URODYNAMICS
URODYNAMICS
(Greek uron urine + dynamikos relating to strength, force) - the process of active excretion of urine from the body as a result of the coordinated activity of the neuromuscular apparatus of the calyces, renal pelvis, ureters, bladder and urethra.
The secretion of urine from the ducts of the renal papillae into the pelvis (see Kidneys) is carried out under the influence of two factors - secretory pressure in the tubular apparatus of the kidney, equal to 36.7-51.5 mm Hg. Art., and biphasic activity of the calyces.
When the muscles of the calyx are relaxed (the first diastolic phase, lasting an average of 4 seconds), urine is released from the duct of the renal papilla due to the pressure gradient in the tubular apparatus and the calyx. At this time, the sphincter of the calyx is in a closed state, which prevents urine from flowing into it from the pelvis. After the cup is filled with urine, the second, systolic, phase begins, lasting 3 seconds. In this phase, m contracts. recludor calycis, m. levator fornicis, sphincter of the fornix and relaxation of the sphincter of the calyx, m. Ion -gitudinalis calycis, resulting in urine pressure of 7.35 mm Hg. Art. moves to the renal pelvis.
The mechanism of movement of urine from the renal pelvis through the ureters (see) into the bladder has not been precisely established. There are two theories of urine transport through the ureter - the so-called. cystoid and peristaltic. According to the cystoid theory, the upper urinary tract consists of a pelvic and 2-4 ureteral dynamic sections - cystoids, which interact in a “pushing-locking” manner. In the first cystoid, the role of the detrusor (expelling muscle) is performed by the pelvis, the role of the sphincter (closing muscle) is played by the ureteropelvic segment. In the ureter, the detrusor of each dynamic section is the corresponding section of the ureter, and the sphincter is cavernous-like vascular formations. The sequential contraction of the overlying cystoids and relaxation of the underlying cystoids ensures the gradual movement of a portion of urine into the bladder.
The peristaltic theory denies the presence of cystoids and explains the process of urination by the peristaltic activity of the ureter, which depends on diuresis (see). With low diuresis (up to 3-4 ml/min/1.73 m2 of body surface), a discrete type of urination occurs, which is carried out as follows. The accumulation of urine in the pelvis is accompanied by an increase in pressure in it. When the pressure reaches a critical level (10-12 cm water column), the ureteropelvic segment opens and fills with urine. The resulting stretching of the walls of the segment generates a peristaltic wave, which spreads along the ureter in the distal direction at a speed of 4.5 cm/sec and is accompanied by a consistent rise to 18-40 cm of water. Art. pressure along the ureteral canal. This process determines the movement of a separate portion of urine through the ureter. The repetition rate of peristaltic waves is 2-6 per minute. The transition to the perfusion type of urination occurs with diuresis. 3-4 ml/min/1.73 m2 body surface. In this case, the evacuated portions of urine are drained, and the renal pelvis, ureter and bladder communicate freely with each other. The perfusion type of urination is carried out due to the pressure gradient in the upper and lower urinary tracts. The pressure in the ureteral canal reaches 40 cm of water. Art. and more. The speed of transition from discrete to perfusion type of urination under the influence of water load or diuretics is used to assess the functional state of the upper urinary tract.
Urodynamics of the bladder (see) and urethra (see) is characterized by two phases. In the first phase, urine accumulates in the bladder to a threshold volume of 200-400 ml at low (10-15 cm water column) intravesical and high (80-90 cm water column) intraurethral pressure. Low intravesical pressure is associated with adaptation (relaxation) of the detrusor, while high intraurethral pressure is created by contraction of the smooth muscle internal and striated external sphincters, muscle tone of the urethra and pelvic floor. A negative vesicourethral pressure gradient ensures urine retention in the bladder.
Achieving the threshold volume, i.e., the volume at which urination occurs (see), is accompanied by depletion of detrusor adaptation and an increase in its muscle tension. This leads to an increase in intravesical pressure and at the same time to relaxation of the urethral sphincters. The second phase of U. begins—emptying the bladder and evacuating urine into the urethra. The voiding phase is assessed by micturition pressure (pressure in the bladder during urination), urine flow rate and resistance in the urethra.
Victory pressure characterizes the force of contraction of the detrusor and ranges from 50 to 85 cm of water. Art. It does not depend on the initial bladder volume and the patient’s age.
The most accessible characteristic of urine flow for determination and analysis is volumetric velocity. This indicator is directly dependent on the amount of urine excreted at one time: with a volume of up to 200 ml, the volumetric flow rate is 14-24 ml/sec, with a volume of more than 200 ml - 25-35 ml/sec.
The volumetric flow rate of urine is regulated by the functional cross-section of the urethra, which, in turn, depends on the muscle tension of the detrusor: the larger the initial volume of the bladder, the higher the muscle tension of the detrusor, and therefore, the larger the effective cross-section of the urethra and the volumetric flow rate urine. Victory pressure does not have a significant effect on the volumetric flow rate of urine.
The most important indicators of the U. phase of emptying include resistance in the urethra, which reflects the loss of energy by the flow of urine as it passes through the urethra. Energy loss depends on the length, diameter, roughness of the canal, urine viscosity, flow turbulence and, according to Gleason (D. M. Gleason, 1976), is 50-70% in men and 30-50% in women.
In 1976, V. S. Ryabinsky and V. F. Savin, to characterize the U. of the lower urinary tract during the emptying phase, proposed another indicator - the energy efficiency of urination, or the efficiency of urination, which is the ratio of the pressure of the stream of emitted urine to micturition pressure. Patients have chronic with pyelonephritis without urinary tract obstruction, the efficiency of urination ranges from 39 to 64%.
A frequent violation of urine in diseases of the genitourinary organs is the reverse flow of urine (see Reflux). With a significant and sudden increase in intrapelvic pressure, as well as with patol. changes in the vault of the calyxes, pelvic-renal refluxes occur - the reverse flow of the contents of the pelvis into the renal parenchyma with its subsequent penetration into the venous or lymph. net. Pelvic-renal refluxes play an important role in the pathogenesis of inflammatory kidney diseases and can cause resorptive fever and acute pyelonephritis.
Vesicoureteral reflux can be congenital or acquired (secondary). The occurrence of congenital vesicoureteral reflux is caused by a malformation of the muscular layer of the terminal ureter. Secondary vesicoureteral reflux occurs in diseases that impair the passage of urine from the bladder and the tone of its muscular wall - sclerosis of the bladder neck, urethral stricture, cystitis, tuberculosis of the bladder, adenoma and prostate cancer, etc.
The most severe U. disorders develop when there are obstacles to the flow of urine along the urinary tract due to the presence of stones, valves, cicatricial narrowings, tumors, accessory vessels, etc., which are most often found in the ureteropelvic, vesicoureteral, and vesicoureteral. urethral segments. If an obstruction to the flow of urine occurs at the level of the ureteropelvic and vesicoureteral segments, a sign of U.'s disorder is a gradual transition to an irreversible perfusion type of urination. This is manifested by an increase in the capacity of the sections of the urinary tract located above the obstacle, an increase in hydrostatic pressure in them, and inhibition of the contractile activity of smooth muscles. The occurrence of an obstruction at the level of the vesico-urethral segment is accompanied by an increase in resistance in the urethra. Against this background, secondary structural and functional changes in the detrusor arise, having three stages of development: functional disorders, compensation and decompensation. The stage of functional disorders is characterized by normal voiding pressure and low volumetric urine flow rate; compensation stage - increased voiding pressure and normal volumetric flow rate; stage of decompensation - increased voiding pressure due to the inclusion of extravesical emptying forces (tension of the muscles of the anterior abdominal wall) and low volumetric flow rate of urine.
The study of the upper urinary tract is carried out using excretory urography (see), television pyeloureteroscopy (visual observation on the TV screen of the contrast dynamics of the ureter and the renal cavity system), radioisotope renography (see Radioisotope renography), ureteromanometry (see Catheterization of the urinary tract) , electroureterography (see Ureter, research methods). To study the U. of the lower urinary tract during the phase of urine accumulation, retrograde cystometry (see Bladder), electromyography of the urethral and anal sphincters (see Electromyography), and urethral profilometry (graphic recording of pressure throughout the entire urethra) are used. The bladder emptying phase is assessed using direct cystometry, uroflowmetry (see), electromyography of the urethral and anal sphincters.
Bibliography:
Derzhavin V. M. et al. Urodynamics of the upper urinary tract with vesicoureteral reflux in children, Urol. and nephrol., N° 2, p. 11, 1982; Pytel A. Ya. Pelvic-renal refluxes and their clinical significance, M., 1959; Ryab and a certain V.S. and Savin V.F. Urodynamic flowmetry for diseases of the lower urinary tract in men, Urol. and nephrol., N 1, p. 34, 1976; Boyarsky S. a. Laba R. Principles of ureteral physiology, in the book: The ureter, ed. by H. Bergman, p. 71, NY ao, 1981; Campbell W. A, Interpretation of pediatric urodynamics through bladder work calculation, J. Urol., (Baltimore), v. 94, p. 112, 1965; Gleason D. M., In ott and with cini MR as D rach GW Urodynamics, ibid., v. 115, p. 356, 1976; Rankin J. T, Concepts of urethral resistance, Brit. J.; Urol., v. 39, p. 594, 1967.
V. M. Derzhavin, E. L. Vishnevsky.
Laparoscopic partial nephrectomy for a large tumor
Patient B.
, 54 years old.
Diagnosis:
cancer of the left kidney T3aN0M0. Kidney cysts.
Clinical manifestations of the disease:
none.
Brief medical history:
During a preventive examination in a clinic at the place of residence, ultrasound data revealed a mass formation in the left kidney measuring up to 43 mm. At her place of residence, the patient was offered nephrectomy, which she refused. She was hospitalized as planned for surgical treatment.
With ultrasound
in the upper segment of the right kidney, anechoic formations with a maximum size of up to 16 mm (cysts) are detected. In the middle segment of the left kidney, a volumetric echo-heterogeneous formation with clear, even contours measuring 43×36×39 mm (tumor) is visualized. In the projection of the lower segment of the right kidney, multiple anechoic formations with a maximum size of up to 10 mm (cysts) are determined. Kidney mobility is preserved.
Ultrasound: Tumor of the right kidney
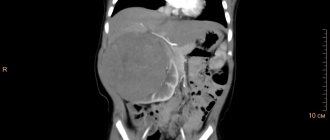
MSCT of the abdominal organs with contrast
in the middle segment of the left kidney, a space-occupying formation of inhomogeneous soft tissue density, measuring 42×44×40 mm, is determined. After IV contrast, inhomogeneous accumulation of the contrast agent is observed. The tumor occupies the entire thickness of the parenchyma, protrudes beyond the outer contour of the kidney, reaches and is closely adjacent to the posteromedial surface of the spleen, the border between these structures is not clearly visible throughout. In both kidneys, a few cysts ranging in size from 3 to 16 mm are detected.
MSCT: Tumor of the middle segment of the right kidney
MSCT: Tumor of the middle segment of the right kidney
According to computer modeling (3D)
pathological process: the left kidney is supplied with blood by two renal arteries, the outflow of blood is carried out through 2 renal veins. The accessory renal artery is located behind the main renal artery. The tumor grows into the renal sinus and is adjacent to the middle group of calyces.
3D modeling. The right kidney is supplied by two renal arteries. The tumor is closely adjacent to the calyces.
According to dynamic renal scintigraphy
The storage and excretory function of the kidneys is preserved, the urodynamics of the pelvis of the left kidney are impaired.
With osteoscintigraphy
no bone metastases were found.
In order to rid the patient of a kidney tumor and prevent the progression of the tumor process, a laparoscopic atypical resection (ennucleoresection) of the left kidney with a tumor . During resection, both renal arteries were temporarily clamped. Warm ischemia time is 16 minutes.
The postoperative period was without complications. Antibacterial and anti-inflammatory therapy was carried out. The emergency drainage and urethral catheter were removed on the 2nd day after surgery. Control ultrasound revealed no pathological changes. On the 4th day the patient was discharged home.
The removed part of the kidney with a tumor.
Kidney tumor in section.
Histological conclusion
– clear cell renal cell carcinoma of moderate differentiation without invasion into the perinephric tissue.
Dynamic observation is carried out.
Surgeon
- Ph.D. Pshikhachev Akhmed Mukhamedovich.
Why calcifications form in the kidneys: necessary treatment and diet
The kidneys are a vulnerable organ that is susceptible to various infections, injuries and colds.
Therefore, it is necessary to constantly monitor their health and immediately engage in treatment if any problems arise.
The kidneys remove all excess substances from the body with urine, cleansing it of unfavorable compounds, so the stability of their work is important.
Experts recommend periodically undergoing routine tests and ultrasound examinations of the kidneys.
Features of calcifications
When metabolic processes are disturbed, calcium salts - calcifications - are deposited in the renal parenchyma.
These are the most common stone-like formations, which are areas of dead kidney tissue covered with a dense sediment of calcium salts.
They are formed in the zone of infiltration inflammation.
Often the development of calcifications is observed with concomitant diseases.
Kidney stones can be detected in adults and newborns (regardless of age and gender).
Causes
Salts are removed from the body along with urine. When metabolic processes are disrupted, unwanted components accumulate in the kidneys, turning into stones without proper treatment.
They can occur in the form of calcifications - deposits of calcium salts that are deposited on the walls of the kidneys, disrupting their functions.
There are a large number of factors that can provoke kidney calcification. This manifests itself when the urinary system is dysfunctional or inflamed.
Often formations are detected in women during pregnancy, in the placenta. The cause of their appearance may be intrauterine infections. Also, the presence of deposits may indicate impaired blood circulation in the placenta.
That is, stones signal unfavorable processes or poor-quality treatment of diseases.
If there is a massive accumulation of calcifications, you should undergo a high-quality diagnosis and consult a doctor to prescribe therapeutic measures.
Diseases are provocateurs
Basically, calcifications develop due to inflammation of the kidneys - glomerulonephritis. Also, a similar pathology can manifest itself after untreated or recently suffered kidney tuberculosis.
These types of deposits are formed due to tabulopathy, Graves' disease, cystinosis, vitamin D deficiency, renal failure, and pyelonephritis.
Kidney calcification is typical for athletes who consume large amounts of protein.
In this case, there are no symptoms of kidney damage, and the pathology can be identified as a result of a medical examination and ultrasound examination.
Types of deposits
The condition characterizing the appearance of calcifications in the urine is called nephrocalcinosis, which can be primary or secondary:
- With impaired development and congenital diseases of the urinary organs, when the tubules are affected (tubulopathy), calcium loss occurs in the area of the papillae and the filtration processes deteriorate. This phenomenon is called primary nephrocalcinosis, it is characterized by calcium deposits in the proximal region of the nephron.
- Secondary nephrocalcinosis is formed during sclerosis, ischemic necrosis of renal tissue as a result of a tumor process or vascular pathology. Sometimes it occurs due to mercury poisoning or excess drugs (ethacrine diuretics and amphotericin B). In this case, calcium accumulates in all parts of the nephron.
Features of the clinical picture
The disease can be asymptomatic (if calcification does not reduce the filtration capacity of the kidneys and there is no obstruction of the ureter).
In other situations, symptoms of kidney calcification are:
- general malaise;
- disruption of the gastrointestinal tract;
- constipation;
- itching;
- pain in the joints;
- rapid fatigue;
- dizziness;
- decreased appetite and sleep.
These symptoms are associated with blockage of the urinary tract by stones.
Also, small urates and mucus may be detected in the urine. A large formation can block the lumen in the ureter, causing severe pain and blood in the urine.
With a large number of calcifications and with an increase in their size, the following symptoms appear:
- copious and frequent urination;
- pain in the lumbar region;
- more yellow skin tone;
- swelling of the limbs;
- unpleasant odor from the mouth (due to the accumulation of urinary toxins in the blood);
- dehydration of the body, strong and unquenchable thirst;
- increased blood pressure;
- an increase in the amount of protein in the urine.
Diagnostic methods
The doctor can determine the deposition of certain deposits in the kidneys using an x-ray examination.
Due to the fact that the consistency of the stone is similar to bone, a dense stone-like formation is clearly visible on the x-ray.
A more detailed study can be carried out using magnetic resonance or computed tomography. In this case, the exact parameters and location of the calcification are determined.
In the early stages, a puncture biopsy is considered an effective research method, since pathological changes cannot be seen using X-rays and ultrasound.
Kidney ultrasound is required mostly to identify concomitant kidney diseases.
The doctor also prescribes blood and urine tests to determine the concentration of this component. An examination of parathyroid hormone and vitamin D levels is required.
A biochemical study of blood and urine is carried out, which reveals the presence of phosphorus and calcium, acid-base balance, alkaline phosphatase activity and the excretion of hydroxyproline in urine.
What can and should be done?
The main goal of treatment is to eliminate the factors that provoke kidney calcification.
To normalize calcium volume, the following methods are used:
- sodium citrate and bicarbonate are introduced;
- for alkalosis, sodium chloride (ammonium) is prescribed (to change the balance to an alkaline environment); for acidosis, potassium aspartate (citrate) is administered (to change the balance to an acidic environment);
- B vitamins;
- diet with limited intake of calcium ions into the body.
Nutritional Features
Diet for kidney calcifications is of paramount importance.
To reduce the intake of calcium in the body, the consumption of sunflower seeds, mustard, and sesame is limited.
You should also not eat:
- hard and processed cheeses;
- halva;
- feta cheese;
- almond;
- condensed milk;
- yeast;
- wheat flour and bran;
- walnuts and nutmegs;
- dill;
- parsley;
- poppy;
- legumes;
- milk;
- garlic;
- oatmeal;
- sour cream;
- cottage cheese;
- black bread and cabbage.
The main nutrition corresponds to treatment table No. 7 (to reduce extractive components and accelerate the removal of toxins).
Salt is excluded, cilantro, cinnamon, citric acid, and cumin are added to the diet.
The following measures are also used to remove salts:
- the use of diuretics and herbs (but the volume of fluid does not increase);
- the use of anti-inflammatory drugs, since excreted salts cause pain, irritating the mucous membrane.
Preventive measures
There are no basic principles for the prevention of calcinosis, since there are many reasons for the appearance of the pathological process.
But doctors advise timely and comprehensive treatment of inflammatory and infectious diseases.
You need to monitor your diet by consuming high-quality foods and monitoring the composition of drinking water. You also need to lead an active lifestyle.
The recovery period depends on the stage of the pathological process.
Basically, in the initial stages, therapy becomes effective, but as renal failure develops and progresses, severe complications can develop with the appearance of uremia, which without surgery can lead to death.
What is renal microlithiasis and how is it treated?
Kidney microlithiasis is the initial stage of urolithiasis, in which small stones form. This pathology is characterized by the appearance of pain in the lumbar region, frequent urge to urinate and other symptoms.
Causes
Kidney microlithiasis occurs for a number of reasons, including:
- Heredity. Genetically determined metabolic disorders provoke active salt deposition.
- Chronic pathologies affecting the gastrointestinal tract and genitourinary system. Such diseases disrupt the functioning of the kidneys and bladder, so they are not able to remove deposits from the body normally and in a timely manner.
- Congenital anomalies in the structure of the pelvic organs, which causes frequent stagnation of urine.
- Bone pathologies. Disturbance of the bone structure leads to an increase in calcium levels in the body.
- Regular fluid intake in small volumes. This results in less urine being produced.
- Regular consumption of foods that increase the acidity of urine, which provokes the active growth of some types of kidney stones.
- Living in a hot and dry climate. Such conditions provoke active sweating, due to which the urine becomes more concentrated, and microliths begin to precipitate.
- Excessive consumption of foods high in salt.
Main symptoms
Symptoms of microlithiasis in the initial stages practically do not manifest themselves. Because of this, most patients seek help from a doctor when the disease has become advanced. Microlithiasis of both kidneys often provokes the development of salt diathesis. And the treatment of the latter disease is a rather complex process.
Symptoms of microlithiasis manifest themselves as:
- Pain syndrome. It is usually localized in the lumbar region, but can radiate to the perineum and lower abdomen. Pain often occurs when walking. In this case, it is noted in the sacral and lumbar regions.
- High pressure.
- Frequent urination. With renal microlithiasis, urine becomes dark in color. There may be small blood clots in it.
- Edema affecting various parts of the body.
- Deterioration in health, weakness during physical activity.
Treatment options depend on the chemical composition of the salt deposits:
- Urats. They are crystals obtained from uric acid salts.
- Oxalates. Appears when there is an excess content of oxalic acid.
- Phosphates. They are formed when the permissible norm of phosphate acid is exceeded.
Diagnostic methods
Diagnosis of microlithiasis involves the following measures:
- Urinalysis, which determines the level of salts, the presence/absence of pathogenic microflora and other parameters.
- Blood analysis. It allows you to find out whether inflammatory processes are occurring in the body caused by repeated infection.
- Blood chemistry. It is carried out to identify the nature of metabolic disorders.
- Ultrasound. Ultrasound is the main tool in the study of kidney lesions.
- X-ray exposure. A contrast agent is injected into the body, with the help of which the stones appear on the machine. The disadvantage of this method is that some microlites remain hidden from this type of radiation.
Treatment Options
To avoid serious complications, when the first symptoms of renal microlithiasis appear, you should seek help from a doctor.
Treatment of microlithiasis involves following a special diet and taking medications. Medicines are selected depending on the type of salt deposits. In addition, drug therapy involves taking drugs that have antispasmodic and diuretic properties. They are prescribed to facilitate the process of removing microliths naturally.
If the disease is complicated by infection, treatment is supplemented with drugs whose action is aimed at suppressing foci of inflammation and pathogenic microflora.
Good results in treatment can be achieved using traditional medicine methods. They include regular intake of decoctions and infusions that have diuretic and anti-inflammatory properties.
Diet therapy
A prerequisite for effective treatment of microlithiasis is adherence to a special diet. Like drug therapy, diet selection depends on the type of salt deposits:
- Phosphates. It is necessary to exclude or limit the consumption of fruits, vegetables and dairy products. They can be replaced with meat, fish, and flour products.
- Urats. Avoid consuming foods rich in calcium. Recommended: boiled meat, fish, eggs, butter and a variety of cereals.
- Oxalates. You should exclude foods containing oxalic acid: sorrel, strong coffee, potatoes, green salad, and so on. Recommended foods: bread, milk, berries, fruits, pasta, eggs and cereals.
Kidney microlithiasis is a disease that rarely causes discomfort to a person. This is primarily due to the fact that the initial stage of the pathology does not have characteristic symptoms. For more effective treatment, it is necessary to follow the doctor’s recommendations, follow a diet, and give up bad habits.