General information about oliguria
In this condition, an adult with an average body weight (women 60–65 kg, men 75–80 kg) secretes less than 400–500 ml of urinary fluid per day, which is not enough for the normal functioning of the body. In a healthy person, daily diuresis is about 1–1.5 liters. It is worth noting that measuring the exact amount of urine output in 24 hours is quite problematic, so there is a risk of error.
As for the reasons for the partial or complete absence of urine excretion, there are quite a few of them. The root causes are usually grouped:
- The first group is vomiting, diarrhea or profuse sweating (hyperhidrosis).
- The second group is the presence of diseases such as glomerulonephritis, renal failure, and renal vascular pathology. These are the most common reasons found in medical practice.
- The third group includes neoplasms in the bladder, stones in the body, pathologies of the prostate gland, cancerous tumors, and narrowing of the urethra.
- The fourth group is the use of medications for a long time.
- The fifth group includes injuries, poisoning with toxic substances, large area burns, and severely reduced blood pressure.
Some reasons may not be dangerous to health, while others may lead to serious consequences. In any case, if you produce a small amount of urine or have difficulty urinating (dysuria) for a long time, you should consult a specialist.
If you have been leaking a small amount of urine for several days without any discomfort, there is no need to worry too much. This phenomenon is transient in nature and is observed during physiological processes such as increased sweating in hot weather or drinking small amounts of drinks. If the urge to urinate has decreased, the disorder continues for more than 2 days, and there is a feeling of itching and burning, then you need to consult a doctor. He will order the necessary tests and prescribe antibiotics (for example, furosemide) or other therapy based on their results.
Changes in the amount of urine
Changes in the ability of the kidneys to concentrate and dilute, along with a disorder of water metabolism throughout the body, are often combined with disturbances in daily diuresis or the amount of urine excreted by the kidneys per day
.
Oliguria - decreased daily urine output
- can be of extrarenal and renal origin.
Oliguria of extrarenal origin
arise from a number of reasons:
1) general circulatory disorder
, accompanied by a decrease in cardiac output, a drop in blood pressure, congestion and, as a result, a slowdown in blood circulation in the kidneys themselves;
2) loss of large amounts of water by the body
due to increased sweating, increased breathing, uncontrollable vomiting, severe diarrhea;
3) water retention in the body
, for example, at the height of fever or swelling;
4) some lesions of the central nervous system
, in particular the areas of the hypothalamus and medulla oblongata, related to the regulation of water metabolism, as well as mental trauma;
5) reflex effects
from various parts of the gastrointestinal tract and skin (for example, with painful irritation).
Oliguria of renal origin
occurs with kidney damage of an inflammatory and dystrophic nature and is explained by changes in the renal tissue itself, which cause a slowdown in urine excretion or an increase in the process of reabsorption of water secreted by the glomeruli. In this case, urine has a higher specific gravity due to the increased concentration ability of the renal filter.
In the initial period of glomerulonephritis, blockage of the lumen of the tubules with cylinders or products of inflammatory infiltration, compression of the tubules due to swelling of the interstitial tissue, the occurrence of a blood clot or vascular spasm may occur. In all these cases, significant oliguria and even a complete absence of urination can be observed - anuria.
Anuria - short-term or long-term complete cessation of urination
. It occurs with acute glomerulonephritis and nephrosis. The nature and duration of its course, as well as the functional recovery of the kidneys, are different: in cases of nephrosis, recovery occurs more quickly than in vascular-inflammatory processes. Such anuria can be reproduced experimentally by poisoning the animal with sublimate or lead.
In addition to the purely renal form
anuria, anuria of extrarenal origin should be distinguished:
prerenal
- with reduced blood supply to the kidneys (due to decreased blood pressure, thrombosis or compression of the renal arteries or veins),
subrenal
- with blockage or compression of the ureters (stones or tumors),
reflex
- with injury, bruise or surgery on the urinary tract, etc.
Polyuria - pathologically increased daily urine output
low specific gravity and reduced percentage of constituent parts.
It can arise from the action of the following extrarenal factors: 1) changes in general blood circulation
in the form of increased blood pressure and increased blood flow and, as a result, the same change in blood circulation in the kidneys, causing increased urination;
2) metabolic disorders and accumulation in the blood of compounds that promote increased urination
, such as glucose (for diabetes), residual nitrogen (for protein metabolism disorders) or chlorine and sodium bicarbonate;
3) abundant intake of fluid into the body
, leading to a decrease in plasma colloid-osmotic pressure;
4) irritation of certain areas of the brain
- the hypothalamus, medulla oblongata and cortex, or as a result of the development of a conditioned reflex to increase urination.
Diabetes insipidus is a peculiar pathology of urination of a neuro-endocrine nature.
(diabetes insipidus). This disease, accompanied by prolonged polyuria, occurs mainly due to impaired water metabolism and decreased water reabsorption. Loading with sodium chloride increases polyuria in this disease, which can be noticeably pronounced even without load (5 - 20 liters per day). Polyuria is accompanied by polydipsia (increased thirst), which is a consequence of developing polyuria. This polyuria develops due to disorders in the diencephalon and insufficient production of antidiuretic hormone.
Polyuria due to kidney disease develops with a secondary and primary wrinkled kidney
.
In the first case, during different periods of development of the process, starting from the acute stage (glomerulonephritis) to the wrinkled kidney, fluctuations in the concentration ability of the kidneys can be observed: from its increase at the very beginning, followed by a gradual decrease to a sharp drop when the process transitions to the chronic stage.
Due to the weakening of the concentrating ability of the kidneys, urea and other nitrogenous substances or sodium chloride are retained in the blood, which can be removed from the body only with increased urination. Such polyuria
called
compensatory
, since it compensates for the insufficient ability of the kidneys to secrete dense substances. It is characterized by the release of urine of low specific gravity - hyposthenuria. This is due to the fact that the water secreted by the glomeruli is not sufficiently reabsorbed in the tubules due to atrophic processes developing in them (with a wrinkled kidney). The concentration of sodium chloride in the urine with a shriveled kidney is approximately the same as its concentration in the blood and even lower. The concentration of urea in the urine is also reduced, but compared to the concentration of sodium chloride, this decrease is not so significant. Polyuria in the initial stages of development of a wrinkled kidney, mainly due to a decrease in water reabsorption, compensates for the insufficient ability of the kidneys to secrete dense substances.
Types of violation
In medicine, there are several types of oliguria, distinguished depending on the pathogenesis:
- Prerenal – manifests itself with decreased renal blood flow, vomiting, diarrhea, hyperhidrosis.
- Renal - develops as a consequence of severe renal pathology, with glomerulonephritis, pyelonephritis, nephritis, and sometimes with cystitis. It also occurs due to kidney injury or taking medications. Manifests itself as a complication after burns, sepsis, trauma or previous operations.
- Postrenal (obstructive) occurs with tumors, stones, i.e. obstruction of the urinary tract. Men have little urine and rare urination occurs as a consequence of prostatitis or prostate adenoma.
Why is oliguria dangerous? The thing is that it can lead to more serious consequences - anuria, when fluid ceases to be excreted from the body. In this case, diuresis is less than 50 ml per day. Such a long delay in urine excretion becomes dangerous to health and requires emergency care.
Causes of urinary incontinence:
- Disease of the spine and spinal cord;
- Spinal injuries;
- Neurogenic bladder;
- Bladder tumors;
- Severe chronic inflammation of the bladder (for example, tuberculosis);
- Urinary incontinence also occurs when the anatomical structure of the female genital organs is disrupted: - prolapse of the vaginal walls; - prolapse and prolapse of the uterus;
- Difficult, protracted or rapid labor;
- gynecological interventions (hysterectomy, removal of interligamentous tumors);
- Endourethral surgeries;
- Backbreaking physical labor;
- Perineal injury;
- Severe inflammatory diseases of the female genital organs;
- Diseases of the prostate gland in men (prostatitis, adenoma).
What is anuria?
The condition is characterized by a small volume of urine (value less than 50 ml/day) or a complete cessation of excretion. Usually the problem lies in the ureters, since it is the disruption of their activity that makes it difficult for urine to enter the bladder.
Absence or decreased urination occurs when:
- removal of a kidney or congenital absence of this organ;
- hemolysis, myolysis;
- glomerulonephritis, pyelonephritis, including chronic, nephritis;
- the presence of stones that interfere with the outflow of urine;
- acute heart failure;
- hemorrhagic fever;
- tumors;
- CRF (chronic renal failure);
- poisoning with toxic substances;
- intersection of the ureters during surgery.
Anuria is possible if there is an allergic reaction to any product/component.
Signs of pathology at first are often completely absent, then thirst, loss of appetite, nausea, and vomiting appear. Over time, a headache begins, drowsiness, fever are observed, and in rare cases a person can fall into a coma.
Anuria and its symptoms require immediate treatment, as it can lead to uremia, when protein metabolites accumulate in a person's blood. This condition can be fatal in some cases.
Determining the risks and degree of danger of anuria is carried out using ultrasound examination of the urinary tract and a general blood test. Patients also undergo computed tomography of the retroperitoneal space and cystoscopy; such diagnostics provide the clearest prognosis for the development of the existing pathology. The doctor prescribes diuretics, a nephrostomy, and in severe cases, transfers the patient to an artificial kidney for a long time.
Diagnostics
Diagnosis and treatment of the disease is carried out by a urologist. After collecting anamnesis, he is authorized to refer the patient for appropriate tests to determine the cause of urinary retention and provide qualified assistance.
First, the specialist feels the patient’s lower abdomen. In this way, he can determine what exactly the patient suffers from: ischuria or anuria. And if we are already familiar with the symptoms and causes of ischuria, then the absence of urine is called anuria, when urine does not enter the bladder.
Once the doctor determines the nature of the disease, he can refer the patient for the following tests to clarify the causes of the disease:
- CBC (complete blood count).
- OAM (general urinalysis).
- blood biochemistry.
- Ultrasound of the kidneys and bladder.
- Ultrasound of the prostate (for men).
A complete blood count can show the number of blood cells: red blood cells, white blood cells, platelets, and erythrocyte sedimentation rate. Why is a general blood test performed? When a person is healthy, the quantitative composition of blood cells does not change, and other indicators (neutrophils, basophils, lymphocytes, etc.) also do not go beyond the established norm. However, if there is an inflammatory process or other disorders in the body, the composition of the blood changes. Thus, by the quantitative composition of the blood, the doctor can determine the nature of the patient’s disease.
If kidney, bladder, or prostate diseases are suspected, a general urine test is prescribed, which is designed to show the transparency, color, smell, and chemical composition of the patient’s urine.
A biochemical blood test will allow the doctor to assess the quality of work of internal organs such as the pancreas, kidneys and liver.
Ultrasound (ultrasound) will help the specialist evaluate the appearance and condition of the internal organs. Thus, ultrasound of the bladder allows you to diagnose:
- stones and sand in the bladder;
- inflammation of the mucous membrane;
- the presence of various foreign bodies in the bladder;
- abnormal structure of the bladder.
Ultrasound of the prostate is prescribed for suspected prostatitis and other diseases of the genital organs in men, due to which the outflow of urine may be impaired. An ultrasound of the prostate is performed through the rectum using a special device, the length of which is no longer than the index finger: this avoids discomfort during the procedure.
Urinary disorders in pregnant women
Low urine output during urination in women is often observed during pregnancy - almost every expectant mother faces this problem. As the fetus begins to develop, it puts pressure on the internal organs. In urology, there are two types of delay: complete and incomplete.
Incomplete is characterized by a decrease in the volume of urine excreted. A small part of it comes out, and a large part remains in the urine. If the disorder is not corrected in time, it can become chronic. At the same time, a woman may not notice any problems, especially in the first trimester. Signs of pathology in later stages, especially in the morning, include uncontrolled fluid secretion (which causes the underwear to become wet), as well as pain during bowel movements, when urine begins to come out in a thin stream.
Complete retention is the absence of urine, even when you may want to go to the toilet for a long time. In this case, the pregnant woman experiences sharp pain in the lower abdomen, sometimes itching, which intensifies with movement, especially in the morning. Added to this are headaches, nausea and vomiting. Swelling often appears.
Possible causes of dysuria in pregnant women:
- pressure on organs from an enlarged uterus;
- chronic diseases, such as kidney problems;
- sedentary lifestyle;
- stress that led to bladder spasm.
A dangerous disorder is intoxication, which threatens both mother and child. To establish an accurate diagnosis and prescribe treatment, tests and ultrasound are performed. Then the doctor recommends treatment (including medications) that can solve the problem.
Bladder training
Bladder training involves three main components: training, creating a voiding plan, and executing it.
The main point of the training is for the patient to comply with a pre-established urination plan agreed upon with the doctor, that is, the patient must urinate at certain intervals. Over the course of several years of illness, patients develop a peculiar urinary stereotype, which consists of the desire to empty the bladder when even a slight urge occurs. This desire is due to the fear of possible urinary incontinence, which may occur in an inappropriate environment.
A bladder training program aims to progressively increase the interval between urinations. In this case, the patient should try to urinate not when the urge to urinate occurs, but in accordance with his individual plan for the day. On this day, patients must restrain the urge to urinate through strong contraction of the anal sphincter.
Treatment with a bladder training program usually lasts several months. It is recommended to increase the interval between urinations by half an hour every 2-3 weeks until a time period of 3-3.5 hours is reached.
Bladder training is most often carried out in combination with drug treatment. By the time the course of drug therapy, usually lasting 3 months, is completed, a new psychological stereotype of urination should be formed. Stopping the medication as a consequence should not lead to a resumption of frequent urination and urinary incontinence.
Bladder training is prescribed to all patients with urinary disorders.
In patients with severe intellectual impairment and lack of lower urinary tract control and urinary incontinence, it is recommended to use a specially adapted “prompted voiding” technique. It consists of three main stages:
At the first stage, it is necessary to teach a mentally retarded patient to note the conditions when he is wet due to urination in bed, and when he is dry.
If the goals of the first stage are successfully achieved, you can begin the second stage of treatment. The most important task in this case is to teach the patient to perceive the urge to urinate and let others know about it.
The goal of the third stage of training is for the patient to achieve complete control over urination. It is noted that it is very effective when treating this category of patients to encourage them in some way at each stage of treatment.
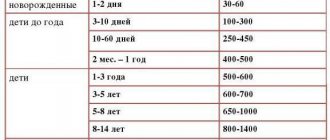
Reducing diuresis in children
A child's diuresis depends on the amount of fluid he drinks per day and sweating. The norm is indicated in the table (ml/day):
| Child's age | Average daily urine volume, ml |
| 1 month | 250-450 |
| 1–2 years | 500-600 |
| 2–5 years | 600-700 |
| 5–9 years | 650-1400 |
| 10–11 years | 1000-1400 |
An older child excretes more than 1 liter of biomaterial per day. To determine the norm, it is best to compare the amount of fluid consumed and excreted; approximately ¾ of the serving of previously consumed drinks should leave the body.
Partial release of urine is typical for diarrhea, vomiting, and the appearance of edema. The daily volume of urine output can decrease with large blood loss, acute nephritis, or blockage of organs with stones.
As for newborns, in the first few days of their life they urinate 4 to 6 times a day in small volumes. This phenomenon is observed in 99% of infants. That is why transient oliguria is considered normal and is observed in all healthy children in the first days of life. In this case, it is worth paying attention to the color, smell of urine, and the general condition of the child, since any deviation from the norm can be a signal of the presence of glomerulonephritis, necrosis, sepsis, nephritis, tumor, or underfeeding of the baby.
What symptoms can you use to identify the disease?
The main symptom of polyuria is an increase in urine output over 2 liters . With different disorders, diuresis may vary significantly, the number of urinations may or may not increase.
In some patients with severe damage to the functions of the tubules, the daily amount of urine increases to 10 liters, while significant losses of minerals and water occur in the body.
But diabetic patients do not fall under this rule: their urine is high density, which is associated with glucose content.
The disorder has no further manifestations, and patients suffer from signs of the underlying disease leading to polyuria.
It is necessary to distinguish the signs of polyuria from cystitis - frequent urination and dull pain in the lower back. With cystitis, false urges bother you and a small amount of urine is released.
Urges with polyuria are also frequent, but the volume of urine significantly exceeds the normal daily value.
Diagnostics
Urinary retention in men cannot develop just like that, so the reasons must first be identified. Urinary retention can be determined during the first examination of the patient. When tapping the suprapubic abdomen, a dull sound is heard.
Diagnosis is carried out after first aid.
Diagnostic procedures for ischuria in men:
- Ultrasound examination of the pelvic organs.
- Excretory cystourethrography.
- Retrograde urethrography.
- Pyelography performed intravenously.
These methods allow you to make the correct diagnosis and carry out treatment.
Treatment
Treatment for acute urinary retention may differ between men and women. Thus, urinary obstruction in women requires immediate medical intervention, since the consequences can result in sepsis or infectious infection of the genital organs. During hospitalization, the first step will be to remove excess urine from the bladder. In case of acute retention, urine is released using a catheter. The procedure is performed while sitting in a gynecological chair. After emptying the bladder, the doctor prescribes treatment to the patient, which will be aimed at eliminating the cause of the disease.
Treatment of acute urinary retention in men also involves hospitalization and removal of urine from the bladder. To do this, use an elastic or rubber catheter, which is gradually inserted into the urethra. The procedure takes place in a lying position, on your back.