itself as a highly echo-negative signal against the background of the renal parenchyma, which makes the diagnosis of AML very reliable.
- CT scan . To diagnose angiomyolipomas, all types of computed tomography are used - multislice CT (MSCT), X-ray (X-ray CT), magnetic resonance CT (MRCT), ultrasound (USCT). A characteristic feature of AML is the presence of a significant amount of adipose tissue in the tumor, which in certain cases is pathognomonic. RCT and ultrasound CT in this case make it possible to establish a diagnosis with 95% accuracy. Low fat AML is much more difficult to diagnose, but is relatively rare (4.5% of cases). The absence or small amount of adipose tissue complicates the differential diagnosis of kidney cancer.
- Angiography . Not long ago, it was believed that vascular abnormalities (arteriovenous shunts, tortuosity, aneurysms) were characteristic only of AML. However, new research has shown that these same features can also occur in malignant tumors. Therefore, angiography - the study of vessels by introducing radiopaque substances into them and imaging using x-rays - has somewhat lost its significance. However, it is still used quite widely, since angiomyolipomas are characterized by vascularity.
- Biopsy. Puncture or aspiration biopsy is used in all cases where diagnosis by non-invasive methods (ultrasound, tomography, radiography) is difficult. A biopsy is indispensable in diagnosing low-fat AML and in some cases before embolotherapy.
- Laboratory methods for diagnosing AML include urine analysis, biochemical and general blood tests.
Classification
Doctors distinguish several forms of angiomyolipoma of the left part of the paired organ:
- hereditary species. It is formed against the background of a genetic predisposition, two kidneys are affected at once, and several foci of growth of pathological tissue are often diagnosed;
- sporadic (acquired). A common type, occurs in 80% of cases. Patients with this diagnosis are often women; only one kidney is affected.
There is another classification of education:
- typical form. The formation includes adipose tissue and is considered completely benign;
- atypical form. It is characterized by the absence of adipose tissue, which indicates a malignant course of the pathology. Histological examination helps to clarify the nature of the tumor.
Methods of therapy
The choice of treatment for angiomyolipomas depends on their size and clinical manifestations. Three treatment tactics are used:
- dynamic observation;
- drug therapy;
- surgical intervention.
In each specific case, preference is given to the method of treatment that allows preserving the organ and its functionality.
Surveillance tactics
Dynamic observation is used for small (up to 4-5 cm) asymptomatic tumors, and involves quarterly visits to a specialist and annual diagnosis using computed tomography and ultrasound.
The purpose of observation is to monitor tumor growth and changes in its quality.
If there is no significant increase in volume or change in quality, the tumor is not removed.
Drug treatment
To date, there is no proven drug therapy for angiomyolipomas that is supported by all specialists. It is not yet possible to get rid of tumors without surgery.
Drug therapy is under development. Innovative targeted drugs are being tested, in particular inhibitors of mTOR, rapamycin and its analogues.
In some cases, under the influence of drugs, the size of the tumor decreases, and it becomes safer.
The risk of rupture and bleeding is reduced, and it becomes possible to use minimally invasive treatment methods - cryogenic ablation, laparoscopic resection.
Surgical intervention
Surgery is the main, and in most cases, the only way to treat AML. Indications for surgery are:
- large (more than 5 cm), tumors that carry the risk of rupture and retroperitoneal bleeding;
- rapid growth of the tumor;
- renal hypertension, which is a consequence of pathological processes affecting the renal arteries;
- clinical manifestations in the form of pain, blood in the urine and other renal symptoms;
- compression of the collecting area by the tumor, and disruption of urine flow;
- danger of malignancy;
- impossibility of preoperative diagnosis.
Kidney resection
Resection is the removal of the tumor along with part of the kidney. The condition for resection of one organ is the normal functioning of the second kidney.
Enucleation
This is a modern, organ-saving method of tumor removal, minimizing damage to the organ itself. If the tumor is located in a fibrous capsule, it is possible to remove (enucleate) it, practically without affecting the kidney itself, with minimal blood loss.
Nephrectomy (removal)
Nephrectomy is the removal of the entire kidney along with adjacent tissue.
The operation has many contraindications and postoperative complications, and is forced, performed in the most desperate cases.
Nephrectomy is indicated when the tumor grows throughout the entire bundle, its localization in the sinus area and other cases when the integrity of the organ cannot be restored.
Vascular embolization
The essence of embolization is that a special material is injected into the artery or its branch feeding the tumor, which clogs the vessel and deprives the tumor of blood supply.
The insertion of the artificial embolus is controlled using radiography.
Embolization allows you to preserve the functions of the parenchyma and avoid traumatic scalpel surgery.
Indicated for multiple or single large angiomyolipomas, bleeding, and also when organ resection is associated with a high risk of renal failure.
Iodized oil, gelatin sponges, polyvinyl alcohol particles, pure ethanol, silk, and Teflon felt are used as embolization materials.
Most patients after embolization experience abdominal pain, nausea, fever, and leukocytosis, which can be relieved with analgesics, antibiotics, and NSAIDs. The duration of post-embolization syndrome is up to 4 weeks.
The practice of embolization throughout the world is small, so its effectiveness can be assessed only after sufficient accumulation of surgical results.
Organ cryoablation
A minimally invasive operation that involves freezing the tumor with argon and gel. Used for small (up to 4 cm) AML sizes. The technology is experimental and not yet widely used.
General information
Angiomyolipoma (AML) is a relatively rare type of benign tumor of mesenchymal tissue. ICD-10 code for renal angiomyolipoma: D30.0. Angiomyolipoma in most cases (80-85%) is an independent sporadic disease, and less often it is associated with lymphangioleiomyomatosis and tuberous sclerosis (15-20%).
The most typical for this type of tumor is kidney damage, much less often the tissues of the liver, pancreas, and adrenal glands are affected. Accordingly, angiomyolipomas of the liver, adrenal glands and pancreas are rare. Renal agiomyolipoma is a highly active benign vascular tumor consisting of endothelial cells of blood vessels, adipose tissue and smooth muscle cells. The tumor can develop both in the brain and in the cortex of the kidneys. More often it originates from the renal pelvis/renal sinus, and the ratio of endothelium, fat component and smooth muscle tissue within the same tumor can vary in different proportions.
The incidence of AML of the kidney is relatively low and varies between 0.3-3%, and without association with tuberous sclerosis it is even lower (0.1% in men/0.2% in women). It is more often discovered during preventive examinations or is an “accidental finding” during ultrasound of the kidneys. The tendency towards malignancy is insignificant. In almost 85% of cases, the tumor grows into the fibrous capsule of the kidney and extends beyond it; less often, invasive growth occurs in the inferior vena cava/renal vein or in the perirenal lymph nodes. It occurs in people of any age, but more often in adults 40-50 years old and older. Women aged 45-70 years are at increased risk of developing angiomyolipoma.
Forecast and prevention of complications
With a slow development of the disease and a mild clinical picture, the prognosis for AML is favorable. Angiomyolipoma surrounds itself with a capsule of connective tissue, which facilitates its surgical removal.
Recurrence and changes in nature towards malignancy are rarely observed. Timely treatment increases the chance of a full recovery. Generally accepted measures for the prevention of angiomyolipomas have not been developed. The main measures that help prevent complications are medical genetic consultations and immediate consultation with a doctor at the first symptoms of AML.
General recommendations for preventing complications include the need to maintain a healthy lifestyle, proper nutrition, quitting alcohol and smoking, and moderate physical activity.
Advantages of Top Assuta
- Each doctor at the clinic is an experienced specialist who has undergone extensive training in leading medical centers around the world. Specialists in the treatment of benign tumors of internal organs working in our center are among the best experts in the country.
- Modern diagnostic equipment makes it possible to draw certain conclusions about the disease and plan treatment measures in just three to four days.
- A wide range of treatment methods - cutting-edge immunomodulating drugs, catheter ablation, surgical interventions.
- Convenient form of payment, no prepayments or commissions. Possibility to pay for procedures step by step, as you receive them.
- A considerate and caring attitude towards the patient has been and remains one of the basic principles. Each patient is the center of attention of doctors and uses the services of a personal case manager (the list of such services includes translation of medical documents, coordination of doctors, etc.).
- 5
- 4
- 3
- 2
- 1
(3 votes, average: 3.7 out of 5)
Are there drugs to treat angiomyolipoma?
Targeted therapy (“target” is a target) is sometimes used to treat tumors associated with tuberous sclerosis. This can be explained by the fact that the lesion in this category of people is bilateral, there are many tumors, their sizes are large, so surgical treatment is impossible.
There is evidence that treatment can be used to reduce the size of the formation in order to be able to perform organ-conserving surgery. Clinical trials of targeted drugs are currently underway.