Multicystic kidney disease is a disease in which healthy organ tissue is replaced by pathological tissue. A formation that is a small cavity with thin walls filled with liquid. The sizes of cystic formations are small - up to two centimeters, and large - 10 centimeters or more. The word "multi" comes from the Latin word "multum", which means multiple, multiplicity.
Most often, only one kidney is affected. Bilateral lesions are less common. With this urological anomaly, a diagnosis of polycystic disease is made, and the prognosis in such cases is not comforting - the child’s life lasts only a few days. Modern medicine makes it possible to save a newborn’s life; in some cases, permanent hemodialysis and even transplantation are considered. Provided that a sufficient amount of healthy tissue is preserved, surgery can be performed to remove the tumors and the patient will have a chance.
In most cases, the disease is congenital, but it happens that it develops after birth. Acquired cysts are safe, their oncogenicity is extremely low. The course of the disease with this pathology is asymptomatic.
Simple cysts include sinus and solitary cysts; if the formation is congenital, then it is likely that it can resolve on its own. A solitary cyst is not associated with the urinary system. Most often, it has a shape resembling a circle and does not have partitions in its cavity. When septa and inclusions form in the cyst cavity, this is a clear sign of the risk of it becoming malignant.
Symptoms and consequences of pathology
This disease is usually unilateral, and bilateral lesions are diagnosed in 20% of cases and are considered incompatible with life.
is formed as a result of a violation of embryonic development in the fourth to sixth week of gestation.
The basis of pathogenesis is atresia of the ureteropelvic junction during embryonic development. An incomplete fusion of the rudiment of the excretory apparatus with the rudiment of the secretory apparatus of the future kidney occurs. In addition, isolated development of the secretory apparatus of the kidney can occur with simultaneous complete agenesis of its excretory components.
In both cases, metanephrogenic tissue produces urine for some time, but it is not excreted, but accumulates in the kidney tubules, causing them to stretch and gradually transform into cysts. As for the size and shape of the cysts, they can vary; their walls are made of fibrous tissue, and between the cysts there is connective tissue; the ureter is poorly developed or absent altogether.
The abnormal kidney has no clinical manifestations and is diagnosed accidentally during an ultrasound examination. The absence of symptoms greatly complicates the preoperative diagnosis of the disease.
In some situations, with multicystic disease, some symptoms may appear, depending on the location of the lesion and its size. The most common symptoms include dull pain in the lumbar or hypochondrium area. An increase in blood pressure is also observed, sometimes total hematuria begins, and the tumor itself is detected as a result of palpation. But palpation should not be taken as a method for diagnosing this anomaly, because cystic formations can be confused with a real tumor or the lower segment of the kidney.
In the event of a breakthrough or suppuration of multicystic disease, severe unbearable pain begins, as well as inflammatory processes.
Often, cystic neoplasms on the kidneys can form without the influence of pathogenic factors on them, so they do not manifest themselves for many years. In this regard, the danger of this disease depends on the specific location of the lesion.
Diagnosis of polycystic kidney disease
When diagnosing polycystic disease, the patient's pedigree is taken into account.
An examination to verify polycystic disease is carried out using instrumental and laboratory methods.
Laboratory examination methods include:
- Detailed urine examination - samples according to Zimnitsky, Nechiporenko, Reberg, bacterial culture.
- Biochemical blood test - study of renal, liver and cardiac parameters (creatinine, urea, AST, ALAT, bilirubin, albumin, total protein, LDH, etc.), acid-base state of the blood.
Examination by instrumental methods is carried out primarily using ultrasound.
Minimum criteria for ultrasound diagnosis of adult-type polycystic kidney disease:
- Two cysts before the age of 30.
- Two cysts in each kidney – from 31 to 59 years.
- Four cysts in each organ in people over 60 years of age.
The dimensions of the organs with minimal criteria are normal, their surface is smooth and even. Accordingly, with the growth of cystic formations, the contour of the kidneys becomes lumpy and uneven. Cysts can reach sizes of 10 cm or more in diameter.
The adult type is characterized by larger cysts.
In addition to ultrasound, the following methods are used:
- MRI and multislice CT.
- Intravenous urography.
- Intravenous pyelography.
- Radioisotope research.
- Dynamic reoscintiography.
- Statistical nephroscintiography.
MRI is a fairly sensitive method for diagnosing adult-type polycystic disease.
Intravenous pyelography shows radial thickening of the collecting ducts that appear like “spokes of a wheel.” These extensions extend from the cortex to the parenchyma.
Diagnosis of malformations in the fetus is carried out using expert-level ultrasound and DNA diagnostics.
Ultrasound markers of polycystic kidney disease of the fetus or childhood type are:
- Increased kidney size.
- Low water.
- Impaired development of the biliary tract.
- Fibrosis of the portal vein system.
Intravenous pyelography is also used in children. If there is any doubt about the diagnosis, doctors conduct this study after reaching 12 months.
If an older child is diagnosed with polycystic disease, then he automatically becomes an “adult type”, since children with ARPP are able to survive in the vast majority of cases only on chronic dialysis or a kidney transplant.
The method of direct open biopsy of the kidneys and liver (surgical access) is also used.
Polycystic kidney disease is differentiated from the following diseases of the urinary system:
- Adult-type polycystic kidney disease must be distinguished from single renal cysts, tuberous sclerosis, and Hippel-Lindau disease.
- Childhood polycystic kidney disease is differentiated from hydronephrosis, Wilms tumor, and renal vein thrombosis.
In practice, doctors often have to distinguish polycystic kidney disease in adults from cystic dysplasia. Cystic dysplasia or multicystic kidney develops as a result of improper formation of the ureter during embryonic development. The ureter is located above its intended place, so its expansions during the process of growth are localized in the parenchyma. This disease is not related to chromosomal damage and the source of cyst formation is not the tubules.
Cystic dysplasia is a congenital condition in which kidney function is lost due to ureteral atresia. The kidney tissue is completely replaced by cysts from the ureter. The size can be huge, and the newborn’s belly will be greatly enlarged. Most often, one kidney is affected. A two-way process is incompatible with life. This diagnosis is made during pregnancy. The incidence is 1:2000 newborns.
Diagnosis and treatment process of pathology
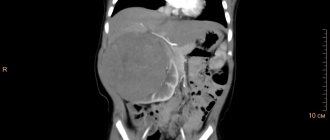
The most valuable diagnostic information for multicystic disease can be obtained through an ultrasound examination, which shows an increase or decrease in the size of the organ, and the renal parenchyma is almost completely replaced by numerous cysts of various sizes and shapes, which in some places are separated from each other by dense partitions.
Between the cysts there is connective tissue, and this may contain calcifications or cartilaginous components. In modern medicine, due to the use of antenatal ultrasound examination in diagnosis, the frequency of diagnosis of multicystic kidney disease in a child has increased significantly.
The question of whether to perform surgical intervention when a multicystic kidney is detected depends on the individual characteristics of the patient, usually this is the age group of children over the age of three years. But there are situations when a nephrectomy may be required immediately after birth. The main indications for surgery at this age are the large size of the multicystic kidney, ultrasound and clinical symptoms of suppuration of the cysts.
Danger of pathology
As possible complications of this disease, doctors identify:
- The pressure on nearby organs and nerve endings is increased due to organ damage, as well as pressure on blood vessels.
- The development of peritonitis if the pathological neoplasm ruptures and its contents spill into the abdominal cavity.
- Untreatable hypertensive condition.
- The risk of the cyst degenerating into a malignant tumor.
Treatment of pathology
Multicystic disease of the left kidney in the fetus or the right kidney causes a lot of controversy among doctors regarding treatment. Some experts believe that the treatment process for multicystic kidneys should only be surgical, that is, the implementation of nephrectomy. In this case, the main indication for surgical intervention is the difficulty of differentiating the tumor process before surgery, the possibility of complications of the anomaly through inflammation, renal hypertension, and the danger of rupture of cysts with thin walls due to injuries to the abdominal and lumbar areas.
Other experts are of the opinion that surgical intervention is required when a multicystic kidney is affected by any pathological process, such as urolithiasis, pyelonephritis, etc., accompanied by pain and increased blood pressure.
If a person has a second completely healthy kidney, the prognosis for the disease remains favorable. A particular danger arises when the diagnosis of multicystic kidney disease is incorrectly made when a patient develops polycystic disease in infancy or adolescence, because with this pathology, nephrectomy, that is, removal of the kidney, is prohibited. In this regard, doctors must be very careful about the manifestations of pathology in newborns and diagnosing them.
Multicystic kidney disease is a rare but very dangerous disease that negatively affects the health of the entire body. During the development of the pathology, the process of replacement of the renal parenchyma with tissue of cystic origin is observed, which is associated with multicystic dysplasia.
A dangerous disease that negatively affects the health of the entire body.
Prognosis for the disease
In most cases, with such damage to the designated organ, the prognosis for the patient is favorable, but only in the case when damage to one kidney occurs and a compensatory increase in the activity of the other. According to experts, paired organs have the ability to take on double the load. In this situation, treatment will consist of reducing the load on the second organ. Disability can be assigned to such patients in the case when a second organ is affected by a pathological process.
In practice, multicystic kidney disease detected at birth is observed by specialists until the child is 5 years old. By this age, the general trend in the course of the disease is already determined. In the case of a moderate course and absence of active growth of cysts, the patient remains under the supervision of specialists for life and is required to undergo regular scheduled examinations.
The relationship between multicystic kidney disease and life expectancy has not been fully studied to this day. There is no clear answer to the question of life expectancy with such a pathology. It all depends on the influence of accompanying factors and the presence of complications.
Description of the pathology
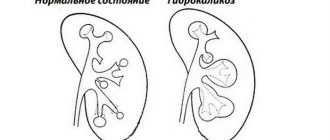
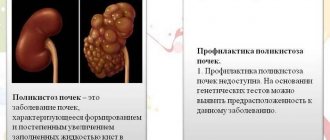
The structure of the kidney is made up of dense tissue with a small cavity - the pelvis. If the disease develops, the superficial membrane is affected by cysts filled with fluid. The organ in appearance becomes similar to a bunch of grapes. Its functionality constantly decreases, and over time, dysplasia provokes the replacement of healthy tissue with abnormal tissue.
With the unilateral type of multicystic disease, the disease does not manifest itself during the first years, but is diagnosed much later. In severe form, the pathology provokes damage to the liver and other organs. Abnormal changes begin to appear at the intrauterine stage of fetal development - during 4-6 weeks of gestation.
The risk of developing the disease is 1%, and in boys the risks are three times higher. At first, the organ looks normal, but over time it becomes overgrown with abnormal tissue. Babies with unilateral multicystic dysplasia will have a better chance of survival. If both kidneys are affected at the same time, then there will be no such chances. Therefore, if pathology is detected on ultrasound, doctors recommend terminating the pregnancy.
Essence of the disease
In practice, multicystic kidney disease is not detected very often. As the statistics presented show, such an anomaly accounts for only 1% of possible malformations of the paired organ. The baby's kidneys begin to form in the 3rd month of pregnancy. Under the influence of certain negative factors, a certain malfunction occurs in this process, as a result of which the departments that secrete urine, as well as the excretory tract, are unable to unite. Against the background of the fact that polycystic kidney disease has developed, it may happen that the renal pelvis is underdeveloped, and the child’s ureter remains without a lumen.
Due to the development of the pathological process, the paired organ, in fact, is a cyst or sac-shaped cavity with different diameters, filled with fluid and walls of connective tissue. If it happened that the organ did secrete urine that did not come out, then these cysts turn out to be filled with urine. A disease such as multicystic kidney disease is very actively discussed on forums.
Causes of occurrence in the fetus
It is quite difficult to speak with complete confidence about the reasons for the development of pathology, but most experts agree on a genetic predisposition. The anomaly occurs during intrauterine development of the fetus. It is usually more likely to occur in boys, with left-sided manifestations being more common.
If changes were detected on ultrasound, then in case of bilateral pathology and severe course, it is recommended to terminate the pregnancy.
After the baby is born, the disease usually does not become apparent until the age of 12. This is due to the slow development of the disease. However, an infectious or inflammatory shock can trigger the activation of pathology. It can be assumed that the provoking factor that can cause the development of multicystic kidney disease in the fetus is the influence on a woman in the first months of pregnancy:
- smoking habit;
- taking medications without consulting a specialist;
- stressful situations;
- poisoning with chemical components;
- lack of nutrients.
Cystic changes in adult patients can take various forms - polycystic disease, manifestations of a spongy kidney and a single cyst, multicystic and multilocular cyst.
Why does multicystic kidney dysplasia occur?
There is no exact scientific data on the preconditions for the anomaly yet. However, a hereditary predisposition is assumed. So, with multicystic disease in the family history of both parents, a congenital anomaly is possible. When inherited from one line, a pathology arises that develops gradually and reaches its apogee after adulthood.
The provoking effect of various negative factors on the expectant mother during pregnancy by the end of the first month cannot be ruled out:
- Bad habits,
- Chemical poisoning
- Taking medications
- Stress,
- Lack of necessary micro and macroelements.
.gif' data-lazy-type='image' data-src='https://parnas42.ru/wp-content/uploads/2019/08/rv0b44iu.jpg' alt='Heredity' width='589′ height ='392′ » data-'https://parnas42.ru/wp-content/uploads/2018/07/1218654.jpg 640w, https://parnas42.ru/wp-content/uploads/2018/07/1218654 -300×200.jpg 300w' sizes='(max-width: 589px) 100vw, 589px'>
The question of the causes of the development of the disease has been well studied. In an adult, pathology occurs due to insufficient outflow of urine from the kidney canals. Over time, the accumulated fluid provokes the formation of cysts that compress the ducts, further aggravating the situation.
Attention! Multicystic organs in the fetus can be diagnosed during pregnancy using ultrasound during the second screening study. In case of bilateral kidney damage or concomitant pathologies in other systems, doctors suggest terminating the pregnancy at any stage.
Why is multicystic disease dangerous?
Kidney dysplasia can cause adverse consequences for the body. Kidney failure, the transition of the disease to the purulent stage and rupture of formations create a threat of death. At the same time, the rapid growth of epithelial cells itself poses risks for the normal condition and development of other organs.
Early diagnosis of the disease can prevent complications, but if specialists are inattentive, multicystic renal dysplasia in the fetus sometimes goes unnoticed.
Attention should be paid to the unfavorable prognosis of the disease. As a result of the progression of the pathology, fluid stagnation is observed in the organ, which begins to actively increase in size. In such a situation, the risks of loss of functionality and failure are high. Bilateral damage is associated with a condition incompatible with life.
Course of the disease
In adults, multicystic disease is often detected accidentally during an ultrasound examination during treatment for another disease. A person with such a disease can live without knowing about the disease. There are often cases when congenital pathology is discovered only after death during an autopsy.
Multicystic dysplasia is predominantly asymptomatic. Pain appears in a child when the cysts increase in size. When palpating the abdomen, you can feel an irregularly shaped formation that is painful when pressed.
The child's blood pressure rises and stool changes. With a more favorable course of multicystic dysplasia, the diseased kidney shrinks, decreasing in size. The diseased organ does not function, and the entire urinary load falls on the healthy organ.
Symptoms
Kidneys develop in three stages, and if a deviation occurs in one of them, abnormal phenomena appear. At the final stage, there is a connection between the electic and secretory departments. If this does not happen, then a phenomenon called a multicystic kidney is observed. At the same time, there are often disturbances in the development of the pelvis and ureters.
The disease, if it was not detected by ultrasound during the prenatal stage of development, is unlikely to bother the baby for a long time. A small number of small cysts will not cause serious symptoms. But multicystic kidney disease in a newborn will begin to show some signs:
The tummy becomes lumpy.
- increase in the surface of the baby's abdomen;
- the tummy becomes lumpy, which is felt during palpation in the right or left part;
- touching the surface provokes pain and crying in the newborn;
- constant moodiness and poor appetite;
- problems with stool, manifested by changes in the color and consistency of stool;
- increase in pressure indicators.
Young patients are characterized by a state of general malaise with pain in the abdomen and lower back.
In adulthood, the symptoms become more distinct:
With hematuria, blood enters the urine.
- Paroxysmal unilateral pain in the lumbar region and side. They often radiate to the abdominal area.
- A state of general weakness, a feeling of malaise.
- Decreased volume of urine excreted.
- Manifestations of hematuria.
- Abnormal stool.
- High blood pressure.
If the provocateur is an infection, then signs of intoxication and fever appear due to the development of pyelonephritis - diarrhea with nausea and vomiting, chills, muscle and bone aches.
When purulent processes occur, the patient begins to complain of thirst, dry mouth, increased blood pressure, and swelling.
Symptoms of the disease
The disease often occurs in a latent form, and a multicystic organ reveals itself with a significant increase in the number of cysts and pressure on neighboring organs.
In newborns, pathology is detected:
- At an appointment with a pediatrician, but only in case of significant enlargement of the organ. Upon palpation, the doctor may feel the presence of a dense formation of a heterogeneous shape.
- During an ultrasound examination of internal organs.
The main symptoms of renal pathology:
- Pain in the lumbar region. It can be aching or sharp in the form of periodic attacks.
- Increase fluid intake.
- Slight increase in temperature.
- Increased blood pressure.
- Dizziness, lightheadedness.
- Stool disorders due to pressure on the intestines.
- The appearance of blood in the urine.
With the development of infectious processes, additional symptoms arise in the form of pain with frequent urination.
Further growth of the cysts leads to blocking of blood flow to the organ, and the kidney begins to atrophy.
Diagnostics
Research for the presence of pathology is carried out at the stage of intrauterine development. Thanks to the use of ultrasound in the period 21-23 weeks, primary signs can be detected in 90% of cases. The doctor identifies darkened cystic cavities in the kidneys. During the third screening, the extent of the lesion is assessed. Timely diagnosis helps to take corrective measures in time and, if necessary, terminate the pregnancy.
Ultrasound is performed after 3 days of the child’s life.
If the disease was not detected during fetal development, this can be done during the initial examination after birth. In modern conditions, ultrasound is performed after 3 days of a child’s life. However, even then it is possible that the disease will not manifest itself.
Suspicion of pathology appears due to the presence of diabetes mellitus, renal failure, and high blood pressure. Therefore, an additional laboratory analysis of urine is carried out - the presence of protein and red blood cells and their specific gravity are detected. Intravenous urography will be more informative. In some cases, a tissue biopsy is taken for histology.
For diagnostic purposes, adult patients undergo:
- palpation of areas where pain is present;
- Ultrasound to identify cysts and the condition of other organs;
- emergency urography with x-ray to assess organ performance;
- arteriography to determine the condition of the arteries;
- CT and MRI.
Detection of pathology
It is optimal to begin identifying pathology with screening of the expectant mother. This kind of research provides the opportunity to terminate a pregnancy if the defects found are incompatible with life. Multicystic disease in the fetus is detected during the second comprehensive examination. This corresponds to approximately 21 – 23 weeks. Ultrasound is highly informative. If there is a pathology, darkened areas will be visible on the screen. However, due to their insignificance, lesions may go unnoticed.
In cases where the family history shows a tendency to a cystic process on the organs of the genitourinary system, and the screening results are negative, primary diagnosis of the newborn is mandatory. It involves an ultrasound examination. But even with proper preparation, cysts may not appear. The first suspicions arise against the background of constantly observed high blood pressure, the development of diabetes insipidus and renal failure.
In cases where it is not possible to confirm the presence of a cystic process by ultrasound, urine biochemistry is prescribed. The disease is indicated by the appearance of protein, red blood cells, and their high specific gravity in the results. But the most informative method is intravenous urography.
Treatment
Timely diagnosis allows you to increase the effectiveness of therapy. The severity of the condition is taken into account. At the first stage, when symptoms do not appear and cystic formations are insignificant, monitoring the patient is recommended.
The second stage, when dysplasia is present but functionality is preserved, requires symptomatic treatment. Surgery is recommended only in cases of loss of functionality and active processes of replacement with fibrous fibers.
Multicystic kidney disease in adults and children is treated with surgery, usually during decompensation, when tissue destruction is observed. Sometimes doctors perform surgery at an earlier stage of pathology progression in order to prevent complications. But they do this not immediately after birth, but when the baby reaches 5 years of age.
Surgery can be performed in several ways:
- by pumping out fluid from large cysts using laparoscopy;
- removal of a non-functioning organ;
- kidney transplant.
If a baby is born with a bilateral pathology, then he is initially left in the clinic for observation and supportive therapy is used. In some rare cases, the baby survives, but the organ does not recover. Therefore, hemodialysis is subsequently performed and transplantation is prescribed.
If the condition is mild in children and adults, then maintenance therapy is prescribed:
- painkillers and antispasmodics;
- diuretics;
- preventing infections with antibiotics;
- using herbal uroseptics to prevent inflammation;
- compliance with dietary nutrition.
If cysts in the kidneys are detected in the early stages, it is possible to use herbal preparations to eliminate inflammatory processes, stimulate the outflow of urine and lower blood pressure. However, such approaches cannot replace a course of drug therapy prescribed by a doctor.
Treatment methods
Treatment tactics will depend on the degree of damage to the kidney tissue.
If both kidneys are not functioning
With bilateral development of the pathology, survival for a newborn is no more than 3 days. Such a diagnosis is incompatible with life.
If one kidney partially performs its functions, but renal failure develops, the only way to save life is to transplant an organ from a donor.
Attention! A donor organ from a living relative prolongs life by 20-25 years (from a deceased donor by 7-9 years), after which the kidney stops functioning for unknown reasons, and repeated surgery becomes necessary.
Organ transplantation into an adult is possible either from a relative or from a deceased person, provided that the blood type matches and the donor material is in satisfactory condition. As for children, they can only receive a kidney from a relative. Previously, operations were performed only on children whose height exceeded 1 m and weighed more than 20 kg. Since 2020, domestic doctors began to perform operations for children weighing over 7 kg with placement of the organ in the abdomen. The method is safe, as evidenced by 40 years of foreign practice in operating on patients in the first year of life.
Prevention
After surgery, patients must follow preventive measures to exclude infectious and inflammatory processes in the genitourinary system.
It is important to adhere to such recommendations;
- follow a diet;
- avoid hypothermia;
- avoid the toxic effects of chemical compounds and toxins;
- limit physical activity;
- follow your doctor's advice.
Multicystic disease is a congenital pathology. It may involve one or more organs. There is a certain hereditary predisposition to the disease. If it occurs in one parent, then there is a high probability that the anomaly will develop with age. If both parents have a pathological abnormality, the newborn will become a carrier of a severe form of multicystic disease.
Candidate of Medical Sciences, mammologist-oncologist, surgeon
Multicystic kidney disease is a disease that can be diagnosed in both an adult and a fetus.
The disease develops slowly and leads to pathological changes and complete atrophy of the organ.
With a long course, multicystic disease can cause severe complications, reduce the size of the organ and lead to its complete atrophy, narrowing of the ureter and disruption of the outflow of urine.
Forecast
The prognosis for the course of the disease is unfavorable. Pathology leads to organ enlargement and fluid stagnation, which is fraught with serious consequences and the emergence of new diseases. A diseased organ may stop working over time. Its functions are completely impaired. If organs are affected on both sides, then a condition incompatible with life occurs.
If a multicystic kidney is removed during surgery, patients after surgery must follow preventive measures to prevent infectious processes in the urinary system. It is recommended to prevent hypothermia.
Basic information about the disease
Multicystic kidney disease is considered a rare disease.
In most cases, cysts form on only 1 paired organ. When the pathological process affects 2 kidneys, severe complications arise. Cysts block the outflow of urine; they occupy the kidney, growing on its surface. Dysplasia progresses slowly, but any inflammatory or infectious disease of the genitourinary system can accelerate its development.
In adults, the pathological process proceeds slowly and is diagnosed mainly during routine ultrasound. The problem is that if cysts form on the surface of one kidney, reducing its functional characteristics, then the second takes over the functions of the diseased organ partially or completely.
Cysts form on the surface, reduce the glomerular filtration rate, lead to narrowing of the ureter and blocking the outflow of urine. Urine stagnates in the body, which leads to an increase in blood pressure and disturbances in the functioning of nearby organs (the liver suffers the most).
But the most difficult disease to treat is in the fetus. In this case, the pathological process most often leads to death.
Classification and types
There are only 3 stages of disease development. This division into categories allows you to classify pathology and determine the extent of damage.
At the initial stage of development, pathological changes are completely absent or barely noticeable.
During this period, it is extremely difficult to identify the presence of pathological changes, even when carrying out differentiated diagnostics.
An assessment of the size of the organ will help to suspect the presence of multicystic disease.
One kidney will be larger than the other, which may be either a developmental anomaly or a sign of the presence of pathological changes.
At this stage of development, the disease progresses, changes affect organ tissue. There is a violation of the outflow of urine, the surface of the organ undergoes dysplasia. But the changes have a slight impact on the functioning of the entire organism. The kidney increases in size due to the accumulation of fluid.
The final stage of disease development. It is characterized by damage to 2 kidneys and nearby organs. Cysts lead to narrowing of the ureters, urine accumulates in the body, and there is a possibility of developing severe complications.
Causes
Multicystic disease develops slowly only in adults; the causes of its occurrence are still not fully understood.
Doctors argue about why the disease occurs; there are several reasons that can, to one degree or another, affect the growth and development of organs.
The disease is most often diagnosed in people of mature age; it has a direct connection with congenital developmental anomalies.
That is, to put it simply, a person is already born with multicystic disease, and different organ sizes may indicate this.
The affected kidney has smaller parameters; it gradually becomes overgrown with cysts and increases in size due to severe swelling.
But if everything is fine with the second organs, then it is extremely difficult to suspect the presence of pathological changes.
Multicystic disease in a child has the same cause as in an adult. That is, it develops against the background of a congenital anomaly.
If a child has suffered pyelonephritis, cystitis or another disease of an inflammatory or infectious nature, then multicystic disease can act as a complication.
Multicystic neonatal disease occurs due to genetic pathologies. That is, in the process of organ formation, certain changes occurred in the body (at the gene level). This leads to tissue dysplasia.
If multicystic disease was diagnosed in the fetus, then the cause of such an anomaly should be considered the presence of:
- genetic changes;
- severe pathologies of pregnancy.
If the disease was diagnosed in the fetus, and the pathological process affected both kidneys, then its viability is questioned. Cysts completely occupy healthy tissue, causing irreversible changes in the kidneys and nearby organs.
Characteristic features of multicystic kidney disease
Multicystic disease is diagnosed extremely rarely. With this disease, healthy tissue is gradually replaced by cystic formations. Due to the fact that the two sections of the organ are not connected to each other, urine, which is actively produced by secretory elements, is not evacuated. Because of this, the renal cavities begin to gradually expand. The surface of the kidney becomes covered with cysts, and connective tissue forms between them. Often the pathology is accompanied by developmental disorders of the ureters and renal pelvis, which may be underdeveloped or even completely absent. Even if the lesions are small in volume, the organ is not able to perform its functions.
Pathology can be of two types:
- One-sided. Over time, tissue degeneration causes the development of kidney failure. And this is not only disability in the future, but also a mandatory transplant.
- Double-sided. This example of multicystic dysplasia is the most severe and dangerous. If this kind of disease is diagnosed in the fetus during a routine or emergency ultrasound examination of the mother, a recommendation is made to terminate the pregnancy.
The disease progresses slowly. Acceleration can be triggered by an infectious or inflammatory pathology affecting the genitourinary system.
Due to the lack of amniotic fluid, compression of the fetus and, accordingly, its internal organs occurs. Kidneys are often affected and can dissolve if they have already begun to form. The defects also affect the pulmonary system, due to which children are born with severe pneumothorax, as a result of which they die within a few hours after birth.
Causes of appearance and stages of development
The etiology of multicystic disease is directly related to the age of the patient. Let us consider the important features of the process of formation of pathological renal neoplasms.
In early childhood
In some cases, the disease can be diagnosed during fetal development. Multicystic kidney dysplasia in the fetus has the following causes:
- genetic changes;
- pregnancy pathologies.
If the disease affects both kidneys, the viability of the unborn child is questionable. Cysts that occupy all healthy tissues cause changes not only in the kidneys, but also in nearby organs, which are irreversible. Even if the baby is born, its life expectancy will be no more than 3 days.
Multicystic kidney disease in a newborn develops due to genetic pathologies. When the formation and/or development of internal organs occurred in the fetus, hereditary disorders became more active under the influence of some factors.
In children who have not yet completed their development, pathology is diagnosed in the presence of a congenital anomaly. In this case, the child must have suffered cystitis, pyelonephritis or any other inflammatory disease. Accordingly, multicystic kidney disease in a child is its complication.
In adults
If the disease does not manifest itself before the age of 12, it is diagnosed in mature adults. In this case, the patient's condition is directly related to congenital anomalies. This can be suspected by the difference in the size of the kidneys.
The organ affected by the disease gradually becomes covered with cystic formations. Severe swelling affects the volume of the diseased kidney. All functions are performed by its second part. In the absence of provoking factors and inflammatory processes, the disease does not manifest itself for a long time.
Experts distinguish three stages of the pathological process. Knowing and understanding them helps to clearly classify the condition and determine the extent and extent of lesions.
First degree
The primary stage of development is characterized by the absence or inconspicuousness of pathological disorders. The disease will pass for some time without any changes in the patient’s health status. Even if differentiated diagnostics are prescribed, multicystic disease is difficult to identify. The only thing the doctor should pay attention to is the size of the organ. One bud will appear larger than the other. But this may be not only a sign of pathology, but also a consequence of abnormal development.
Second degree
By this stage, multicystic dysplasia of the left or right fetal kidney begins to progress. Organ tissues undergo significant changes. There are disturbances in the outflow of urine. However, the clinical picture does not yet greatly affect the functioning of the body. Due to the accumulating fluid, the organ affected by the cystic process begins to increase in volume.
Third degree
This is the final stage of pathology development. Patients have bilateral multicystic disease, which can also affect nearby organs. Growing cystic formations cause the ureters to narrow. Accordingly, urine begins to actively accumulate in the body. The patient's life deteriorates significantly.
Signs of manifestation
There are several specific symptoms of multicystic disease that will help recognize the presence of the disease. Such signs have varying intensity and, often, patients leave them without proper attention, thereby starting the pathological process.
The disease is asymptomatic for a long time. Nothing bothers the person. Pathological changes can be diagnosed only during a routine ultrasound.
In rare cases, when the pathology affects 2 kidneys at once, a number of characteristic signs are observed:
- pain in the lumbar region;
- decrease in diuresis volume;
- disturbance of urine outflow.
These symptoms can also be disturbing in other diseases of the urinary system, the cause of which is inflammatory, infectious or other pathological processes.
Infants may have the following symptoms:
- change in skin color;
- rare urination;
- the presence of compaction in the area of the affected organ.
Detecting a cyst is not so difficult when it comes to a newborn baby. You can simply palpate the area of his abdominal wall on the left side (most often the pathology affects the left kidney).
Multicystic disease has a certain resemblance to cancer, for this reason it is so important to differentiate the disease and promptly seek help from a specialist.
If we are talking about a child older than one year, then in the presence of cystic changes, the disease may occur with the following symptoms:
- pain in the lumbar spine;
- decrease in the amount of urine excreted;
- the appearance of edema;
- general weakness of the body;
- nausea, loss of appetite.
Symptoms appear if both organs are affected, and tissue dysplasia has led to an increase in their size.
Cysts block the outflow of urine and disrupt the filtration function. Which leads to certain changes in the body.
But if the disease affects only the tissue of 1 kidney, then the signs may be completely absent.
Polycystic kidney disease - what is it?
This anomaly of kidney development is a hereditary pathology of the urinary system. It is characterized by the replacement of the organ parenchyma with cysts of various sizes. This occurs as a result of a violation of the formation of the secretory department - the kidney tubules. The outflow of urine will become difficult, which leads to the expansion of the tubules and the formation of large cavity formations.
Stagnation of urine inevitably leads to compression of the parenchyma by growing cysts and infection of the cavities. Since the kidneys are the organs that regulate blood pressure, compression leads to a persistent increase in blood pressure. Complications such as pyelonephritis and urolithiasis are recorded most often.
The kidneys also produce erythropoietin, a substance that stimulates the formation of red blood cells, which is why anemia is observed in polycystic disease.
The most unfavorable outcome of the disease is considered to be chronic renal failure, as a result of which the patient is forced to be on constant hemodialysis. Persistent loss of organ function may lead to the need for organ removal and transplantation.
Modern methods of treating anomalies can prolong and make the patient’s life easier.
Who to contact and how to diagnose?
Diagnosis of the disease is carried out in several stages and is carried out with the participation of the following specialists:
After visiting a doctor, you will need to undergo a number of diagnostic procedures:
Urography is considered the most accurate and informative study. But it is carried out in the field of ultrasound, as a supplement.
You can confirm or refute the diagnosis made by a doctor using ultrasound diagnostics. But urography provides more information about cysts, their sizes and locations.
Methods of therapy
Conservative medicine is not effective in the treatment of multicystic disease, for this reason it is not carried out. Taking medications will not help get rid of cysts or reduce their size.
Surgery is the most effective; it is performed using several methods. The operation is performed on both children and adults.
There are 2 methods that will help get rid of cysts:
Laparoscopy is characterized by low trauma; it allows you to get rid of cysts and does not involve removing the kidney (only a certain part of it).
It is performed under general anesthesia and has a short recovery period.
But if it is not possible to remove part of the organ using laparoscopy, then open nephrectomy is used. If the tissues are not affected, the disease is just beginning to develop, but cysts have already appeared on the surface, then you can resort to puncture.
Using a puncture, the formation is opened and the fluid contained in it is taken for a biopsy.
If multicystic disease has been diagnosed in a child, then before the age of 5, surgery is performed only if there is a serious threat to the baby’s life.
Preference is given to puncture, with opening the cyst and collecting its contents. If the baby has reached the age of 5 years, then surgical interventions can begin.
Indications for surgical procedures are:
- presence of a pathological process;
- damage to only 1 kidney;
- no complications.
Multicystic disease is treated surgically only if it affects 1 kidney, progresses rapidly and threatens severe complications.
Otherwise, therapy is not required; doctors simply monitor the development of the disease and, if necessary, intervene in the process.
Due to ineffectiveness, it is not carried out, as is drug therapy. Taking herbal decoctions and plant extracts can negatively affect the patient's health.
Treatment Options
The choice of tactics to eliminate the disease is determined by its degree. In cases where the formations are insignificant, the well-being and functioning of the organ are not impaired, preference is given to drug treatment:
- antispasmodics - help reduce pain that occurs from time to time;
- diuretics – reduce blood pressure, improve urine flow;
- antibiotics – prevent and eliminate the infectious process;
- uroseptics – eliminate the likelihood of inflammation.
Patients must be prescribed a gentle diet. It involves avoiding spicy, smoked, fatty, salty and fried foods.
The operation is prescribed if, based on the test results, it can be assumed that there is extensive replacement of one’s own tissues with fibrous fibers, a large-scale loss of functionality. The intervention is carried out in three directions:
- Pumping out fluid that has accumulated in the largest cysts.
- Removal of the affected organ. In this case, the functions are taken over by a healthy kidney, most often the right one. Hemodialysis is mandatory.
- Transplantation.
When choosing the type of surgical intervention, the doctor is guided by the state of health, the number of cysts, and their size.
Prevention and prognosis
If the pathological process has reached the final stage of development and both kidneys are affected, then the prognosis directly depends on the speed of providing assistance to the patient. Often, surgical intervention allows you to completely restore the function of the affected organ.
As part of preventive procedures, it is recommended that once every 12 months you undergo a routine examination by a urologist and nephrologist, do an ultrasound, and have your urine tested.
Multicystic kidney disease is a rare and little-studied disease that remains asymptomatic for a long period of time. In order not to encounter manifestations of the disease, you should regularly visit a urologist and nephrologist, do an ultrasound or urography.
Diagnostic methods
Reliable data on the condition of the kidneys can be obtained already in the perinatal period (from the 22nd week of pregnancy). Ultrasound does not pose a risk to the development of the fetus, so you should not be afraid of diagnosis, but find out as early as possible about the development of multicystic kidney disease in your baby.
The procedure takes no more than 10 minutes. On the monitor, you can examine the structure of the organ, determine the number of cystic formations, their size, and location relative to other organs.
To check whether the kidneys are performing their functions, excretory urography (x-ray with contrast) is performed. Arteriography (x-ray of arteries with contrast) is used to study the condition of the arteries.
Additional research methods can identify tumors and vascular blockages.
Information about the functioning of both organs is provided by a general and biochemical urine analysis.