Loop diuretics are the most potent of all diuretics available in clinical practice. Most often, loop diuretics are used in the treatment of edema of various origins.
All loop diuretics, except ethacrynic acid, are sulfonamide derivatives in their chemical structure.
Chemical structure of loop diuretics
Loop diuretics list of drugs
List of drugs in Europe
The following loop diuretics are common in Europe:
- Bumex generic: bumetanide;
- Edecrin generic: ethacrynic acid;
- Demadex generic: torsemide;
- Lasix generic: furosemide;
- Sodium Edecrin generic: ethacrynic acid.
List of drugs in Russia and Belarus
The most common loop diuretics are:
- Britomar (Oral tablets)
- Bufenox (Oral tablets)
- Bufenox solution for injection 0.025% (Solution for injection)
- Diuver (Oral tablets)
- Lasix (Solution for infusion)
- Lasix (Oral tablets)
- Furosemide (Solution for intravenous and intramuscular administration)
- Furosemide (Solution for injection)
- Furosemide (Substance)
- Furosemide (Substance-powder)
- Furosemide (Oral tablets)
- Furosemide Lannacher (Solution for injection)
- Furosemide Lannacher (Oral tablets)
Comparison of drugs
Despite the emergence of other loop diuretics, the most popular substance in this group remains furosemide (Lasix). Ethacrynic acid is less effective than furosemide (especially in cases of renal impairment) and is the most toxic of all loop diuretics. For example, it has a greater risk of ototoxicity than furosemide. Therefore, it is used less frequently than all substances in this group, usually only when the patient is allergic to other loop and thiazide diuretics (since it does not contain a sulfonamide group). Bumetanide and torsemide (torsemide) differ from furosemide in their stronger and (torsemide) long-lasting action.
Properties of drugs
These are new generation medications that are used on an inpatient and outpatient basis. The classification is based on the properties of the substance, its effect on the body. On this basis they are divided into two groups:
- Those that block the production of aldosterone (an adrenal hormone that affects fluid retention by the body).
- Those that can influence the release of potassium.
Medicines are used on an inpatient and outpatient basis.
Based on the strength of their action, potassium-sparing diuretics are classified as weak, in terms of speed - slow-acting, and in terms of the duration of the effect - long-acting.
Indications for the use of loop diuretics
Loop diuretics are used in medicine mainly for the treatment of hypertension and edema of various origins, most often in congestive heart failure or renal failure.
Loop diuretics are used for:
- edema of various origins (hepatic, cardiac and especially renal), for example, edema associated with heart failure, cirrhosis of the liver, renal failure and nephrotic syndrome;
- in acute renal failure - increase renal blood flow and stimulate urine separation during anuria (soak the patient);
- hypercalcemia (intensively removes calcium from the body);
- for forced diuresis in case of poisoning with various chemicals, including drugs;
- loop diuretics are used for emergency treatment of pulmonary edema and cerebral edema;
- for arterial hypertension - prescribed only for severe heart failure; in other cases, due to their long-lasting action, thiazide diuretics are more preferable.
A systematic review by the Cochrane Hypertension group assessing the antihypertensive effects of loop diuretics found only a modest reduction in blood pressure compared with placebo. The review highlights the need for more randomized controlled trials.
Purpose and limitations
Drugs with a diuretic and potassium-sparing effect are used in cardiology to alleviate the condition of hypertensive patients. But they have a big disadvantage - they slightly reduce blood pressure, so they are usually combined with more effective hypertensive drugs.
Indications for the use of diuretics
In addition, indicated for:
- primary aldosteronism;
- renal edema;
- heart failure;
- gout
Potassium-sparing diuretics are prescribed in small doses for hypertensive patients. If the pressure remains high, the dose is not increased, because their effect is weak, and the number of negative consequences may increase. They are limited to prescribing one more diuretic.
In case of heart failure, when water is retained in the body, a small dose of a potassium-sparing diuretic is prescribed with a slow increase. This ensures complete resorption of swelling.
Diuretics have a beneficial effect on edema during pregnancy, when it is necessary to preserve potassium. The pregnant woman is prescribed a special diet and diuretics. This is done in the last trimesters.
Pharmacokinetics of loop diuretics
Loop diuretics are rapidly, but only partially absorbed from the gastrointestinal tract and are quickly eliminated from the body. For example, the bioavailability of furosemide when taken orally is about 60%. Torsemide is absorbed record-breakingly quickly (two to three times faster than furosemide) from the gastrointestinal tract. Most loop diuretics are excreted as metabolites (for example, furosemide binds to glucuronic acid in the kidneys, bumetanide is metabolized in the liver). Unlike oral administration, when administered into a vein, the effect of loop diuretics occurs very quickly, but it is short-lived.
The longest-lasting loop diuretic is torsemide - 2 times longer than furosemide (therefore it is the best of the group of loop diuretics for the treatment of hypertension).
Effect on the body
The use of loop diuretics is aimed at the filtration properties of the kidneys, making it possible to remove salts and unnecessary fluid from the body. The advantage of these drugs is that when used in the treatment of arterial hypertension, there is no increase in blood cholesterol levels, and there is no stimulation of the development of diabetes mellitus (inherent in thiazide diuretics).
But there is also a negative side: long-term use of these drugs leads to a decrease in the amount of sodium, magnesium and calcium present in the body.
The medications affect blood flow to the kidneys, reduce pressure on the heart, and increase the amount of urinary fluid.
Indications
Indications for the use of the presented medicines are:
High blood pressure
- edema resulting from increased sodium content in the body;
- increased blood pressure;
- heart disease (CHF - chronic heart failure);
- excessive amounts of calcium and potassium in the blood;
- diseases related to kidney function.
Contraindications
There are a number of contraindications for the use of this group of drugs:
Recommended topic:
Dill as a diuretic
- urine does not enter the bladder;
- diseases resulting in deviations from the norm in the frequency, rhythm, sequence of excitations and contractions of the heart;
- presence of allergies to drugs that are part of the sulfonamide group;
- decrease in the amount of circulating blood;
- the period of bearing a child and breastfeeding.
Mechanism of action of loop diuretics
Loop diuretics act on the Na-K-2Cl symporter (transporter) in the luminal part of the tubular epithelium of the ascending part of the loop of Henle. The consequence of this effect is inhibition of the joint transport of Na, K, Cl. Blockade of chlorine transport reduces the electrochemical gradient along the surface of the epithelial membranes of the nephron and, as a result, inhibits sodium reabsorption.
The strong diuretic effect is explained by the fact that it is in the ascending part of the loop of Henle that the bulk of sodium, and therefore water, is reabsorbed. Loop diuretics, through active sectionation, enter the lumen of the proximal tubules and compete with uric acid for excretion, which leads to its retention and hypercuricemia.
Loop diuretics also have a secondary effect. The secondary effect of this group of drugs is an increase in the production of prostaglandins, which leads to vasodilation and improved blood supply to the kidneys. NSAIDs block cyclooxygenases, which are involved in the synthesis of prostaglandins, so NSAIDs may reduce the effectiveness of diuretics.
Pros and cons of potassium-sparing drugs
Potassium-sparing diuretics, regardless of composition, have the following properties:
- retain potassium;
- have a weak diuretic effect, therefore they are very convenient for patients;
- not dangerous for the cardiovascular system.
Mechanism of action
But they have a number of disadvantages. Overdose causes dyspepsia and gastrointestinal disorders. In women, the menstrual cycle may be disrupted, and in men, gynecomastia and impotence may occur. Medicines lead to a reduction in the number of platelets, which in extreme situations provokes the development of thrombocytopenia. In mild cases, headache and urticaria are possible.
As with any other diuretic, the doctor is constantly obliged to monitor the patient’s condition: check the amount of potassium, prevent possible dehydration.
An excess of potassium can provoke the development of hyperkalemia, which adversely affects the condition of the heart and causes muscle weakness. Diuretics are contraindicated in renal failure.
It should be remembered that medications are prescribed only by a medical specialist. Self-medication is unacceptable here.
Side effects of loop diuretics
Common side effects of loop diuretics :
- hypovolemia,
- hypokalemia (it sharply increases the toxicity of cardiac glycosides),
- hyponatremia,
- hyperuricemia (can provoke a gout attack),
- hypocalcemia,
- hyperglycemia,
- hypomagnesemia – loss of magnesium is considered a possible cause of pseudogout (chondrocalcinosis),
- dizziness,
- fainting,
- hypotension.
Rare side effects of loop diuretics :
- dyslipidemia,
- increase in serum creatinine concentration,
- hypocalcemia,
- rash.
Ototoxicity (ear damage) is a serious but rare side effect of loop diuretics. Tinnitus and dizziness may occur, but in severe cases it can also lead to deafness.
Cross allergic reactions
Since loop diuretics such as furosemide, torsemide and bumetanide are technically sulfur-containing drugs (see image under chemical structure of loop diuretics), there is a theoretical risk that patients sensitive to sulfonamides may also be sensitive to loop diuretics. This risk is indicated in the drug package inserts. However, the actual risk of cross-reactivity is unknown, and there are some sources that dispute the existence of such cross-reactivity. One study found that only 10% of patients allergic to sulfonamide antibiotics were cross-allergic to loop diuretics. However, it remains unclear whether this is true cross-reactivity or whether the nature of such a reaction is different.
Ethacrynic acid is the only drug in this class of diuretics that is not a sulfonamide. However, it has a pronounced complication associated with toxic effects on the gastrointestinal tract.
Drug interactions
Loop diuretics, when combined with aminoglycoside antibiotics, dramatically increase the risk of severe ototoxicity (irreversible deafness); anticoagulants – increase the risk of bleeding; cardiac glycosides – increase the risk of arrhythmias; antidiabetic drugs from the group of sulfonylurea derivatives - increase the risk of hypoglycemia; NSAIDs - reduce the effect of the latter. Loop diuretics increase the effect of propranolol and lithium preparations.
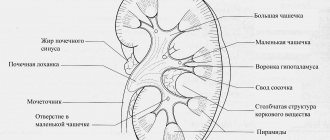
Physiology of urine formation and excretion
The kidney has a complex structure and consists of numerous (about 1 million) structural and functional units - nephrons.
The following physiological processes underlie urine formation and excretion:
- Glomerular filtration is the process of formation of primary urine (up to 150-170 l/day) as a result of blood filtration through the Bowman-Shumlyansky capsule in the glomeruli.
Tubular reabsorption is the process of formation of secondary urine (1.5-1.7 l/day).
Tubular secretion is the process of active release of potassium ions from the blood into the urine (into the lumen of the tubule) at the level of the distal nephron.
Each nephron contains a vascular glomerulus, which is connected to the tubular apparatus through the Bowman-Shumlyansky capsule. Through the walls of the capillaries of the glomerulus, large-molecular proteins are filtered into the capsule from the blood plasma. The filtration process is very intensive: 150-170 liters of filtrate - primary urine - are formed per day. The resulting filtrate enters the tubules, where it undergoes significant, 99%, reabsorption into the blood, i.e. reabsorption. Thus, after reabsorption, only 1% of liquid remains in the tubules, which amounts to 1.5-1.7 liters per day (normal daily diuresis). In this case, the reabsorption of water in the tubules is closely related to the reabsorption of various ions of sodium, potassium, chlorine, etc.
Tubular reabsorption is a complex process in which various enzymes (carbonic anhydrase) and hormones (aldosterone, antidiuretic hormone) take part.
Loop diuretics and thiazide
The duration of effect of most loop diuretics (except long-acting torsemide) is significantly shorter than that of thiazide diuretics.
Loop diuretics have a strong effect. A strong effect means a very high risk of developing side effects (primarily disturbances in electrolyte balance and acid-base balance). This puts loop diuretics at a disadvantage compared to thiazide diuretics when a not too strong but long-lasting effect is required (in particular, in the treatment of arterial hypertension).
Thiazide diuretics are more effective than loop diuretics in patients with normal renal function, and loop diuretics are more effective in patients with impaired renal function i.e. do not lose activity in acute kidney injury.
Physiology of urine formation and excretion
The kidney has a complex structure and consists of numerous (about 1 million) structural and functional units - nephrons.
The following physiological processes underlie urine formation and excretion:
- Glomerular filtration is the process of formation of primary urine (up to 150-170 l/day) as a result of blood filtration through the Bowman-Shumlyansky capsule in the glomeruli.
Tubular reabsorption is the process of formation of secondary urine (1.5-1.7 l/day).
Tubular secretion is the process of active release of potassium ions from the blood into the urine (into the lumen of the tubule) at the level of the distal nephron.
Each nephron contains a vascular glomerulus, which is connected to the tubular apparatus through the Bowman-Shumlyansky capsule. Through the walls of the capillaries of the glomerulus, large-molecular proteins are filtered into the capsule from the blood plasma. The filtration process is very intensive: 150-170 liters of filtrate - primary urine - are formed per day. The resulting filtrate enters the tubules, where it undergoes significant, 99%, reabsorption into the blood, i.e. reabsorption. Thus, after reabsorption, only 1% of liquid remains in the tubules, which amounts to 1.5-1.7 liters per day (normal daily diuresis). In this case, the reabsorption of water in the tubules is closely related to the reabsorption of various ions of sodium, potassium, chlorine, etc.
Tubular reabsorption is a complex process in which various enzymes (carbonic anhydrase) and hormones (aldosterone, antidiuretic hormone) take part.
How do they work?
Loop diuretics begin to act after 30 minutes. The spectrum of action of diuretic drugs is based on relaxing blood vessels and increasing renal blood flow; the drugs improve the connection of prostaglandins in the endothelial cells of the capillaries.
The drugs begin to act after about 30-60 minutes and end after about six hours. Loop diuretics cause disturbances in the countercurrent-turn mechanism of the nephron and increase glomerular filtration.
In addition, the mechanism of action of loop diuretics is to reduce the reverse absorption of chlorine and sodium ions, and in the nephron the absorption of magnesium is inhibited, thereby increasing the volume of its co-excretion with urine.
Loop diuretics affect renal blood flow. In addition, they reduce cardiac stress, as well as the tone of the veins and increase the volume of urine.
"Lasix"
The drug is produced in the form of an injection solution and tablets. The solution is infused intravenously. For edema, the drug is prescribed in an amount of 20-40 mg per day, for pulmonary edema - 40 mg. For high blood pressure - 80 mg per day (two doses). For high blood pressure - 80 mg per day (two doses). The diuretic begins to “work” two hours after use.
Before starting loop diuretic therapy, a person should be assessed for renal impairment, especially if daytime urine output is severely reduced. The fact is that the mechanism of loop diuretics is based on relaxation of blood vessels and increased renal blood flow.
During drug treatment, it is also necessary to monitor the functioning of vital organs, especially if the patient is forced to use Lasix in high concentrations. Unauthorized increase in dosage can lead to symptoms of poisoning and severe hypovolemia.