Description
Clear cell adenocarcinoma of the kidney (hypernephroma) is a malignant epithelial tumor of the kidney, a type of renal cell carcinoma. Hypernephroma is manifested by local and paraplastic (general) symptoms: gross hematuria, pain in the kidney area, palpable tumor-like formation, deterioration of general condition, weakness, weight loss. To recognize hypernephroma and differential diagnosis, excretory urography, retrograde pyelography, renal angiography, ultrasound of the kidneys, CT and MRI are used, fine needle biopsy of the kidney. Treatment of clear cell adenocarcinoma is carried out in compliance with oncological principles and includes nephrectomy with lymphadenectomy, radiation and drug chemotherapy.
Hypernephroma
Additional facts
Hypernephroma (clear cell adenocarcinoma, Gravitz tumor, hypernephroid cancer) accounts for 2-5% of malignant neoplasms in general, and in urology - up to 85% of all cases of kidney cancer.
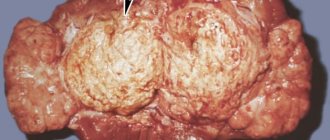
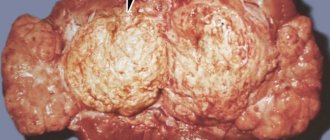
Hypernephroma refers to tumors of epithelial origin and can develop from almost any structure of the nephron: glomerular capsule, loop of Henle, distal and proximal tubules. In men, hypernephroma is detected 2.5-3 times more often than in women. In 2/3 of cases, hypernephroma occurs in patients aged 40–70 years. Hypernephroma is a softish node of variegated color with a pseudocapsule, microscopic examination of which reveals light polygonal and polymorphic cells containing lipids and numerous mitoses. Tumor cells unite into alveoli and lobules, merging into tubular and papillary structures. The stroma is poorly expressed, hemorrhages and tumor necrosis are typical. In 45% of cases, invasive growth of hypernephroma is detected, it invades the pelvis, and spreads in the form of tumor thrombi through the veins. Metastasis of hypernephroma is lymphogenous (to the lymph nodes) and hematogenous (to the lungs, contralateral kidney, liver, bones). The TNM stages of hypernephroma development are similar to those of renal cell carcinoma.
What is this
Hypernephroma or carcinoma is the most common type of kidney cancer. Despite the fact that the disease is quite serious, early diagnosis allows a complete cure. Regardless of what stage the diagnosis was made, the goal of doctors is to relieve the symptoms and ensure that the patient feels good during treatment.
Most people suffering from this disease are elderly people aged 50 to 70 years . It often begins as a small tumor in one of the organs, but it can also begin in two at the same time or with some time interval. The disease may also be called simply kidney cancer. Doctors have different ways of diagnosing and treating this disease, and every year, newer, more modern treatment methods appear.
Causes
The reasons for the development of hypernephroma remain unknown, but there are certain factors whose influence significantly increases the likelihood of kidney cancer. It is known that hypernephroma is detected 2 times more often in males and smokers. Smoking is considered the main risk factor for the occurrence of tumors of urological localization - bladder and kidney cancer. Meanwhile, quitting smoking leads to a reduction in this risk by 15% over 25 years. Various chemicals have an adverse effect on the renal epithelium: gasoline, asbestos, cadmium, organic solvents, herbicides, phenacetin-containing drugs, etc. It has been noted that the frequency of detection of hypernephroma correlates with diseases such as obesity, arterial hypertension, diabetes mellitus, as well as the pathology of the kidneys themselves (chronic pyelonephritis, nephrolithiasis, tuberculosis, dystopia, polycystic disease, nephrosclerosis, etc.). Patients with renal failure who are forced to undergo long-term hemodialysis are more predisposed to the development of hypernephroma. There is an increased risk of hypernephroma in patients with genetic pathology (Hippel-Lindau disease) and a family history (hereditary papillary cell carcinoma, hypernephroid cancer).
Causes of hypernephroma and risk factors
The exact causes of the pathology are unknown to medicine, but there are a number of factors that increase the likelihood of cancer. The risk of developing the disease is significantly higher in people who smoke.
In addition, cell degeneration most often occurs when:
- obesity;
- alcohol abuse;
- long-term use of cytostatics, hormones;
- radiation exposure;
- weakening of the body's defenses;
- long-term hemodialysis;
- unfavorable environmental situation;
- consumption of products containing carcinogens;
- exposure to cadmium, herbicides, gasoline vapors, organic solvents, and asbestos dust on the body.
Kidney cancer can be caused by drugs based on phenacetin. There is often a genetic predisposition to the disease. Moreover, men suffer from the disease more often not only because of addiction to alcohol and smoking.
Their risk of developing a kidney tumor increases with prostate disease. At the same time, in women, due to the similarity of the symptoms of kidney tumors with gynecological diseases, treatment is carried out late, which worsens the prognosis.
Also, the development of hypernephroma of the left and right kidneys is associated with the presence of other pathologies in the body. These include:
- disturbances in the functioning of the genitourinary system;
- endocrine dysfunction;
- kidney cysts;
- autoimmune diseases;
- tuberculosis;
- hypertension.
Hypernephroma of the right or left kidney may be associated with chronic pathology of this organ. Most often, the disease develops against the background of dystopia, polycystic disease, pyelonephritis, nephrosclerosis, glomerulonephritis, and urolithiasis.
Symptoms
Several years may pass from the onset of hypernephroma in the kidney to the development of the first clinical symptoms. The clinical picture of hypernephroma is characterized by the classic renal triad (hematuria, pain, palpable tumor) and extrarenal manifestations. The first thing that 2/3 of patients with hypernephroma usually notice is the appearance of blood in the urine (hematuria). As a rule, hematuria develops suddenly and is not accompanied by pain; may be transient, minor, total or profuse in nature. Frequently recurring or intense hematuria leads to severe anemia of the patient. In some cases, hypernephroma causes microhematuria, which can only be detected by urine examination. The formation of blood clots can cause ureteral occlusion and an acute attack of renal colic. Very characteristic of hypernephroma is the appearance of pain after hematuria, and not before it, as with kidney stones. More often the pain is constant and has a dull, aching character. Colostrum-like discharge from the nipples. Chills. Lack of appetite. Vomit. Nausea.
Prognosis and prevention
If kidney cancer was detected at an initial, operable stage, then with timely surgical removal and adequate therapy, the prognosis for recovery is high. In advanced cases, prognosis will depend on the general health of the patient, the degree of spread of metastases, and the prescribed course of therapy. Therefore, it is important to diagnose the disease in the early stages in order to save the patient’s life.
Prevention consists of following all the doctor’s recommendations, while it is important to carefully monitor your health, get rid of bad habits, and eliminate negative factors that can provoke a relapse. The patient needs to monitor his diet, adhere to the rules of a healthy lifestyle, harden himself, and engage in physical therapy. To monitor your health, you need to regularly undergo medical examinations, take urine and blood tests, and if characteristic symptoms occur, immediately seek medical help and not self-medicate.
Source: EtoPochki.ru
Diagnostics
Detection and differential diagnosis of hypernephroma requires a detailed urological examination, including excretory urography, retrograde pyelography, renal angiography, renal ultrasound, renal CT and MRI, fine-needle biopsy of the kidney and morphological analysis of the tumor. Already during the examination of the patient, characteristic asymmetry of the abdomen, increased venous pattern on the anterior abdominal wall in the form of a “jellyfish head”, dilation of the veins of the spermatic cord, and edema in the lower extremities can be identified. A clinical blood test reveals an increase in ESR, anemia, and polycythemia. A general urine test revealed erythrocyturia. To exclude the source of bleeding in the bladder (stones, diverticulum, tumors), cystoscopy may be necessary. At the first stage, ultrasound and Doppler ultrasound of the renal vessels provide information about the location and size of the space-occupying lesion and the likelihood of vascular invasion. Intravenous urography for hypernephroma reveals a deformation or defect in the filling of the pyelocaliceal system, pushing the ureter towards the spinal column. With a pronounced decrease in renal function and the impossibility of obtaining excretory urograms, retrograde pyelography is performed. To study the involvement of the renal vessels in tumor invasion, renal angiography and venography are performed. Using CT or MRI, the size and extent of hypernephroma are detailed, and enlarged lymph nodes are identified. For the purpose of preoperative morphological verification of the diagnosis and staging of the oncological process, a kidney biopsy or lymph node biopsy is performed to determine the histotype of the tumor formation. To exclude the possibility of hypernephroma metastases in distant organs, osteoscintigraphy, chest radiography, and liver ultrasound are performed.
Treatment
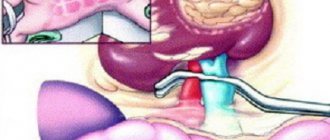
If hypernephroma is detected, surgery, x-rays, or systemic chemotherapy may be undertaken. If the function of the second kidney is satisfactory and the hypernephroma is operable, a radical nephrectomy is performed, including removal of the kidney with the adrenal gland, surrounding tissue and lymph nodes. At stage I of the tumor process (hypernephroma with a diameter of less than 7 cm, not extending beyond the capsule), poor functioning or absence of another kidney, a partial nephrectomy can be performed. If radical intervention for hypernephroma is not possible, arterial embolization can be undertaken, aimed at blocking the blood vessels of the kidney that feed the tumor. X-ray or chemotherapy for hypernephroma can be used alone or in combination with a surgical stage. Methods such as cryotherapy, radiofrequency ablation, HIFU therapy with high-energy focused ultrasound are of experimental value.
Treatment (methods, what and how)
In medical practice, there are several ways to treat kidney carcinoma. You may have to try several before finding one that works correctly.
The treatment plan is drawn up taking into account the stage of cancer, concomitant diseases and symptoms. Treatment methods include:
- Surgical removal of part or the whole kidney.
- Biological drugs that are used to strengthen one's own immune system to fight cancer cells.
- Chemotherapy and radiation exposure occur in conjunction with surgery.
- Vascular embolization - blocking the vessels feeding the tumor.
- Ablation is the effect of extreme cold waves on a tumor.
Many types of cancer are treated with radiation and chemotherapy. These procedures are usually combined with nephrectomy. In addition to all treatment, your doctor may prescribe medications or procedures to relieve associated symptoms and pain.
Clinics for treatment with the best prices
Price
Total: 117in 9 cities
| Selected clinics | Phones | City (metro) | Rating | Price of services |
| CELT on Enthusiastov Highway | +7(495) 788..show Record +7(495) 788-33-88 | Moscow (metro Shosse Entuziastov) | rating: 4.5 | 273400ք (80%*) |
| K+31 on Lobachevsky | +7(495) 152..show+7(495) 152-58-97+7(499) 999-31-31+7(800) 777-31-31 | Moscow (metro Prospekt Vernadskogo) | — | 289850ք (80%*) |
| JSC "Medicine" in 2nd Tverskoy-Yamsky Lane | +7(495) 152..show Appointment +7(495) 152-59-88+7(495) 229-00-03+7(495) 775-74-78 | Moscow (m. Mayakovskaya) | rating: 4.4 | 352160ք (80%*) |
| Military Medical Academy named after. S.M.Kirova | +7(812) 292..show+7(812) 292-34-35+7(812) 292-32-86 | St. Petersburg (metro station Lenin Square) | — | 69080ք (70%*) |
| Leningrad Regional Clinical Hospital | +7(812) 655..show+7(812) 655-89-27+7(812) 559-50-86+7(812) 670-55-82+7(812) 655-89-27 | St. Petersburg (m. Ozerki) | — | 75405ք (70%*) |
| Central Design Bureau No. 2 of JSC Russian Railways | +7(495) 727..show+7(495) 727-00-03+7(499) 187-08-17 | Moscow (metro station Rostokino) | — | 83190ք (70%*) |
| Medical center in 2nd Botkinsky Proezd | +7(499) 519..show+7(499) 519-37-39+7(495) 945-79-82+7(495) 653-14-57 | Moscow (metro station Begovaya) | — | 105663ք (70%*) |
| Medical center in 4th Dobryninsky Lane | +7(495) 933..show+7(495) 933-86-48+7(495) 933-86-49+7(499) 237-38-52+7(499) 237-40-04 | Moscow (metro station Dobryninskaya) | — | 105663ք (70%*) |
| DKB named after Semashko | +7(499) 266..show+7(499) 266-98-98 | Moscow (metro station Lyublino) | — | 106055ք (70%*) |
| KB MSMU im. Sechenov | +7(499) 248..show+7(499) 248-75-25 | Moscow (metro station Sportivnaya) | — | 151550ք (70%*) |
| * — the clinic does not provide 100% of the selected services. More details by clicking on the price. | ||||
Source
- Description
- Causes
- Diagnostics
- Treatment
Short description
Epidemiology. Kidney tumors in adults are found relatively rarely, accounting for 2–3% of all neoplasms.
The predominant age of patients is 55–60 years. Men suffer from kidney cancer 2 times more often. Cancer is registered in 80–90% of cases of all malignant kidney tumors. Incidence: 9.7 per 100,000 population in 2001. Code according to the international classification of diseases ICD-10:
- C64 Malignant neoplasm of the kidney, other than the renal pelvis
- C65 Malignant neoplasm of the renal pelvis
Causes
The etiology of kidney cancer is not well understood. The appearance of atypical cells is facilitated by chemical pollution of the environment, smoking, the use of hormonal drugs and cytostatics, irradiation, virus carriage, nitrosamines and aromatic amines. Hippel-Lindau disease and polycystic kidney disease have a high incidence of kidney cancer. Genetic aspects • There are several inherited forms of renal cell adenocarcinoma (• RCA1, HRCA1, 144700, 3p14.2; • VHL, 193300, 3p26 p25; • familial and sporadic, MET, 164860, 7q31; • type 1, PRCC, RCCP1, 179755, 1q21; • type 2, RCCP2, 312390, Xp11.2) • Associations of individual forms with some HLA haplotypes (Bw44, Dr8, W17) have been noted • Various chromosomal rearrangements have been recorded • There are associations with tumors of other localizations (pheochromocytoma - Lindau disease, multiple hamartomas - Cowden's disease [158350, PTEN, MMAC1, 601728, 10q23.3]). Morphology. Most kidney tumors are clear cell carcinoma (adenocarcinoma). The following histological variants of renal cell carcinoma are distinguished: • Clear cell alveolar • Granular (dark cell) • Spindle cell (polymorphic cell, sarcoma-like, aggressive carcinosarcoma) • Glandular (adenocarcinoma).
classification (see also Tumor, stages) • T0 - no signs of a primary tumor • T1 - tumor up to 7 cm in greatest dimension, limited to the kidney • T2 - tumor more than 7 cm in greatest dimension, limited to the kidney • T3 - tumor spreads to large veins or grows into the adrenal gland or perinephric tissues, but within the Gerota's fascia; T3a - the tumor grows into the adrenal gland or perinephric tissue, but within the Gerota's fascia; T3b - tumor spreads through the renal or inferior vena cava (below the diaphragm); T3c - the tumor spreads along the inferior vena cava above the diaphragm • T4 - the tumor spreads beyond Gerota's fascia • N1 - there is a metastasis in a single regional lymph node • N2 - multiple metastases in regional lymph nodes. Grouping of kidney cancer by stage • Stage I: T1N0M0 • Stage II: T2N0M0 • Stage III •• T1N1M0 •• T2N1M0 •• T3N0M0 •• T3N1M0 • Stage IV: •• T4N0M0 •• T4N1M0 •• T0–4N2M0 •• T0–4N0 –2M1. Clinical picture . Pain and hematuria are the first clinical signs, but most tumors are now diagnosed accidentally during ultrasound • The classic triad - palpable tumor, gross hematuria, lower back or abdominal pain - is recorded in the later stages of kidney cancer and is observed in only 5% of cases. Much more often, 1 or 2 of these symptoms are noted • Hematuria is the most common finding, observed in 70% of patients, and in 45–50% of patients, hematuria is the first symptom of the disease, blood in the urine appears suddenly, without warning or pain • Pain is noted at 60 –70% of observations • Increased body temperature can sometimes be the only symptom of a kidney tumor. Patients with fever of unknown origin should undergo a detailed urological examination • Weight loss (in 30%) • Malaise, night sweats and anemia (15–30% of patients) • Paraneoplastic syndromes: hypercalcemia, polycythemia and hypertension • Sudden onset of varicocele in middle-aged individuals and old age. Metastasis. Kidney cancer is characterized by pronounced vascularization and early metastasis to the lungs, bones, liver, brain and other areas • The tumor can metastasize to the paracaval, para-aortic lymph nodes and to the lymph nodes in the region of the renal hilum • More often, metastasis occurs hematogenously. In terms of metastasis damage, the lungs are in first place, followed by the liver, bones, and brain.
What to do after undergoing treatment for hypernephroma
Further monitoring by an oncologist and urologist is necessary. Scope of examination:
Ultrasound of the abdominal cavity and retroperitoneal space;- computed tomography of OBP;
- X-ray examination of the lungs;
- skeletal scintigraphy for bone pain;
- computed tomography of the brain with the appropriate clinic (headache, impaired consciousness, decreased visual acuity, etc.).
In addition, the levels of urea, creatinine, alkaline phosphatase, calcium, and a general blood and urine test are examined.
Important
The calcium level must be determined before starting treatment, this will increase the diagnostic value of the analysis after treatment and will allow timely prediction of the process of metastasis to the bones.
Victoria Mishina, urologist, medical columnist
8, total, today
( 26 votes, average: 4.65 out of 5)
Lymphoma - types, symptoms and treatment
Treatment of bladder diverticulum in children: causes, symptoms, therapy
Related Posts
Diagnostics
Diagnosis • OAM: detect hematuria • Cytological examination examines urine samples taken either after urination, or obtained during catheterization, or scrapings from the wall of the urinary tract taken during cystoscopy • Excretory urography is more accurate: they reveal a defect in the filling of the cups or a symptom of amputation •• B Further, the origin of the filling defect should be determined. It is necessary to differentiate uroepithelial tumor from X-ray negative stones. A filling defect can be caused by blood clots and necrotic renal papillae •• In approximately 30% of patients, the affected kidney is not visualized on a urogram (radiologically “silent kidney”). Radiologically, a “silent kidney” may be a sign of tense hydronephrosis, which can be easily confirmed by ultrasound or CT • Retrograde ureteropyelography: reveals defects in the filling of the renal calyces (dangerous with the possibility of infection); • Ultrasound: reveals a space-occupying formation (infiltrate that does not form a shadow). In addition, under ultrasound control, it is possible to perform a targeted puncture biopsy of the tumor • CT allows one to differentiate very dense urate stones from tumors. The density of the tumor shadow does not change after intravenous administration of a contrast agent • Ureteroscopy is an endoscopic procedure that allows for examination and targeted biopsy of the affected area in the ureter • Angiography of the kidney allows to detect the vascularization of the tumor •• Avascular tumors of the kidney - adenoma, adenocarcinoma •• Hypervascular tumors - clear cell carcinoma, polymorphocellular, dark cell •• Determine the deformation of the kidney and the configuration of the tumor, the depot of the contrast agent •• Detect the displacement of vessels by the tumor, arteriovenous fistulas, as well as arteries that additionally supply blood to adjacent tissues • A chest x-ray, bone scanning are indicated to determine metastases.
Treatment
Treatment. The only method of radical treatment is surgery. Chemotherapy and radiation therapy are ineffective. Basically, immunotherapy is used, which can achieve an effect in 30–35% of patients. • Surgical access during operations - laparotomy or combined access, depending on the extent of the tumor. • The scope of the operation is nephrectomy with removal of perinephric tissue, lymphadenectomy and revision of the renal vein to remove tumor thrombi (if any). The immobility of a tumor upon palpation does not always indicate the impossibility of its removal. For small tumors, or a tumor of a single (functioning) kidney, it is possible to perform organ-preserving operations •• In some cases, selective embolization of the renal artery is recommended, which makes it possible to stop life-threatening hematuria, followed by surgery. • In a relatively satisfactory condition of patients with single metastases to the lungs, their surgical removal is indicated. Observation • The purpose of observation is to identify a single curable metastasis • Follow-up studies include determining ESR, performing a blood test, determining the activity of ALT, alkaline phosphatase, creatinine concentration in the blood serum, OAM. Chest X-rays should be performed annually. Ultrasound, radioisotope bone scanning and other studies are carried out if necessary. Prognosis • Stage I. 5-year survival rate - 67%, 10-year survival rate - 49% • Stage II. 5-year survival rate - 59%, 10-year survival rate - 34% • Stage III. 5-year survival rate - 30%, 10-year survival rate - 19% • Stage IV. 5-year survival rate is 7%, 10-year survival rate is 2%. Synonyms • Renal cell carcinoma • Hypernephroma • Hypernephroid cancer • Gravitz tumor.
ICD-10 • C64 Malignant neoplasm of the kidney, other than the renal pelvis • C65 Malignant neoplasm of the renal pelvis
What threatens
Kidney damage from hypernephroma occurs more often in men, and mainly adults aged 40 years and older suffer from this disease; children are rarely at risk.
The growth of the tumor can reach gigantic sizes, ranging from 1–2 mm, the tumor can increase to the size of the head. In rare cases, both kidneys are affected; more often, hypernephroma affects only one right organ, and pathologies on the left side are recorded in only 30% of the disease.
The consequences of kidney hypernephroma are extremely dangerous due to the rapid development of this neoplasm in the body. Cells affected by this disease spread very quickly through the circulatory system to other organs. As a result, when metastases develop, they suffer:
- lungs,
- skeletal system,
- brain,
- intestinal tract,
- adipose tissue.
When metastases spread, their localization is observed in the lymph nodes and joints.
The absence of obvious symptoms and pain can complicate the timely detection of a tumor, and therapeutic methods will be powerless - surgery in advanced cases cannot solve the problem. Such complications are more often observed in women due to the similarity of symptoms of renal hypernephroma and uterine disorders.
When a neoplasm occurs in young people under 20 years of age, the following negative phenomena may occur:
- pseudohermaphroditism,
- macrogenitosomia,
- accelerated puberty in boys,
- girls may develop hirsutism,
- Women are characterized by manifestations of virilism.
Probability of death
The survival rate when the disease is detected in the initial stage and timely measures are taken to eliminate it is at the level of 80%. This rate is quite high for cancer, but is only possible with early detection. In the case of prolonged development of the tumor and spread of metastases to neighboring organs, the prognosis is disappointing - only 5% of patients can live for about a year, and the tumor in the last stage kills a person in a few months.
The harsh sentence imposed by advanced kidney hypernephroma can only be reversed with the help of regular preventive examinations.