Causes of the disease
In urology, urethral diverticula are more often detected in women. Among other urological pathologies, this disease is diagnosed in 1.4-5% of cases, mainly between the ages of 30 and 60 years. The size of the diverticulum cavity is on average 2–3 cm in diameter; it can be located in any part of the urethra, in most cases in the posterior wall. As a rule, urethral diverticula are single; multiple urethral diverticula are less common.
When urinating, the urethral diverticulum increases, filling with urine, then decreases again. Part of the urine may be retained in the pathological cavity, and then released from the urethra in separate drops. The danger of a urethral diverticulum lies in the presence of conditions for the development of urethritis, diverticulitis, cystitis, abscesses, the formation of stones, and the formation of benign tumors.
Taking into account etiofactors and morphological structure, acquired (false) and congenital (true) urethral diverticula are distinguished.
The causes of congenital urethral diverticula are:
- dysembryogenetic disorders - residual duct of Gartner;
- improper fusion of primordial folds;
- dilatation of paraurethral cysts, etc.
Much more often, urologists have to deal with acquired diverticula of the urethra. In these cases, the causes of pathology may be:
- birth injuries;
- intraurethral interventions (for example, rough catheterization of the bladder, bougienage of the urethra);
- infection of the paraurethral glands with microbial flora in nonspecific urethritis, chlamydia, gonorrhea;
- abscess formation of the glands of the urethra.
Symptoms and course of the disease
In most cases, diverticulum develops without active symptoms, so it can be diagnosed in rare cases, so the extent of the disease is not fully known.
Noticeable manifestations develop, as a rule, with a complicated course of urethral diverticula - inflammation, bladder outlet obstruction, stone formation, malignancy.
Symptoms of urethral diverticulum:
- painful urination, pain when urinating and urgency (imperative urge to urinate);
- discharge of pus from the urethra;
- relative urinary incontinence (leakage of urine after finishing urination);
- pain during intercourse (dyspareunia);
- vaginismus;
- hematuria (blood in the urine).
It is worth paying attention to the possibility of a diverticulum in chronic lower urinary tract infections that cannot be treated.
The quality of life with urethral diverticulum is significantly deteriorated. Exacerbations of symptoms can be episodic, and the duration of the period of remission can reach several years. When patients see their doctor for chronic pelvic pain, urinary problems, and frequent episodes of recurrent infections, the possibility of urethral diverticulum often escapes the doctor's attention.
What are the dangers of having a urethral diverticulum?
Urethral diverticulum can lead to a large number of complications. Stagnation of urine in the urethral diverticulum leads to its infection, which in turn leads to an exacerbation of inflammatory processes, and as a result, an exacerbation of symptoms. Periodic exacerbations of urinary tract infections are observed in approximately 30% of patients.
Impaired urine outflow also contributes to the thickening of urethral mucus and the deposition of urinary salts and leads to the formation of secondary stones (stones) of the diverticulum (1.5-10% of cases).
Large urethral diverticula can impair the flow of urine from the bladder, leading to acute urinary retention.
Chronic inflammation of the mucous membrane of a urethral diverticulum can cause metaplasia (changes in structure) and malignancy (malignant degeneration) of the mucous membrane lining the diverticulum, with the appearance of foci of transitional cell or keratinizing cancer. Such cases are extremely rare; in modern literature there are no more than 100 described cases of urethral diverticulum tumor.
What is prolapse of the urethral mucosa in women?
Urethral prolapse is a protrusion or prolapse of the urethral lining through the external opening of the urethra.
This condition most often occurs in prepubertal girls and postmenopausal women. Upon examination, a round, often “donut-shaped” protrusion of the mucous membrane is visualized and a narrowing of the lumen of the external opening of the urethra is observed.
Because urethral mucosal prolapse is rare, misdiagnosis rates are high.
Differential diagnoses range from simple urethral caruncle to rhabdomyosarcoma. Only sufficient experience of the doctor can help avoid incorrect diagnoses and associated consequences.
Urolithiasis, prolapse
There are diseases of the urethra associated with the formation of stones and urethral prolapse:
Urolithiasis affects people of different age groups. Stones form in the bladder and urinary duct. When stones come out along with urine, injuring the mucous membrane, acute pain occurs. Due to blockage of the duct by stones, the bladder does not empty completely. The choice of treatment - therapy or surgery - is determined by the number and size of stones.
Prolapse is the loss of all layers of the urethral wall through the opening, complete from the outside: (along the entire length) or incomplete (lower part). The reason for the prolapse of the urethra is the downward displacement of the bladder due to weakening of the ligamentous-muscular apparatus that holds it.
Externally, it is a mucous formation at the opening of the urethra. The disease is alarming only when sexual life is disrupted, pain is felt when walking, and urine output is complicated. Prolapse requires surgery.
Medical history
Solingen first described urethral prolapse in 1732. Most authors believe that urethral prolapse is limited to the distal urethra.
In the past, treatment was mainly surgical. Currently, conservative therapy is the preferred initial treatment for uncomplicated urethral prolapse.
With strangulated urethral prolapse, as one of the main complications, surgical intervention is required. A lot of surgical procedures have been described for the treatment of prolapse of the urethral mucosa.
Surgical excision of mucosal prolapse in women is the fastest method of cure and is the definitive therapy. Procedures such as cauterization and cryotherapy of the urethral mucosa using a Foley catheter are no longer practiced.
Provoking factors
The following factors can also lead to the development of female urethritis:
- possible injury to the genital organs;
- hypothermia of the patient's body;
- significant weakening of the immune system after serious illness or stress;
- severe dietary restrictions, deficiency of vitamins and nutrients;
- craving for alcoholic beverages;
- chronic inflammation processes;
- diseases of the urinary system;
- menopause and pregnancy;
- violation of intimate hygiene by the patient.
Symptoms and treatment of urethritis in women are of interest to many.
Definition of the concept
Prolapse of the urethral mucosa in women is defined as complete eversion and exit of the urethral mucosa from the external canal (see figure below).
Urethral prolapse should be distinguished from a urethral caruncle, in which only part of the urethral mucosa protrudes outward and from a urethral polyp, which is a tumor-like formation on a stalk or broad base.
Prolapse of the urethral mucosa. Complete circular eversion of the mucous membrane of the distal urethra.
Symptomatic manifestations
Eversion of the urethral mucosa in women is accompanied by constant pain and burning in the area of the urethra, the pain syndrome is especially noticeable when walking.
The presence of a protruding fold is determined visually or by contact. The swollen formation has a pink or bluish tint. There is swelling and hyperemia of the genital organs, which increase in size. The situation is aggravated by urinary disorders. A persistent urge to urinate frequently results in difficulty urinating. Urinary incontinence is noted, and blood is found in the fluid itself. Bleeding can be seen during contact examination of the external genitalia and appears on underwear.
Video: Prolapse of the uterus
Prolapse (prolapse) of the uterus, vagina, bladder. Causes. Treatment. Operation
Causes of prolapse of the urethral mucosa
The exact cause of urethral prolapse remains unknown, however several theories have been proposed. These theories can be categorized as either congenital or acquired factors.
Congenital factors include weak pelvic floor structures leading to insufficient genitourinary support and urethral hypermobility, as well as internal urethral abnormalities (eg, abnormally wide urethra, excess mucosa), neuromuscular disorders, urethral malposition, and elastic tissue deficiency in the small organs. pelvis
Acquired factors include trauma during birth, prolonged vaginal labor or obstetric lacerations, and poor tissue quality in frail and malnourished women.
Risk factors for urethral prolapse include:
- increased intra-abdominal pressure due to chronic cough or constipation
- urethral trauma, including multiple births
- heavy physical activity
- chronic inflammatory process of the pelvic organs
- weight, body mass index exceeding acceptable values
- Poor nutrition and poor hygiene may be additional possible risk factors
- a decrease in estrogen levels during menopause, as well as hormonal imbalance in prepuberty.
Urethral prolapse in women has become much less common since the introduction of estrogen replacement therapy.
Make an appointmentMake an appointment with a gynecologist by calling 8(812)952-99-95 or filling out the online form - the administrator will contact you to confirm the appointment, guaranteeing complete confidentiality
Forecast and preventive measures
The basis for a favorable outcome is timely treatment. Preventive measures are aimed at eliminating excess weight, heavy physical activity, and preventing the development of inflammatory processes in the organs of the genitourinary system.
To increase muscle tone of the pelvic floor, special Kegel exercises have been developed.
- Squeeze the pelvic floor muscles for 10 seconds, trying to pull it up.
- Relax your muscles for the same amount of time.
- Perform the exercise for at least 5 minutes three times a day. Increase the duration of classes gradually.
Breathing during training should be free and deep.
Video: Safe surgical treatment of uterine prolapse
Safe surgical treatment of prolapse of the uterus, vagina, bladder (genital prolapse)
Pathophysiology
Urethral prolapse primarily affects the distal female urethra.
The separation of the longitudinal and circular muscle layers, due to an episodic increase in intra-abdominal pressure, leads to complete or circular eversion of the mucous membrane of the urethra through the meatus. Swelling and accumulation of the prolapsed mucous membrane create a “clamping” effect around the distal urethra, preventing venous circulation, increasing vascular congestion.
If left untreated, urethral prolapse can progress to strangulation and possible necrosis of the protruding tissue.
Clinical manifestations and symptoms of urethral mucosal prolapse
As is already known, there are two types of urethral prolapse - prepubertal and postmenopausal.
The clinical picture is different for both groups.
Prolapse in prepubertal age is predominantly asymptomatic. Often, urethral prolapse is an incidental finding during an examination by a doctor. The most common manifestation is spotting or staining of underwear. Hematuria is rare. Urinary disturbances are typically rare, but when present, patients may report dysuria, urinary frequency, or introital pain. Children may report genital pain if the mucosal prolapse becomes very large or if thrombosis and necrosis have developed. There are isolated cases of obstructive lesions when acute urinary retention develops due to urethral prolapse.
In contrast, postmenopausal urethral prolapse patients often experience the following symptoms:
- bloody discharge from the genitourinary organs
- dysuria, frequency or urgency, nocturia
- Both microscopic and gross hematuria may be observed
- if prolapse of the urethra is severe, the mucous membrane may be pinched, which leads to venous obstruction, thrombosis and necrosis of the prolapsed tissue. Patients with strangulated urethral prolapse may experience suprapubic pain, dysuria, hematuria, and urethral bleeding
- A urinary tract infection is also possible.
On physical examination, urethral prolapse appears as protruding mucous membrane from the external urethral meatus. In children, there may be a pinkish-orange stagnant mass in the center of the urethra. The mass may be painful and tender to palpation. The mucosa is ulcerated in most cases and usually bleeds on contact.
In adults, urethral prolapse manifests as erythematous, inflamed mucosa protruding from the urethra. The mucous membrane may be bright red or dark bluish. Depending on the development of the process, tissue prolapse can be infected, ulcerated or necrotic.
The initial diagnosis of urethral prolapse by a physician requires careful consideration due to the rarity of the condition. The differential diagnosis should include urethral or vaginal malignancy, urethral caruncle, ureterocele, condyloma, and rhabdomyosarcoma.
Treatment can be conservative, or in case of a complicated process, surgical.
Treatment methods
Inflammation of the urethra in a woman whose symptoms are pronounced is treated, like any infectious disease, with antibacterial therapy, which includes both local treatment and general medications.
Prescribed drugs are taken in various forms:
- pills;
- intravaginal suppositories;
- intravenous injections;
- liquid dosage forms for administration through a catheter.
| Type of inflammation of the urethra | Name of drugs | Price in rub. |
| Non-specific | Azithromycin | 30 |
| Cefazolin | 25 | |
| Ceftriaxone | 25 | |
| Trichomonas | Benzydamine | 200 |
| Ornidazole | 160 | |
| Trichopolum | 70 | |
| Gonococcal | Ceftriaxone | 20 |
| Cefixime | 700 | |
| Ciprofloxacin | 15 | |
| Clotrimazole | 11 | |
| Levorin | 200 | |
| Chlamydial | Tetracycline | 25 |
| Erythromycin | 25 | |
| Doxycycline | 35 | |
| Mycoplasma | Tetracycline | 25 |
| Viral | Penciclovir | 300 |
| Ribavirin | 50 | |
| Herpes | Acyclovir | 20 |
The duration of treatment and dose are determined by the doctor depending on the degree of damage, the stage of the disease, and the patient’s tolerability of the drug. Good results are achieved when treating urethritis with Azithromycin. It is used without additional means; it has a gentle effect on the female body.
The drug Ciprofloxacin has a wider spectrum of action. It is prescribed as the main drug, it has no side effects and does not affect the gastrointestinal tract. The duration of treatment is up to 20 days. Prescribed doses are 0.25–0.5 g twice daily. Can be administered by injection, 0.1 g 2 times a day.
Traditional methods
Inflammation of the urethra in women (symptoms must be accurately correlated by the doctor with the type of disease) can be treated with supportive care, in the form of home remedies.
When treating inflammation, you should follow an integrated approach:
- At the initial stage of the disease, doctors advise drinking plenty of fluids. This helps flush out bacteria from the body.
- At the second stage, you should start taking the prescribed medications. Traditional home remedies should be in addition to the main treatment. And it would be good to consult a doctor before starting to use them.
- At subsequent stages of treatment, thermal procedures in the form of sitz baths, to which herbal decoctions are added, help.
Relieve inflammation and unpleasant symptoms with herbal decoctions, which should be taken for at least 15–20 days. After this course, you should take a 2-week break and then continue treatment.
Recipes:
- Leaves of nettle, mint, calamus, and horsetail are taken in equal proportions, poured into 500 ml of water, and boiled for 30 minutes. The decoction should be drunk before bed, ½ tbsp.
- Take 100 chopped parsley leaves and pour in milk until it covers the herb. Place everything in the microwave and keep until the milk evaporates. Take the resulting product during the day, 40–50 g, every hour.
- Herbal mixture consisting of rose hips, horsetail, juniper berries, pour 500 ml of water. The collection should be no more than 2 tbsp. l. Boil everything and leave for 15–20 minutes. Then strain and take 1 glass in the morning on an empty stomach and before bedtime.
- Take 2 tbsp. l. dry black currant leaves. Pour 500 ml of water, boil a little and leave for 20-30 minutes. After straining, take the decoction throughout the day.
- Infusion of blue cornflower flowers. Add 80 g of freshly picked flowers to 200 ml of boiling water. Infuse the collection for 1–1.5 hours. After straining, take 2-3 tbsp 2 times a day. l. before eating.
All decoctions are taken outside of exacerbation, they are prepared daily and should be drunk regularly, without skipping days. For better infusion, decoctions should be wrapped in a warm cloth.
For pain in the lower abdomen, local warming baths are used. They are made from decoctions of St. John's wort, yarrow and chamomile. Take 3 tbsp. l. each herb, pour 1–15 liters of boiling water, then pour into a basin prepared for the bath, diluting with warm water. The warming procedure should not last more than 20 minutes.
To enhance the diuretic effect and remove infections from the body, you can drink a homemade drink made from apple cider vinegar and honey (1 teaspoon each) added to a glass of water. The drink is consumed within a month.
Freshly squeezed juices from vegetables and berries help with urethritis. They should be taken daily, no more than ½ tbsp.
- Carrot.
- Cranberry.
- Parsley juice.
- Currant.
- Beetroot.
- Cranberry.
Cranberry juice increases the acidity of urine and increases the effectiveness of anti-infective drugs. Pharmacy tinctures based on Rhodiola rosea, Schisandra chinensis and aralia are used as maintenance therapy. The drugs are taken 20–25 drops daily for half a month.
general description
Prolapse of the urethral mucosa is a pathological process that develops against the background of loss of elasticity of the structural elements of the urethra in females. The urethra may prolapse completely or partially. In the first case, it is located symmetrically around the external opening of the urethra, and in the second - asymmetrically on any side. More often, this disease occurs in girls under 15 years of age and in older women, which is believed to be due to the poor development of the submucosal structures of the urethra in these age groups.
Among the provoking factors, the most significant are:
- Mechanical injury to the urethra.
- Chronic inflammatory diseases of the bladder and urethra.
- Frequent increase in intra-abdominal pressure with coughing, constipation, and the urge to defecate.
- A sharp decrease in the production of female sex hormones during menopause.
- Anatomical features of the structure of the female urethra: it is much wider and shorter than the male one.
The size of the prolapsed mucous membrane is variable: from a few millimeters to several centimeters in diameter. Due to venous stagnation, the prolapsed area, which initially has a red color, is pinched by the external opening of the urethra and subsequently acquires a bluish tint, and its swelling develops. In some cases, strangulation leads to necrosis of the prolapsed structure with the development of gangrene.
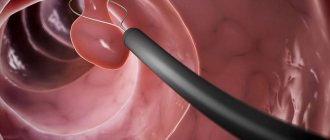
Diagnostics
First of all, the doctor is interested in the patient’s general health and disturbing symptoms. Then the urologist examines the genital organs and determines the extent of the disease. He finds out from the patient how long ago the discomfort due to the foreign formation began and whether there is any bleeding. For a more accurate picture, catheterization is prescribed, during which the bladder is emptied and an examination is performed. A cystoscopy is performed and the bladder is examined using an endoscope. Additionally, a consultation with a qualified gynecologist is scheduled.
Symptoms of prolapse of the urethral mucosa
At the very beginning of the disease, patients do not experience any discomfort, but over time the following symptoms appear:
- Urination becomes frequent.
- Urine is excreted with difficulty to such an extent that acute retention may occur.
- Urination becomes painful.
- Urinary incontinence may occur.
- There may be bleeding from ulcers in areas of prolapse.
- The prolapsed mucous membrane becomes painful when touched and interferes with walking and during moments of intimacy.
User Questions (7)
- Polina2017-06-30 14:25:20
After sexual intercourse, about 3 cm of mucous membrane appeared near the urethra. I began to go to the toilet more often, but I do not experience any pain. It’s unpleasant to walk if... read the answer >> - Taatyana2017-05-11 13:44:35
Hello, in 2014, 2 operations were performed for prolapse of the urethral mucosa with pinching. On the 3rd day I feel it is starting to increase again, is it possible to carry out a course of pills or is it necessary... read the answer >> - Maria2017-01-25 16:01:41
Mom is 69 years old. Diagnosis: prolapse, strangulation, ulceration of the urethral mucosa. 50 days have passed since the operation. The wound is still fresh and not healing. We treated it with levomikol, now we switched to tetracycline 3%. ... read the answer >> - GARIK2016-12-28 21:59:30
To narrow the valve on the bladder, an operation was performed by bougiening a catheter to size 16. During catheterization with disposable catheters, pain is felt, a wound remains. How to treat a wound on... read the answer >> - Natalia2016-12-12 16:17:28
Is it possible to perform urogenetic surgery at the same time? It is necessary to remove a urethral polyp measuring 3 by 3 cm and suturing the anterior wall of the vagina. Age 71 years old. Or is it better separately, so that there is no... read the answer >> - Natalia2016-12-10 08:22:37
Hello, can the bladder fall out of the vagina when internal organs prolapse in the form of a chicken egg? Or is it a prolapsed vagina with a symmetrical hole in the form of a smiley face at the bottom... read the answer >> - zaza2016-11-30 16:25:01
prolapse of the mucous membrane of the urethra 7 mm, an 80-year-old patient refuses surgery. Pain during urination in the external genital organs disappears, Pain, burning, cramping in... read the answer >>
Medical institutions you can contact:
Morphological and structural changes in the urethra have always attracted attention and remain relevant to this day. It is worth highlighting such pathologies that are no longer rare and can occur in both women and men:
- Prolapse of the urethra or prolapse (prolapse) of the urethra;
- Diverticulum of the urethra;
- Hypertrophy of the urethral mucosa.
Moreover, each of the above problems has its own age peaks, that is, the time when there is a high probability of their occurrence, with the exception of those forms of the disease that are congenital in nature and can manifest themselves from childhood.
For example, prolapse of the urethral mucosa (prolapse) is recorded with the greatest frequency in prepuberty (up to 14 years) and in the menopausal period (over 45 years). Urethral diverticula, as an acquired pathology, occur in 2–5% of cases, in the age range from 35 to 60 years.
Microflora in the organ
The channel for excreting urine in representatives of different sexes differs in microflora. Immediately after the birth of a child, various microorganisms enter his skin. They gradually penetrate into the body and settle on the mucous membranes and internal organs.
Bacteria cannot penetrate further than the mucous membranes; this process is hampered by the internal secretions of the body, urine, and ciliated epithelium, so they become attached to them. Pathogenic organisms that remain on the mucous membranes become the innate human microflora.
The female urethral mucosa contains several times more bacteria than the male urethral mucosa. It is dominated by lactobacilli and bifidobacteria. They produce acid, creating an acidic environment. If there are few bacteria, then the acidic environment is replaced by an alkaline one, which allows inflammatory processes to develop.
The composition of the microflora may change depending on the large number of sexual partners. Frequently changing partners introduces dangerous microbes into the body that can cause serious illness.
Men's channel
The male urethra during the embryonic period is similar to the female one, as it consists of the same structures. And once formed, it begins to differ significantly, becomes longer and smaller in diameter, is located inside the penis, and its functions, in addition to urine output, also include ejaculation.
The redistribution of these functions of the male body completely depends on the degree of filling with blood of the cavernous bodies and the spongy body, which surround the male urethra. With erection, the blood supply to the penis occurs, ejaculation occurs, and in the absence of blood supply to the penis, the process of urination occurs.
The male urinary canal has a length of 18-22 cm. In a state of excitement, the length becomes a third longer, in boys before puberty it is a third less.
The urethra in men is divided into posterior (the distance from the internal opening to the beginning of the corpus cavernosum) and anterior (the remotely located part of the canal).
It has two bends in the shape of the letter S:
- The upper (infrapubic) bend bends around the pubic symphysis (half-joint) from below as it passes from top to bottom of the membranous part of the urethra into the cavernous one.
- The lower one (prepubic, prepubic) is located at the point of its transition from the fixed part of the urethra to the mobile one.
When the penis is raised, both curves form one common one, the concavity of which is directed forward and upward. Throughout its entire length, the male urethra is not the same in lumen diameter; narrow parts alternate with wide ones.
Conventionally, the male urethra is divided into 3 parts:
- Prostatic (prostate). It has a length of 0.5-1.5 cm. It consists of tubules for ejaculate release and 2 ducts (prostatic and sperm excretory).
- Sponginous (spongy). The urethral part is located along the penis in its lower part and has a length of 13-16 cm.
- Cavernous (membranous). The longest section of the male urethra, the length of which is approximately 20 cm. The spongy section contains ducts of numerous small tubules. It is located deep in the perineum, passes through the urogenital diaphragm, which has a muscular sphincter.
The male urethra originates from the urinary sac. Smoothly moving into the prostate area, it crosses this gland and ends at the head of the penis, where urine and seminal fluid come out. The average size of the urethral lumen in men along its entire length is 4-7 mm, in boys 3-6 mm.
Female urinary tube
The female urethra is an anteriorly directed, straight tube passing close to the elastic vaginal wall and pubic bone. Its length is 4.8-5 cm, and its diameter is 10 - 15 mm, while it is easily stretched.
Inside, the urinary canal is lined with a mucous membrane, which has the appearance of longitudinal folds, due to which the urethral lumen appears smaller. In the female urethra there is a special obstructing pad consisting of connective tissue, veins, and elastic threads. It closes the duct of the urinary canal.
Read more Complications after curettage
The female urethra does not perform reproductive functions, although substances are excreted through it, which can be used to determine whether a woman is pregnant or not. The female urethra is surrounded by tissues that are similar in structure to the corpus spongiosum of the penis, and the corpus cavernosum of the clitoris, which is similar to the corpus cavernosum of the penis, is located in front of the urethra.
It is closely connected to the anterior wall of the vagina and is firmly attached to the lower branches of the pubic bones, as well as partially to the ischial bones.
Since it is short and wide in women, located next to the vagina and anus, the danger of bacteria, microbes and other pathogenic microflora entering it is much higher in women than in men. Therefore, they are more susceptible to genitourinary infections.
Urethral prolapse
There are many factors due to which a woman most often faces the problem of prolapse, and in the worst case, prolapse of the urethra. Among these factors it is worth highlighting:
- Frequent excessive stress on the body and abdominal muscles (lifting weights);
- Multiple genders (more than 3);
- Childbirth during which a large fetus was born weighing more than 4 kilograms;
- Functional problems with the intestines in the form of chronic constipation, when excessive straining during bowel movements increases intra-abdominal pressure;
- Injury to the urethra, including during rough sexual intercourse, which is due to the proximity of the vagina and urethra;
- Old age, when age-related changes occur in the ligamentous and muscular framework of the organ, due to the loss of elasticity of muscle and connective tissue.
It should be understood that the organ can prolapse completely along its entire length, then they speak of a complete form, or prolapse of the lower part of the urethra in isolation is an incomplete form.
A woman may experience the following symptoms:
- Dysuria in the form of frequent urination and imperative urges or, conversely, acute urinary retention (ischuria);
- Urinary incontinence;
- Discomfort and sensation of a foreign object, which is a section of the urethral mucosa;
- Pain is constant or intermittent in the lower abdomen.
Prolapse and protrusion of the urethra requires a urologist to carry out diagnostic methods that will confirm the disease. These include:
- Anamnesis collection. The doctor analyzes all the risk factors that could lead to this pathology;
- Inspection. In the process of visual assessment, it is possible to find elastic prolapsed urethral mucosa with visual swelling and a bluish tint;
- Laboratory diagnostics - clinical urine analysis (micro- or macrohematuria);
- Endoscopic technique – urethrocystoscopy;
- Bladder catheterization. In case of urinary retention, this method has not only diagnostic significance, but also therapeutic value.
Specifics of the examination
Medical diagnosis is mandatory. During the examination, hyperemia of the external opening of the urethra or adjacent tissues, discharge and pain on palpation can be determined. Such signs require a mandatory comprehensive examination.
The practice of doctors and reviews of women indicate the need for such diagnostics:
- extended urine analysis according to Nichiporenko;
- general blood and urine examination;
- urine test for the absence or presence of potentially dangerous bacteria to identify the pathogen;
- PCR for the purpose of analyzing biomaterial;
- bacterial sensitivity test to antibiotics;
- urine analysis for tuberculous mycobacteria, however, the result in this case can be obtained only after 10-12 weeks.
The diagnostic methods listed above are the most significant. In some cases, ureteroscopy may be necessary.
To adequately assess the genitourinary system, an ultrasound of the pelvic organs will be required.
Treatment of chronic urethritis in women is often difficult.
Urethral diverticulum
A urethral diverticulum is a so-called “protrusion” that resembles the shape of a “pocket” and communicates with its cavity through a narrow channel.
Causes:
- Disturbance of embryogenesis and tissue differentiation in the fetus, which leads to the congenital form of diverticula;
- Birth injuries, infections, invasive diagnostic or therapeutic measures;
Clinical manifestations can be characterized by a long asymptomatic period when the disease does not manifest itself in any way. But sometimes the disease from the very beginning acquires symptoms such as pain localized in the groin and iliac region, dysuria, urinary incontinence with frequent urge.
The process of urination has its own characteristics: it is accompanied by pain and a feeling of an existing obstacle; emptying of the bladder occurs in the form of an intermittent stream, followed by involuntary leakage of urine. In addition, during the process of urination, the patient may pay attention to the turbidity of the urine if there is an admixture of pus and protein; on the color of urine - with a reddish tint, due to the admixture of red blood cells.
Urethral diverticula in men and women have the following diagnostic directions:
- History and general examination;
- Clinical analysis of urine and blood;
- Sterility smear;
- Oncocytological study
- Ultrasound invasive and non-invasive;
- Urethroscopy.
Symptoms characteristic of prolapse
Later, the symptoms of pathology may be accompanied by the appearance of blood in the urine.
When the urethral mucosa prolapses, redness and swelling of this organ is observed. Over time, the urinary canal itself and the external organs of the reproductive system acquire a bluish tint. The eversion organ is easily palpable. In advanced forms of the disease, inflammatory processes begin at the site of urethral prolapse due to the accumulation of infection. Touching the mucous membrane causes pain. Possible symptoms include bleeding from the prolapsed area.
The disease also has secondary symptoms, such as:
- difficulty in emptying the bladder;
- the presence of blood impurities in the excreted urine;
- the desire to urinate becomes frequent and obsessive;
- constant presence of pain in the genitourinary area;
- incontinence or delay in the normal flow of urine;
- the volume of urine decreases due to frequent urge.
Return to contents
Hypertrophy of the urethral mucosa
Hypertrophy is the process of enlargement of the small glands of the urethral mucosa. This concept includes a wide range of pathologies that are accompanied by excessive growth of the inner layer with possible partial or complete closure of the lumen of the urethra. This condition is usually asymptomatic for a long time until problems with normal bladder emptying begin.
An important step in diagnosing this condition is testing for tumor markers. Timely exclusion of malignant growth is guaranteed to reduce the risk of mortality from this disease.
Editor
Dyachenko Elena Vladimirovna
Update date: 08/23/2018, next update date: 08/23/2021
February 19 at 15:17 —> 16081
URETHRA CARUNCULE
Urethral caruncle must be differentiated from urethral cancer. For small sizes, the caruncle is coagulated or excised with lasers similar to these lkmed.ru/catalog/xirurgicheskie-lazery/ .
The patient's position is like during stone cutting. Three stay sutures are placed on the mucous membrane of the urethra in the area of its external opening (at 3, 6 and 9 o’clock). Incision. Outward from the stay sutures, a scalpel tucked with a No. 10 blade is used to dissect the mucous membrane along the posterior semicircle of the external opening of the urethra. Using an electric knife, the submucosal membrane is separated from the posterior and lateral walls of the urethra, while simultaneously pulling it up by the holders.
Crossing the posterior wall of the urethra proximal to the caruncle, interrupted sutures with a 4-0 synthetic absorbable thread align the proximal edge with the mucous membrane in the area of the external urethral meatus.
They continue to sequentially cross the posterior wall of the urethra and suture the defect until the area of the mucous membrane with the caruncle is completely cut off. A 24F Foley catheter with a 5 ml balloon is inserted into the bladder. The wound is closed with a tampon soaked in Vaseline.
PROPRESSION OF THE MUCOUS MEASURE OF THE URETHRA
In the acute period, conservative treatment is prescribed to reduce swelling. Apply 4 stay sutures to the periphery of the prolapsed mucous membrane. The mucous membrane is dissected in the area of its transition from the urethra to the vagina to the level of the muscular layer. The urethral mucosa is grasped circularly with small Allis forceps. First, it is cut vertically on one side, then circularly excised. Interrupted sutures are placed with chrome-plated catgut suture 3-0 on the edges of the mucous membrane. The mucous membrane around the urethrocele is taken with 4 stay sutures. In the middle between the entrance to the vagina and the external opening of the urethra, the mucosa is dissected to the muscular layer, after which the mucous membrane of the urethra is grasped around the circumference with small Allis clamps. First, it is cut vertically on one side, then, continuing the cut around the circumference, it is completely excised. The resulting mucosal defect is sutured with chrome-plated catgut 3-0. In this case, the edge of the vaginal wall is aligned with the edge of the urethral mucosa.
POSTOPERATIVE COMPLICATIONS
When excision of a significant area of the mucous membrane in the postoperative period, the formation of a stricture of the urethra is possible. Chronic urinary retention and incontinence are rare.