A disease characterized by the destruction of kidney tissue is called necrosis. A characteristic sign of dead cells appearing in an organ is its swelling due to the decomposition of proteins. Kidney necrosis occurs as complications after diseases, poisoning of the body with various substances, or injury.
The kidneys perform a huge number of important functions in the body, so any damage to them affects its functioning. The kidney is enveloped by adipose tissue, under which there is a muscle capsule connected to the general kidney system - the parenchyma. The outer layer of the kidney is the cortex, the inner medulla. The parenchyma is an interweaving of millions of tubules and glomeruli; its medulla forms pyramids (up to 12 pieces). At the top of the pyramid is a papilla that opens into the renal calyx. The collection of calyces form the pelvis. And from the pelvis through the ureteric canals, urine enters the bladder and is excreted.
Treatment
Initially, in the treatment of renal necrosis, they try to remove the root cause of the occurrence of this process. In most cases, antibacterial therapy is carried out, antispasmodics and analgesics are prescribed.
Depending on the type of necrosis, the following measures are carried out:
- In case of necrosis of the renal papillae, antispasmodics are prescribed first. To unblock the ureter, a catheter is installed. Antibiotics, blood thinners and immunostimulants are used.
- With cortical necrosis, blood flow in the brain tissue is restored. The patient is prescribed procedures using an artificial kidney machine. Antibiotic therapy is used to eliminate foci of infection.
- In case of tubular necrosis, the drugs used are adjusted, antibacterial drugs are prescribed, and procedures are carried out to cleanse the bloodstream and body of toxins.
In severely advanced cases, when medication and physical therapy do not help, surgical intervention is resorted to. The kidney is removed entirely or only the area affected by necrosis is removed.
If a blood clot is detected in the kidney vessels, removal does not occur; specialists use a special balloon to remove the blockage, and drug treatment continues.
Microslide O/20 – kidney abscess.
1. presence of a cavity in the kidney;
2. the composition of the exudate is a purulent, creamy mass. Tissue detritus from the inflammation site, microbes, viable and dead granulocytes, lymphocytes, macrophages, neutrophils, leukocytes;
3. pyogenic membrane at the border with the kidney tissue;
4. structure of the pyogenic membrane: granulation tissue shaft. Pyogenic capsule is granulation tissue delimiting the abscess cavity. It consists of 2 layers: the inner one consists of granulations, the outer one is formed as a result of the maturation of granulation tissue into mature SDT. The outer layer may be missing;
5. abscess along the course - acute in exacerbation of chronic pyelonephritis, accompanied by purulent discharge.
(Description) Well, the presence of an abscess cavity is quite clearly visible (it was slightly damaged during the preparation of the drug, so there is nothing “outside”). The abscess cavity is delimited from the rest of the kidney by an inflammatory shaft and a pyogenic membrane (can you see a pink stripe?)
This pyogenic membrane is granulation tissue. Typically, the pyogenic membrane consists of 2 layers: the inner one - the granulation tissue itself + the outer one (may be absent, for example, as here) - CT, which is formed as a result of the maturation of granulations.
In the abscess cavity there is pus (it lies outward, as it were, in the direction of the lower right corner), containing leukocytes (both living and dead), tissue detritus + macrophages can be found.
Enlarged photo - a clearly visible pyogenic capsule consisting of granulations + the contents of the abscess cavity (below!)
7. Microslide C/12 – “Radicular cyst (cystogranuloma).
1) general view of the cyst wall (in some fields of view there may be stratified squamous epithelium in the inner lining of the cyst wall.); 2) inflammatory infiltration of the cyst wall; 3) reticulate processes 4) granulation tissue; 5) fibrous tissue; 6) bone trabeculae; 7) accumulation of cholesterol crystals and xanthoma cells;
8.C/14 – “Leukoplakia of the oral mucosa.”
1. general appearance: hyperplasia of cells of the spinous and basal layers, multilayered squamous epithelium without keratinization; 2. parakeratosis and acanthosis; 3. lymphoplasmacytic infiltrates at high magnification in the lamina propria; 4. inflammatory lymphoplasmacytic, lymphoid infiltrates of the mucous membrane.
9.O/8 – “Papilloma”.
1) papillary growths of flat stratified epithelium and stroma;
2) flat multilayered epithelium of uneven thickness with strands penetrating deep into the dermis;
3) differentiation of layers is preserved in the epithelium: basal, spinous, shiny, granular, horny;
4) the stroma is loose, with excessive formation of blood vessels;
5) characterized by morphological atypism - tissue. Uneven development of stroma and epithelium with excessive formation of blood vessels.
Preparations for papilloma and condyloma are very similar. And the first sign by which we can distinguish them with the naked eye is the shape of the formation on the glass.
If condyloma is an elongated, cone-shaped formation, then papilloma is a “rounded” formation compared to condyloma, so to speak.
Now we look at the preparation microscopically.
We see papillary growths of the epithelium and stroma (let me remind you that the epithelium is a multilayered squamous keratinized one.
+ strands of epithelium go deep into the underlying dermis (not as pronounced as with condyloma, this is very clearly visible).
If you look closely, you can see how the blood vessels in the stroma of the papilloma are quite well developed (my mistake, I forgot to photograph them well).
+ if you look at a higher magnification, you will notice that the stroma is loose.
It should also be said that the epithelium retains its differentiation.
10. O/35 squamous cell carcinoma with keratinization.
1. tumor cells form complexes that grow into the fibrous tissue of the skin; 2. complexes consist of layers of atypical cells with signs of stratification (stratification); 3. the presence of extracellular keratinization (“cancer pearls”); 4. hyperplastic follicle; 5. Degree of tumor differentiation: highly differentiated
It should be said right away that this cancer has a high degree of differentiation.
As I understand it, this is largely indicated by cancerous pearls - foci of extracellular keratinization - concentrically located epithelial cells with a focus of keratinization in the center.
Here they are, cancer pearls. “Roundles”, which, as I said above, are concentrically located epithelial cells, and in the center there is keratinization. All this is located in the stroma of the skin, in fibrous tissue.
See the next 3 photos.
One cancer pearl.
11.Ch/125-“Fibrous bone dysplasia.”
1. general view of cellular fibrous tissue; 2. Osteoid islands; 3. proliferation of fibrous tissue; 4. accumulations of osteoblasts.
Fibrous dysplasia is a bone disease. Its essence is the replacement of bone tissue with fibrous tissue (FT).
The stroma of the formation is represented by fibrous tissue (FT).
Among it, like islands of bright pink-orange color, are bone tissue (trabeculae).
Here's a larger image. It can be seen that the trabeculae are constructed quite primitively.
In some places small (compared to the trabeculae of bone tissue) vessels are visible.
12. Microspecimen 0/58 – “Giant cell tumor” (osteoblastoclastoma).
1) fields of cellular fibrous tissue; 2) small osteoblast cells; 3) giant osteoclast cells; 4) accumulations of red blood cells in tumor tissue; 5) vessels of sinusoidal type; 6) foci of “tissue blood flow” containing hemosiderin; 7) proliferation of fibrous connective tissue.
13. O/80 - granulation tissue
1. layer of necrosis, impregnated with fibrin and leukocytes;
2. layer of numerous vessels (capillaries);
3. capillaries are located vertically to the surface;
4. between the vessels - loose interstitial substance, lymphocytes, leukocytes, fibroblasts predominate;
5. layer of fibroblasts and formed connective tissue;
6. wound healing proceeds through zones of reparative regeneration, healing by secondary intention.
O/80 – granulation tissue.
The granulation tissue is clearly visible at the bottom of the photo. It is located between necrotic tissue (the lowest pole of the photo of the specimen) and “living” tissue. Look at the bottom 3 photos.
High magnification. Once again: granulation tissue is visible from above, and necrosis is visible from below (“living” tissue has not entered).
In necrosis – inflammatory infiltration.
In the granulation tissue there is the formation of CT + fibroblasts (if you zoom in a lot, you can find them). + We see some of the vessels that are located vertically.
More vessels located vertically.
Between them there is a loose interstitial substance. This can be seen especially clearly in the very last photo.
14.O/164 - genital wart.
1. cone-shaped growths covered with flat stratified keratinizing epithelium;
2. flat multilayered epithelium is thickened with pronounced acanthosis (immersion of strands of flat epithelium into the dermis);
3. the stroma is loose, with a large number of newly formed capillaries;
4. diffuse inflammatory infiltration of the stroma; 5. The inflammatory infiltrate consists of plasma cells, lymphocytes and macrophages.
O/164 – Condyloma.
This is probably one of the simplest drugs along with papilloma. I’ll tell you right away how to distinguish them. Papilloma is small, looking at the glass with your eyes, not under a microscope, and condyloma is more elongated, similar to a “spike”.
Here, look at the photo.
Now let's look at the microdescription.
Firstly, the cone-shaped growths, which are covered with stratified squamous keratinizing epithelium, immediately catch the eye.
Acanthosis is quite well expressed - the immersion of the strands of the epidermis into the depths of the dermis (see the previous 2 photos) + the next, lower one.
This is the stroma of the condyloma. If we go down the cone-shaped formations to their bases, we will reach the stroma.
It is necessary to pay attention to the fact that the stroma itself is quite loose; a large number of vessels and capillaries immediately catches the eye. In some places, diffuse inflammatory infiltration is quite pronounced (especially in the 2nd photo below).
15.Ch/65 – miliary pulmonary tuberculosis.
1. multiple granulomas;
2. in the center of only individual granulomas there is caseous necrosis, because more time is needed for the formation of necrosis; the granuloma must form completely. Around the necrosis there are activated macrophages - epithelioid cells, forming a circulatory layer of varying thickness. The formation of a necrotic lesion is a staged process, macrophages cope with Koch’s bacillus up to a certain point, then there is a progression of invasion;
3. cellular composition of granulomas: epithelioid cells, giant multinucleated Pirogov-Langhans cells, lymphocytes;
4. in the alveoli around the granulomas there is serous exudate;
5. by etiology - established, infectious; according to the level of metabolism - with a high level of metabolism, active, productive; According to the cellular composition, it is epithelioid cell.
. Ch/65 – miliary pulmonary tuberculosis
Again, I’ll make a reservation in advance. There is a drug for fibrous focal pulmonary tuberculosis.
And sometimes it can be confused with miliary tuberculosis. For me, the main difference is that with miliary tuberculosis, the foci of granulomas are generally quite small and, as a rule, are located in groups (there will be a photo later, you can see it).
With fibrous-focal tuberculosis, the foci are larger than with miliary tuberculosis, approximately as large as 2-2.5 granulomas of miliary tuberculosis.
On the specimen we see a granuloma, in the center of which caseous necrosis can sometimes be detected.
Giant multinucleated Pirogov-Langhans cells can also be seen; at low magnification they look like dark purple large dots. If we zoom in, we will see that their nuclei are located along the periphery of the cell!
There should be serous exudate in the alveoli around the granulomas.
Foci of granulomatous inflammation (granulomas) are very clearly visible.
There are just tons of them here.
Can you see the purple dot closer to the center? Most likely, this is a giant multinucleated Pirogov-Langhans cell. You just need to zoom in and look to be sure. There are also a lot of them in the previous photos. In the center of the granuloma there is a slightly darker colored formation. In my opinion, this is a focus of necrosis, albeit a very small one.
Forecast
If renal necrosis is diagnosed early, the prognosis is favorable. All dead areas and areas are removed and they are scarred over a period of time. The patient continues to live his usual life, with some adjustments.
If detected late, the majority of cases require kidney transplantation. And in very advanced cases there is the possibility of death. Therefore, it is so important to monitor your health, undergo regular medical check-ups, and if you suspect the presence of any disease, contact your doctor.
Kidney necrosis
Kidney necrosis is the process of death of kidney tissue cells. As a result of research, it was found that kidney necrosis is characterized by swelling of cells and protein structures in them, followed by destruction (lysis).
Necrotic changes in the kidneys can occur as a result of severe intoxication with any toxic substances, as a result of the development of autoimmune processes in the human body. Quite often, the cause of kidney cell destruction is a decrease in blood flow in the organ itself. With a decrease in the degree of blood supply, ischemia and hypoxia of the cellular system of the kidney develop, and then cell destruction.
Impaired blood flow to the kidney may occur due to thrombosis of the renal vessels or obstruction of the urinary tract by a stone or neoplasm.
Often, kidney necrosis develops in pregnant women and women in labor; this occurs due to heavy bleeding from the uterine cavity or premature detachment of a normal or pathologically placed placenta.
In children, this pathology occurs against the background of a viral or bacterial disease as a complication of dehydration (with excessive vomiting or diarrhea).
Causes and symptoms of necrosis, outcome and prevention
Causes of necrosis
Necrosis is the irreversible cessation of the vital activity of cells, tissues or organs in a living organism, caused by the influence of pathogenic microbes. The cause of necrosis can be tissue destruction by a mechanical, thermal, chemical, infectious or toxic agent. This phenomenon occurs due to an allergic reaction, disruption of innervation and blood circulation. The severity of necrosis depends on the general condition of the body and unfavorable local factors.
The development of necrosis is facilitated by the presence of pathogenic microorganisms, fungi, and viruses. Also, cooling in the area where there is poor circulation has a negative effect; under such conditions, vascular spasm intensifies and blood circulation is further disrupted. Excessive overheating affects the increase in metabolism and with a lack of blood circulation, necrotic processes appear.
Symptoms of necrosis
Numbness and lack of sensitivity are the very first symptoms that should be a reason to visit a doctor. Pallor of the skin is observed as a result of improper blood circulation, gradually the skin color becomes bluish, then black or dark green. If necrosis occurs in the lower extremities, it is initially manifested by rapid fatigue when walking, a feeling of cold, and cramps. the appearance of lameness, after which non-healing trophic ulcers form, necrotizing over time.
The deterioration of the general condition of the body occurs from dysfunctions of the central nervous system, blood circulation, respiratory system, kidneys, and liver. In this case, there is a decrease in immunity due to the appearance of concomitant blood diseases and anemia. Metabolic disorder, exhaustion, hypovitaminosis and overwork occur.
Types of necrosis
Depending on what changes occur in the tissues, two forms of necrosis are distinguished:
· Coagulative (dry) necrosis - occurs when tissue protein coagulates, thickens, dries out and turns into a curdled mass. This is the result of stopping blood flow and evaporation of moisture. The tissue areas are dry, brittle, dark brown or gray-yellow in color with a clear demarcation line. At the site of rejection of dead tissue, an ulcer appears, a purulent process develops, and an abscess forms. upon opening, a fistula is formed. Dry necrosis forms in the spleen, kidneys, and umbilical cord stump in newborns.
· Colliquation (wet) necrosis - manifested by swelling, softening and liquefaction of dead tissue, the formation of a gray mass, and the appearance of a putrid odor.
There are several types of necrosis:
· Heart attack - occurs as a result of a sudden cessation of blood supply to a tissue or organ. The term ischemic necrosis means necrosis of a part of an internal organ - infarction of the brain, heart, intestines, lung, kidney, spleen. With a small infarction, autolytic melting or resorption occurs and complete tissue restoration occurs. An unfavorable outcome of a heart attack is tissue disruption, complications or death.
· Sequestrum – a dead area of bone tissue located in the sequestral cavity, separated from healthy tissue due to a purulent process (osteomyelitis).
· Gangrene – death of the skin, mucous surfaces, and muscles. Its development is preceded by tissue necrosis.
· Bedsores – occur in immobilized people due to prolonged compression of tissues or damage to the skin. All this leads to the formation of deep, purulent ulcers.
Diagnosis of necrosis
Unfortunately, patients are often sent for examination using X-rays, but this method does not allow identifying pathology at the very beginning of its development. Necrosis is noticeable on x-rays only in the second and third stages of the disease. Blood tests also do not provide effective results in investigating this problem. Modern magnetic resonance imaging or computed tomography devices today allow timely and accurate determination of changes in tissue structure.
Outcome of necrosis
The outcome of necrosis is favorable if there is enzymatic melting of the tissue, growth of connective tissue into the remaining dead tissue, and a scar is formed. The necrosis zone can become overgrown with connective tissue - a capsule is formed (encapsulation). Bone may also form in the area of dead tissue (ossification).
If the outcome is unfavorable, purulent melting occurs, complicated by bleeding. spread of the lesion – sepsis develops. Fatal outcome is typical for ischemic strokes. myocardial infarction. Necrosis of the renal cortex, necrosis of the pancreas (pancreatic necrosis), etc. etc. – damage to vital organs leads to death.
Treatment of necrosis
Treatment of any type of necrosis will be successful if the disease is detected at an early stage. There are many methods of conservative, gentle and functional treatment; only a highly qualified specialist can determine which one is best suited for the most effective result.
Acute tubular necrosis
In tubular necrosis, the epithelial tissue of the renal tubules is affected. In this case, there are 2 types of disease, depending on the causes:
- Ischemic necrosis is provoked by injuries, inflammatory processes, sepsis, shock, and low oxygen levels in the blood.
- Nephrotoxic necrosis occurs as a result of poisoning of tissues and cells by toxins, heavy metals, antibiotics, etc.
Acute tubular necrosis means mechanical damage to the renal tubules due to sloughing of the epithelium. This pathology damages the tubular cells themselves and is accompanied by an acute inflammatory process. The result is severe damage to the kidney tissue and changes in the structure of the organ, leading to kidney failure.
Symptoms of the pathology depend on the degree of organ damage. The most commonly observed signs are:
- coma;
- drowsiness;
- delirium (damage to the nervous system by toxins);
- swelling;
- weak urination;
- nausea, vomiting.
Prevention
Prevention includes the following measures:
- Maintaining normal blood volume and renal perfusion in critically ill patients.
- Avoid prescribing nephrotoxic drugs whenever possible.
- Carefully monitor renal function when using nephrotoxic drugs.
- Measures to prevent contrast-induced nephropathy.
- Monitoring blood sugar levels in patients with diabetes.
There is no evidence for the effectiveness of loop diuretics, mannitol, or dopamine in preventing ATN.
Diagnostics
To make a correct diagnosis, at the very beginning, the specialist collects an anamnesis, namely, clarifies a number of symptoms that are troubling the patient and concomitant pathologies, diseases, in particular, whether he suffers from diabetes or takes certain medications.
It is also mandatory to collect an anamnesis about previous surgical interventions and injuries, and whether there has been contact with poisons and toxic substances.
After collecting anamnesis, both urine and blood are collected and examined. If controversial issues arise in the study, the specialist prescribes an ultrasound of the kidneys and x-ray studies. Doctors may also conduct the following tests:
Consequences and complications
The consequence and negative complication of the pathology is the development of renal failure. In this case, the patient exhibits strong signs of intoxication and damage to other organs and systems occurs.
As medical statistics show, 7-8 patients out of 10 with this diagnosis die from blood poisoning, kidney failure, and problems with the cardiovascular system. If the pathology is not identified in a timely manner and a course of effective therapy is not prescribed, over time an organ transplant may be required, or the developing pathology will provoke death.
Characteristics of the pathology
With kidney necrosis, damage to cytoplasmic proteins is recorded, in which the cellular structure of the organ dies. The disease is diagnosed in people of different ages, including newborns.
The main causes of the disease include:
- infectious processes, sepsis;
- injuries, blood loss;
- placental passage during pregnancy;
- kidney rejection after transplantation;
- intoxication with chemical compounds;
- exacerbation of cardiovascular pathologies.
Depending on the location of the lesion, cortical, tubular, and papillary types of the disease are distinguished.
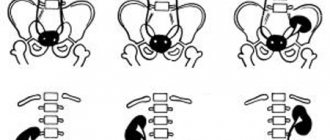
Cortical
A rarely diagnosed type of necrosis, in which the outer membrane of the kidney is affected, while the inner membrane remains intact. The cause of the pathology is blockage of small vessels that feed the cortex.
Kidney disease is manifested by the following symptoms:
- reduction or absence of urination;
- blood in urine;
- heat.
In addition, changes in blood pressure, as well as pulmonary edema, are possible.
Important! Endotoxic shock promotes centralization of blood flow, its deficiency, which causes necrosis of organ tissue.
The crusted appearance is often found in infants. This is explained by placental abruption, blood poisoning, and infectious processes. In women, in most cases, the disease manifests itself in the postpartum period due to uterine bleeding, infectious diseases, and compression of the arteries.
Papillary
Papillary necrosis is the death of the renal papilla. The functionality of the organ is impaired due to the destruction of the brain area.
By the way! In patients suffering from pyelonephritis, papillary necrosis is diagnosed in 3% of cases.
The acute form of the disease is manifested by colic, chills, and cessation of urination.
The causes of the pathology are:
- dysfunction of the blood supply to the brain and renal papillae;
- disruption of the outflow of urine in the pelvis;
- inflammatory phenomena, purulent formations in the organ;
- toxic poisoning of the tissue structure of the kidney.
The disease is more common in women.
Tubular
Tubular necrosis of the kidneys (acute tubular necrosis) is characterized by damage to the mucous membrane of the nephron tubules, which provokes renal failure.
Acute tubular necrosis occurs in two types:
- Ischemic. The pathology is caused by mechanical damage, sepsis, “oxygen starvation” of the blood, and inflammatory phenomena.
- Nephrotoxic. It becomes a consequence of severe intoxication of the body.
Acute tubular necrosis develops as a result of serious damage to the tubular epithelium, accompanied by intense tissue inflammation. As a result, the kidney structure changes, initiating organ failure.
Etiology of the disease
The main reason for the development of the disease is Escherichia coli, which penetrates through the papillae of the kidney through the mucous membrane of the pelvis by contact. Renal papillary necrosis can be unilateral or bilateral. The disease completely affects the performance of one or more papillae of the organ, gives it a pale color, and separates it from the adjacent tissue. In the affected papillae there is an ulcerative-necrotic process, an abscess, infiltration of leukocytes or sclerosis of the papillae. Additional development of the disease is facilitated by a surge in pressure in the pelvis and a circulatory disorder in the pyramids of the organ, which leads to the death of healthy cells and a complete disruption of the functionality of the organ and the entire system as a whole.
For information! According to statistics, only 3% of people suffering from pyelonephritis suffer from kidney necrosis.
The main reasons for the formation of pathology are:
- circulatory disorders in the brain;
- poor blood supply to the renal papillae;
- surges in blood pressure that interfere with urine output;
- the presence of ulcers and foci of inflammation in the brain part of the organ;
- intoxication of kidney tissue;
- circulatory disorders.
What is renal adenoma?
Kidney adenoma is a benign neoplasm. Diagnosed in 9% of patients, more often in men than in women. The tumor develops slowly, but if left untreated, it has the ability to increase in size and develop into a malignant one. The formation is small in size, up to 3 centimeters, has a dense structure and distinct edges. In most cases, it appears on one kidney, much less often - on two at the same time. In terms of external characteristics, the tumor is similar to a malignant form of glandular cell carcinoma of the kidneys. Therefore, many doctors and scientists believe that adenoma is a precancerous condition. Although this has not been officially proven.
Causes of occurrence in women and men
One of the causes of kidney adenoma may be polycystic disease.
Scientists have not yet been able to investigate the exact causes of kidney adenoma. It is believed that growth can be triggered by poor nutrition and insufficient fluid intake. The risk zone includes men over 40 years of age and smokers. And also people who, for one reason or another, are in constant contact with aggressive substances. For example, workers at chemical plants.
The appearance of tumors is also influenced by genetic factors. In many patients, adenoma develops against the background of inflammatory kidney diseases. Such pathological phenomena are often considered the cause of neoplasms: