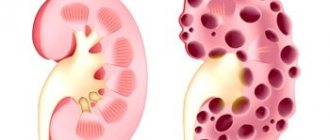
Renal cysts are common diseases and represent both benign and oncological formations. The Bosniak classification of renal cysts, proposed in 1986, is considered an effective technique according to which the degree of malignancy is determined. Data from diagnostic studies, including computed tomography, are taken as a basis.
The Bosniak classification allows for better examination of the pathology and selection of adequate therapy.
Signs of a malignant cyst
The most accurate method to determine the presence of a kidney cyst is histological examination. There is a list of additional signs that distinguish a malignant tumor from a benign one. Fundamental features in the classification of renal cysts according to Bosniak:
- density of formation is higher than normal;
- multiple formations in the cavity;
- calcium deposits on the walls like nodules;
- increased number of chambers in the cavity;
- accumulation of contrast agent;
- increased density of the walls between the partitions.
Signs are determined by imaging of the kidneys. The results obtained must be compared with the classification criteria and conclusions drawn about the degree of threat of the tumor to health. A correctly defined category according to Bosniak allows treatment to begin in a timely manner. If a mistake is made, there is a risk of developing cystic cancer.
Kidney cyst and its diagnosis
To detect this pathology, standard types of examination are used using instrumental diagnostic methods.
The success of therapy and further prognosis depend entirely on the timeliness of seeking medical help.
This allows you to identify the pathological process in the early stages and begin timely treatment, increasing the likelihood of recovery and reducing the risk of disease progression.
Late diagnosis and detection of cancer at the fourth stage cannot prevent death.
Detection of a malignant renal cyst is a difficult diagnostic problem, since the disease manifests itself with scanty symptoms or may be asymptomatic.
One of the signs of manifestation may be an unreasonable increase in blood pressure or the appearance of blood in the urine. To verify a renal cyst, the following diagnostic procedures are used:
- Ultrasound diagnostics is an informative, minimally invasive research method that allows you to detect small cystic formations.
Since cysts are aechoic structures, the density and intensity of the signal changes significantly when they are detected, which allows them to be easily diagnosed. The use of Doppler ultrasound allows one to assess the degree of influence of pathology on renal blood flow; Computed tomography is an X-ray diagnostic method that allows one to identify and differentiate oncological tumors. Single cysts have the appearance of rounded objects, their contours are smooth and even.
Inside there is a secret that differs in density from the surrounding tissues. Multilocular cysts are a conglomerate of cystic formations of different sizes.
The use of intravenous contrast makes it possible to differentiate oncopathology from cysts. This is possible due to the specificity of the blood supply to neoplasms, which allows the accumulation of contrast;
For example, studying the patency of the ureters during excretory urography; general clinical tests. A standard diagnostic procedure that allows you to evaluate the functions of organs and systems based on laboratory parameters. The method is not very informative for small cystic formations.
However, large cysts can be manifested by changes in the chemical composition of urine, which are detected during tests. Impaired kidney function can be manifested by the appearance of blood and excess protein in the urine.
Compression caused by the cyst causes a decrease in daily diuresis, the appearance of pain, and a feeling of incomplete emptying of the bladder.
Classification of cysts according to Bosniak
Kidney cysts can be simple (I Bosniak) or complex (II, IIF, III and IV Bosniak). Simple ones can form in the kidneys at any age. They differ in the presence of one chamber, which is filled with liquid. The likelihood of it turning into cancer is extremely low. Complex ones are characterized by the previously listed symptoms and have a high risk of malignancy.
Bosniak-I
When undergoing an MRI or CT scan, its single-chamber appearance is clearly visible. The category consists of simple cysts. They often form in the kidneys, but are not a threat. Typically characterized by a thin septum. The walls are free of thickening and salt deposits. Formations in this category do not require further observation or treatment because they are benign.
Bosniak-II
This includes simple cysts. Unlike the previous group, there may be slight thickening of the walls, as well as the presence of minor calcifications. During examination, several thin-walled septa may be identified. The group also consists of dense formations with clear contours less than 3 cm in size. They are benign and do not require treatment.
Bosniak-IIF
Seals are characterized by an enlargement of the cavity, thickening of the walls between the partitions, and nodular calcium deposits on them are possible. During the examination, the injected contrast is not visible. Cysts of uniform density and larger than 3 cm are also included in this category. They still fall under the signs of benignity, but already require observation. A small percentage of such formations are considered cancerous.
Bosniak-III
Formations with uneven thickening of walls and partitions, calcium deposits are uneven. During the examination, contrast may slightly accumulate. This includes those tumors that are difficult to clearly classify as malignant or benign. In any case, observation and surgery are required, since half of the cases are cancerous growths.
Types of kidney cysts according to Bosniak
Renal cysts are divided into several categories depending on morphology and risk of malignant transformation. Ultrasound and x-ray methods play a decisive role in diagnosis.
The Bosniak classification allows the attending physician to make the right decisions regarding the therapeutic approach. Classification depends on the degree of malignancy of the process:
- Bosniak I, II – no need for active therapy;
- Bosniak II F – examination and observation over time are indicated;
- Bosniak III, IV – surgical intervention is required.
Alexey Viktorovich Fedchenko - surgical oncologist, oncourologist
| Category | Character traits | Further tactics |
| I | A simple benign thin-walled cyst without septations, calcifications or solid component. The contents have a liquid density and are not contrasted. | Benign, no further observation required |
| II | Benign cyst. May contain several thin septa in which "apparent contrast" may be observed. There may be small or slightly thickened calcifications in the walls and septa. This group also includes formations of uniform high density ≤ 3 cm in size with clear contours that do not accumulate contrast | Benign, no further observation required |
| IIF (F–follow-up, dynamic observation) | These cysts may have many thin septa. There may be minimal uniform thickening, as well as “apparent contrast” of the walls or septa. They may contain calcifications, including wide and nodular ones, but there is no measurable accumulation of contrast. The contours are usually clear. This category also includes non-contrast-accumulating high-density lesions measuring > 3 cm and located entirely within the kidney | Dynamic observation. A small proportion of lesions are malignant |
| III | Questionable cystic lesions with uniformly or unevenly thickened walls or septa with measurable contrast uptake. Some are benign (hemorrhagic cysts, cysts with chronic infection, multilocular cystic nephroma), others are malignant (cystic and multilocular cystic RCC) | Surgery or follow-up. Over 50% of neoplasms are malignant |
| IV | Obviously malignant cystic formations that have all the characteristics of category III and, in addition, contain soft tissue components that accumulate contrast, adjacent but not associated with the walls or septa. These neoplasms include cystic carcinoma | Surgery recommended |
oncologist
Make an appointment with an oncologist in St. Petersburg
Treatment in the urological oncology department of the Leningrad Oblast Hospital
www.drfedchenko.ru
Bosniak IIF
Benign cysts, although in rare cases oncological neoplasms are detected, consisting of numerous thin septa or with slight thickening. Calcifications are deposited in the form of nodes, but the contrast does not accumulate. This group also consists of homogeneous, high-density formations measuring more than 3 cm.
The percentage of malignant transformation is still minimal, so surgery is not required, but constant monitoring is required.
What is the classification based on?
Kidney cysts can be simple or complex. The first type includes only one chamber with liquid. A widespread simple neoplasm has a low risk of malignant transformation.
Complex cysts are multi-chambered, with deformed and thickened walls, multiple septa, and significant signs of calcification. This type of pathological formation has some characteristics that make the disease dangerous.
The existing systematization makes it possible to divide neoplasms into categories depending on the likelihood of malignancy based on the morphological characteristics of cysts, which are determined during diagnostic studies. Further therapy depends on the classification degree.
Cysts are divided into four categories:
- Bosniak I is a simple neoplasm with a negligible risk of malignant degeneration.
- Bosniak II is a renal cyst with minimal complications.
- Bosniak IIF is a benign pathology that requires further study.
- Bosniak III is a neoplasm with an extremely high risk of malignancy.
- Bosniak IV is a malignant tumor that must be surgically removed.
On this topic
What are the symptoms of prostate adenoma?
To make an accurate diagnosis, histological examination is used. The choice of treatment depends on the presence of symptoms that help determine the category of cystosis. If formations of the first and second types are ignored, then cysts of the Bosniak IIF type are constantly observed and examined, and the third and fourth types are necessarily removed.
Despite accurate histology, there are some signs that help determine a simple or complex cyst and assess the degree of malignancy. A pathological formation is considered potentially dangerous if the following factors are present:
- Calcifications.
- Increased density.
- Partitions in the cavity of the neoplasm.
- Lots of cameras.
- Nodular seals of walls, partitions.
- Accumulations of contrast agent in a cyst.
- Thickened partitions, walls.
Nodular calcium deposits should be monitored for disease and removed if the walls are thickened with excessive calcification. An increased density of the cyst indicates the presence of blood in the cavity or an increased level of proteins in the fluid. Formations with thin and even septa are ignored, while those with thick, heterogeneous or nodular septa are removed.
If the cyst accumulates contrast, it should be eliminated, since this process leads to an increase in the density of the pathology. The same applies to all multi-chamber kidney lesions with three or more septa.
In the presence of small nodules that do not accumulate contrast agent, the cyst is observed, while in other cases surgical removal is necessary. All defects with thickened walls and without infection must be eliminated.
Bosniak II
A simple, benign neoplasm with slightly thickened walls, thin septa, and slight calcification. Such cysts also do not accumulate contrast. This includes homogeneous high-density formations with clear boundaries and infected cysts.
Hyperdense pathology with old coagulated blood or protein compacts the contents detected on a CT scan. These renal cysts do not become cancerous, so no therapy is required. It is important to be periodically examined using CT or ultrasound.
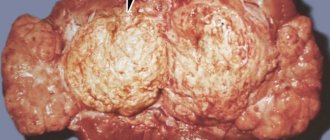
Bosniak IV
This is a malignant cyst with accumulation of contrast tissue component, numerous thick septa, thickened walls and large calcium deposits in the form of nodes.
In this case, the cavity of the neoplasm is completely filled with liquid. Cystic cancer is dangerous because it grows into neighboring organs and lymph nodes. To protect against metastasis, the patient should have it surgically removed immediately.
Cystic formations are divided into five categories, which differ in the degree of malignancy. Cysts of the first or second type do not cause the patient much discomfort. Often such kidney lesions are detected accidentally during a CT or ultrasound scan.
On this topic
The difference between prostate adenoma and prostatitis
Accurate histological examination allows the cyst to be classified into one category or another. If the neoplasm is classified according to Bosniak as I, II or IIF, then such a pathology is not dangerous for humans, but it is important to be periodically examined to monitor the condition of the disease.
The last two categories indicate a dangerous situation when cystic cancer has already developed or will soon appear, so you should not hesitate to promptly remove the identified problem.
Bosniak III
Renal cystosis with all manifestations of malignancy, with thickened walls, thick septa, accumulation of a contrast agent. Diagnosis reveals extensive nodular calcifications. These signs indicate the presence of cystic cancer, so urgent surgery is necessary to avoid metastasis.
If a CT scan reveals a benign hemorrhagic cyst, a formation with chronic infection, or multilocular nephroma, then constant monitoring is required. Moreover, even formations from this category of benign nature are often removed to avoid the development of oncological lesions.
Bosniak I
A simple single-chamber benign cyst with thin walls, without septations, calcium deposits and nodes. Such formations do not accumulate contrast or salts and have a liquid consistency. This is a common type of kidney cyst that does not cause any discomfort to the patient.
Moreover, such neoplasms do not degenerate into malignant ones, and therefore do not require treatment. However, it is necessary to regularly conduct diagnostic tests in order to constantly monitor the condition of the disease.