Viral diseases have a special course. They spread quickly and also have several periods in pathogenesis, during which the clinical picture changes significantly. The danger from pathogens of such infections is posed not only by sick people, but also by carriers, which are often animals. One of these diseases is hemorrhagic fever with renal syndrome (HFRS). This pathology is an acute viral infection that a person can become infected with from small rodents. The disease is characterized by a specific immune response and occurs with significant intoxication and fever, vascular damage and impaired renal function.
There are several areas on the territory of the Russian Federation that are endemic for this problem. These include the Far East, Kazakhstan and Eastern Siberia, as well as Transbaikalia. The disease is not common, but on average 10–15 thousand patients are registered during the year. The risk group includes people working in agriculture and livestock farming, tractor drivers, as well as patients of other professions that involve direct contact with the external environment. Most often, males aged 17 to 50 years are susceptible to viral infection. Treatment of hemorrhagic fever involves acting directly on the causative agent of the disease, but symptomatic therapy also plays an important role, which includes detoxification, hemodialysis and infusions aimed at restoring normal kidney function.
Reasons for the spread of HFRS
Disorder of the functions of internal organs associated with the disease occurs against the background of damage by an infectious agent - an RNA-containing structure that belongs to the Bunyavirus family. Medicine knows several serovars, and each of them is distributed in a certain area. One of them is found in Russia - Puumala. All people are susceptible to this pathogen, that is, when it enters the patient’s blood, a cascade of pathological reactions develops, which cause the symptoms of hemorrhagic fever with renal syndrome. The disease is considered contagious. The virus enters the patient’s body, as a rule, through aerogenic or transmissible routes, through wounds on the skin. This happens both during work, in contact with the feces of small rodents, and also in everyday life, that is, the infection can be transmitted from one person to another.
When infected with a virus, it actively replicates – multiplies. It is accompanied by damage to the inner layer of blood vessels - the endothelium. This leads to increased porosity of arteries and veins. There is a gradual “sweating” of the liquid part of the blood into the tissue. This leads to disruption of many systems, but the kidneys suffer the most. The glomerular filtration rate decreases due to clots formed as a result of immune reactions entering the tubules. Such processes provoke a gradual worsening of nephron failure, which leads to increased intoxication.
The exact pathogenesis of the disease is currently unclear. Initially, it was assumed that damage to the vascular wall was associated with the tropism of the virus - its ability to invade certain cells. However, the hypothesis was refuted. In vitro, scientists did not notice any cytopathogenetic effects that the pathogen can cause.
There is a direct connection between the severity of the clinical picture and the introduction of viral RNA into the patient’s cells. Moreover, the greater the amount of genetic material that enters the body, the brighter the symptoms. This process is accompanied by a violation of the barrier function of the cells that make up the endothelial lining of blood vessels. Subsequently, damage to the filtering apparatus of the kidneys also occurs, which is associated both with the negative impact of the virus on the arteries and with damage to the nephrons by immune complexes. Despite the fact that the body tries to compensate for pathological processes by producing specific growth factors, the patient’s condition gradually worsens. Proteins produced during the reproduction of the pathogen also lead to increased vascular permeability and sweating of the liquid part of the blood.
Hemorrhagic fever with renal syndrome - prevention
For specific preventive measures, Korean vaccines created on the basis of Hantaan-type viral particles are used. In Russia, this type of vaccine is not certified, therefore specific prevention of the disease is not carried out on the territory of the Russian Federation.
For nonspecific prophylaxis the following is used:
- epidemic control over deratization in outbreaks;
- use of special protective glasses, gloves and respirators when working with grain, hay, or working in very dusty rooms;
- control over the quality of food storage, etc.
Clinical signs of the disease
The disease is characterized by staged development. This is a feature of most infectious lesions. It is customary to distinguish several stages of hemorrhagic fever with renal syndrome:
- The incubation period during which symptoms do not appear, although the pathogen has already entered the patient’s blood. It lasts from one week to one and a half months. There is a gradual damage to the walls of blood vessels, as well as transformations of metabolism.
- The prodromal period immediately follows the incubation period, but in some cases it is absent. This stage is accompanied by uncharacteristic symptoms: migraine, chills, general weakness and a slight increase in body temperature. It is problematic to suspect a specific disease at this stage. It lasts 2–3 days.
- The causative agent of hemorrhagic fever with renal syndrome, upon further reproduction, provokes a strong immune response. It is accompanied by a sharp increase in temperature to 400 C. From this moment, a febrile period begins, which lasts for 3–7 days. The peak of hyperthermia is recorded in the morning, while in the evening the symptoms soften.
- Subsequently, severe vascular damage is observed with the formation of petechiae and hemorrhages, as well as impaired renal function. There is a decrease in daily urine volume. This period is called oliguric and lasts for a week. At the same time, body temperature decreases, but patient complaints of pain in the lumbar region are recorded. The presence of blood is noted in the urine, while the total volume of its excretion decreases. There is also an accumulation of nitrogen metabolism products, which leads to an increase in intoxication.
- The patient's condition is gradually stabilizing. The disease transforms into the polyuric stage. Painful symptoms and manifestations of intoxication disappear. An increase in the daily volume of urine is detected, which reaches 3–5 liters per day.
- The period of convalescence is marked by significant variability in time. It can last from several weeks to 2-3 years. There is a gradual restoration of the functions of internal organs, which has a positive effect on the patient’s condition. However, general weakness and increased fatigue may persist for a long time.
In adults
The main manifestations of the disease are vascular symptoms and damage to kidney function. At the onset of the disease, the temperature rises, patients complain of weakness and aching joints. Metabolic products gradually accumulate. Nausea and vomiting occur, which does not bring relief. Subsequently, as the glomerular filtration rate decreases in the kidneys, diuresis is impaired. Blood appears in the urine and its volume decreases. This is accompanied by an increase in intoxication and painful sensations that radiate to the lumbar and abdominal area.
In children
In young patients, hemorrhagic fever is more severe than in adults. This is due both to the imperfection of the immune system and to the structural features of the vascular bed. The first sign of the disease is the development of fever, which is important to detect in time. Otherwise, a prolonged increase in temperature can negatively affect the functioning of the nervous structures and lead to the development of unpleasant consequences. Hemorrhagic symptoms in children also appear more intense than in adults. The development of massive bleeding is possible, which is life-threatening for a small patient.
What it is?
Its first description was made in 1935 in the Far East, then it turned out that it is widespread in the Moscow, Tula, Yaroslavl, Samara, Tver regions, and the Urals.
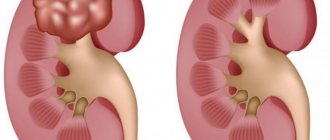
The disease is characterized by selective damage to the blood vessels of the kidneys. The infection is caused by viruses of the Hantavirus genus; they are carried by forest and field mice. The virus is released into the environment through the saliva and feces of rodents; infection occurs by inhaling air contaminated with particles of dried mouse secretions; the food route of infection is also possible - through products.
People are quite susceptible to the disease, but a sick person does not pose a danger to others. The infection leaves behind lasting lifelong immunity.
Diagnostic tests
Anamnesis is important in confirming the presence of a viral infection. The patient’s stay in an area where the disease is endemic is taken into account, as well as the possibility of contact with soil, water and small rodents. The nature of the course of the disease, that is, the presence of an incubation period, also matters.
During the examination of the patient, attention is paid to body temperature, the occurrence of petechiae and other vascular lesions, as well as possible pain in the projection of the kidneys. Blood tests are key to diagnosing HFRS. At the initial stage of the disease, a decrease in the number of leukocytes is characteristic, which is later replaced by a significant increase. With severe damage to the vascular endothelium, erythrocytosis develops first, and then anemia, which has a regenerative nature. Since hemorrhagic fever is characterized by thickening of the blood, a decrease in the number of platelets, cells involved in the coagulation mechanism, is also recorded in the general analysis. Changes in biochemical tests indicate significant changes in metabolism. The most important prognostic indicators are urea and creatinine. Their significant increase indicates a violation of filtration and leads to an increased risk of complications.
Testing the patient's urine is also of great importance. It reveals blood, protein and renal casts, which indicate damage to the nephrons and a decrease in the glomerular filtration rate. A characteristic change is also considered to be a decrease in density, which indicates a decrease in the concentrating ability of the kidneys. Hypoisosthenuria persists for a long period of time and is of great importance, and also affects the further outcome of the disease.
Methodological recommendations for diagnosing lesions imply periodic monitoring of tests, since it is important to monitor the disease over time. The frequency of tests is determined by the doctor based on the patient’s condition.
Differential diagnosis
If acute symptoms of HFRS appear, you must immediately consult a doctor , because the signs of this disease are very similar to other equally dangerous diseases: typhoid fever, influenza, pyelonephritis, leptospirosis.
Find out what are the symptoms of pyelonephritis here.
The doctor collects the patient’s medical history and also finds out his recent whereabouts . This is a mandatory item if HFRS is suspected, because in this way possible contact with infected animals is revealed.
Difficulties for diagnosis are erased and atypical forms of HFRS.
First, an external examination is carried out. The doctor pays attention to the persistent cyclical nature of the disease, symptoms characteristic of hemorrhagic fever, such as muscle pain, vision problems, rashes, oliguria, etc.
Next comes time for laboratory research :
- General and biochemical blood test (advanced);
- RNIF with blood serum testing (serological method);
- General urine analysis;
- A general blood test in the early period of the disease will show leukopenia, and only from 3-4 days you can see a pronounced increase in ESR and leukocytes;
- The PCR method will allow the doctor to detect the RNA of the virus raging in the body.
Special methods - enzyme immunoassay - ELISA, immunofluorescence reaction - RNIF, RIA - radioimmunoassay must be carried out over time . After all, the effect of antibodies in HFRS is not constant, and their maximum concentration is achieved only by the 13th day of illness.
The RNIF method must be applied as early as possible and repeated after 6 days of disease activity. Such a study will definitely confirm the diagnosis if antibody titers increase at least 3 times .
In severe cases and in the presence of complications, the doctor prescribes additional tests : FGDS, ultrasound, X-ray or MRI.
Treatment
A necessary condition in the fight against hemorrhagic fever with renal syndrome is hospitalization of the patient in an infectious diseases hospital. This is required to ensure the safety of others, since the disease is contagious. Bed rest is prescribed to reduce the load on the vascular bed. You will also need a special diet, which involves limiting protein intake and increasing calorie intake. This is necessary to facilitate kidney function. At the same time, it is important to provide adequate nutrition, since the body’s energy needs during the period of illness increase significantly.
Etiotropic therapy, that is, treatment aimed directly at the pathogen, is effective only in the initial stages of HFRS. In the future, the fight against the disease is based on drug support. It involves normalizing hemodynamics, restoring kidney function and relieving intoxication.
Overview of prescribed drugs
- At the initial stage of hemorrhagic fever formation, the administration of immunoglobulins shows good results. They help activate the body's defenses and more quickly get rid of the pathogen.
- Antiviral medications, such as Ribaverin and Cycloferon, can also be used in later stages.
- Angioprotectors are drugs that help protect the vascular wall from damage. These products include “Rutin” and “Prodectin”.
- Normalization of the rheological properties of blood is also important in the treatment of HFRS. This is achieved through the use of drugs such as Trental and Curantil.
- At the stage of oliguria, an important condition for the patient’s recovery is stimulation of diuresis. It is produced through the use of diuretics such as Eufillin and Furosemide.
Intravenous infusions of solutions allow you to restore the volume of circulating blood, and also help to cope with a decrease in the concentration of albumin, which is actively excreted through the kidneys.
In case of severe impairment of nephron function, patients are recommended to undergo hemodialysis.
Home methods
- Flaxseed is actively used in the fight against HFRS. It helps restore kidney function. You will need 1 teaspoon of the ingredient per glass of water. The liquid is boiled, after which 150 ml is consumed every 2 hours for 2 days.
- Red clover is used as a diuretic and antiseptic. You will need to pour 1 tablespoon of the plant into a glass of boiling water and leave for 2-3 hours, then consume throughout the day.
- An infusion of blue cornflower flowers also has a therapeutic effect. You will need 1 tablespoon of the plant, which is poured with 2 cups of boiling water and left for several hours. The finished medicine is consumed in 3 doses shortly before meals.