Causes of ureteral injury
External trauma
The prevalence of ureteral injuries is 3% of all external injuries of the genitourinary system! Most penetrating gunshot wounds are accompanied by multiple injuries to internal organs, most often the small and large intestines, liver and iliac vessels. Ureteral injuries due to blunt trauma are rare. The mechanism of injury is usually caused by sudden braking. These injuries are most often accompanied by damage to the liver, spleen and musculoskeletal system.
Iatrogenic trauma
The most common cause of ureteral injury is iatrogenic. Intraoperative ureteral injuries include dissection, avulsion, resection, compression, devascularization, electrocautery, and ureteral ligation.
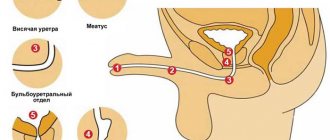
- Urethroscopy. Often these injuries are small (mucosal trauma or perforation) and, as a rule, insignificant. Serious injuries include avulsion and intussusception of the ureter. The incidence of ureteral injury may be reduced by using smaller diameter urethroscopes.
- The most serious injuries to the ureter occur during gynecological procedures, such as: hysterectomy (transabdominal, radical, transvaginal);
- C-section;
- oophorectomy.
- general surgical operations (low anterior and abdominoperineal resection);
Factors predisposing to iatrogenic ureteral injury
- Previous operations.
- The presence of infection and inflammation (diverticulitis, pelvic inflammatory disease, endometriosis).
- Radiation therapy.
- Malignant tumor.
- Uterine size greater than 12 weeks of gestation.
- Volumetric formations in the ovaries (more than 4 cm).
- Obesity.
- Massive bleeding.
- Congenital anomalies (duplicate and retrocaval ureter, horseshoe kidney)
Knowledge of the anatomical location of the ureters and the areas at highest risk of injury plays an important role in the prevention of iatrogenic injuries.
Intraoperative placement of stents to identify the ureter and prevent accidental injury has been extensively studied. Although placement of a ureteral stent before major pelvic-abdominal surgery may help palpate the location of the ureter and possibly avoid ureteral trauma, there has been no clear benefit to this strategy.
Therefore, routine placement of a ureteral stent before major pelvic-abdominal surgery is not recommended.
Possible complications
Inflammation of the ureter in women (the symptoms of the disease will intensify as the pathological processes progress) will lead to complications if medical care is not provided in a timely manner. Pathological processes will progress, the patient’s condition will worsen and, as a result, serious consequences will arise.
| Name | Description |
| Vaginitis | A disease that is accompanied by an inflammatory process on the surface of the vaginal mucosa. The woman complains of severe itching, burning, and body temperature also increases. |
| Emphysematous pyelonephritis | A purulent form of acute pyelonephritis, the causative agents of which are pathogenic microorganisms. Pathological processes provoke necrosis of renal tissue. In this case, characteristic bubbles filled with gas are formed. |
| Kidney failure | A pathological condition in which the functioning of the kidneys is impaired. As a result, the water-electrolyte balance fails. |
Inflammation of the ureter can lead to activation of existing chronic diseases. There is also a high probability of infection spreading to other organs and damage to the reproductive system in women. The chronic form of pathological changes can provoke irreversible consequences.
Inflammation of the ureter in women brings serious discomfort and disrupts the usual way of life. You cannot ignore the symptoms of the disease; it is important to go to the hospital immediately. Comprehensive diagnostics will determine the source of inflammation and its location. Treatment will eliminate pathological changes and reduce the likelihood of complications.
Symptoms and signs of ureteral injury
- There are no obvious early clinical signs of ureteral injury.
- Long-term clinical manifestations include prolonged intestinal obstruction, persistent flank pain, fever, urinary tract obstruction, urinary leakage, fistula formation, anuria, and eventually sepsis
- In general, more than 90% of ureteral injuries caused by external trauma are diagnosed immediately, and less than half of iatrogenic ureteral injuries.
- In any patient with penetrating or blunt abdominal trauma (especially in the lateral region) or undergoing abdominal or pelvic surgery with clinical signs of ureteral injury, radiologic imaging or intraoperative exploration of the ureter is indicated.
Stages and degrees
Taking into account the course of pathological processes, the following types of ureteritis are distinguished:
| Name | Description |
| Spicy | The inflammatory process develops quickly and unexpectedly. A common cause is the movement of stones and developing tumor processes. |
| Chronic | The inflammatory process in this situation is characterized by a sluggish course and minor clinical signs. The patient is often diagnosed with chronic pyelonephritis or cystitis. |
There is also a unilateral or bilateral inflammatory process, when the disease develops on one side or on both sides at once. A urologist and a comprehensive examination, which a specialist will prescribe for the patient, taking into account complaints and existing manifestations of the inflammatory process, will help to establish an accurate diagnosis.
Diagnosis of ureteral injury
- Imaging, revision surgery, or a combination of both.
Diagnosis is based on history and requires extreme vigilance, since symptoms are nonspecific and hematuria is absent in >30% of patients. Diagnosis is confirmed by imaging (eg, contrast-enhanced CT scan, intravenous urography, revision surgery, or both). Flank pain and fever are the main symptoms of blunt injuries.
Quick diagnosis is the first step to successful treatment. In case of damage to the ureter caused by external trauma, this can be difficult due to multiple lesions of other organs and the lack of early pathognomonic clinical and laboratory data. Iatrogenic injury caused by devascularization or coagulation of the ureter is usually diagnosed late, due to the slow development of symptoms. In general, diagnosis of any ureteral injury is difficult and requires a high index of suspicion.
Laboratory diagnostics
- Hematuria is absent in approximately 30% of cases of ureteral injury caused by external trauma.
- If there is a delay in diagnosis, azotemia may be the only manifestation of ureteral injury.
Radiation diagnostic methods
- If a ureteral injury is suspected, the most preferred method of radiological diagnosis is MSCT with intravenous enhancement. For adequate visualization during the excretory phase, delayed images must be obtained.
- Retrograde ureteropyelography allows you to obtain the most informative images of the ureter. However, this procedure is not always possible in unstable patients with polytrauma, as it requires additional time and equipment (for example, X-ray and cystoscopy). Retrograde ureteropyelography can be performed routinely. This study is also recommended when diagnosing any iatrogenic ureteral injury.
- Intravenous pyelography can be performed if other radiation diagnostic methods are not possible.
- Extravasation of contrast material on x-ray is a reliable sign of ureteral injury.
Intraoperative assessment
- During laparotomy or laparoscopy, the integrity of the ureter can be assessed visually and using methylene blue or indigo carmine administered (intravenously or through a vascular catheter).
- Urine leakage and dye extravasation are clear signs of ureteral injury.
- Changes in the color of the ureter or decreased motility may be signs of ureteral injury.
- The presence of a release of contrast material from the orifices of the ureters, detected during cystoscopy, excludes ureteral avulsion, but not its partial rupture or contusion.
- Installation of a ureteral catheter can be performed by cystoscopy or through a cystostomy. When the ureter is injured, difficulties usually arise when installing a ureteral catheter. It is important to evaluate the condition of both ureters.
Diagnosis of integrity violations
It is not so easy to determine whether the internal hollow tube is damaged, mainly due to unexpressed symptoms. The first step is a consultation with the attending physician with a detailed description of the patient’s complaints. Then you need to take a urine test. If laboratory test results show an increase in the number of red blood cells, the likelihood of rupture of the paired organ is high. The next stage is ultrasound of the peritoneum and retroperitoneal region. Enlarged renal calyces and pelvis indicate damage to the connecting tube.
The most accurate method for identifying damage is radiographic examination. With the help of retrograde ureteropyelography, which involves injecting the patient with a special contrast solution through a catheter during cytoscopy, the diagnosis is determined accurately when the injected solution is visualized outside the organ. Highly accurate results are also obtained from different types of computed tomography. If a violation is detected, the extent of damage is assessed using excretory urography.
Treatment of ureteral injury
- For minor injuries, a nephrostomy or ureteral stent is used.
- Severe injuries require surgical repair.
All injuries require surgical intervention. For minor injuries (eg, contusions or partial rupture), percutaneous nephrostomy or cystoscopic placement of a ureteral stent is often sufficient. Complete transection or avulsions require interventions using reconstructive techniques, including ureteral reimplantation, primary ureteral anastomosis, anterior bladder flap, iliac interposition and, as a last resort, autotransplantation.
External trauma
- Most patients with ureteral injury due to external trauma require urgent exploratory surgery due to the presence of abdominal injuries, the treatment of which is a priority.
- If the patient’s condition is stable and a ureteral injury is detected intraoperatively, the latter should be immediately eliminated.
- If there is a significant delay in diagnosing a ureteral injury or if the patient's condition is unstable, the first stage of treatment is most justified by urinary diversion (by percutaneous nephrostomy or placement of a ureteral stent) or ureterocutaneostomy. Reconstructive surgery is performed as planned.
- When performing surgery on severely traumatized patients, the lethal triad of acidosis, hypothermia, and coagulopathy requires damage control strategies. It involves stopping the operation and transferring the patient to the intensive care unit for appropriate intensive care, after which (24-36 hours later) definitive surgical treatment of the injuries (including ureteral reconstruction) is performed.
Iatrogenic trauma
- There is a delay in diagnosis of most non-urological iatrogenic ureteral injuries.
- The first stage of treatment usually involves urinary diversion only.
- After retrograde ureteropyelography, placement of a ureteral stent may be attempted. If a ureteral stent cannot be installed, a percutaneous nephrostomy must be performed to divert urine.
- Many of these injuries can only be resolved by urinary diversion.
Ureteral reconstruction
The best access for revision of the ureter is a midline laparotomy. In case of delayed reconstructive surgery on the ureter, the approach may be changed depending on the specific situation. For example, a subcostal incision can be used for surgery on the upper or middle third of the ureter, and the Gibson (intermuscular) approach can be used for the lower third. Most reconstructive surgeries on the ureter are performed openly. Given the advances in laparoscopic and robot-assisted surgery, the surgeon's experience is a major factor in the use of these minimally invasive techniques. In the presence of concomitant injuries to the abdominal organs, part of the greater omentum can be used to delimit and protect the ureter in the reconstruction area.
Basic principles of ureteral reconstruction.
- Careful treatment of the wound.
- Creation of a tight, tension-free anastomosis (using absorbable sutures).
- Isolation from surrounding organs.
- Adequate drainage of the ureter and retroperitoneum.
The choice of reconstruction method depends on the level and extent of damage.
Stitching/ligation and incomplete division of the ureter
In some cases, with minor injuries to the ureter - ligation or incomplete intersection of the ureter, identified intraoperatively, it may be sufficient to remove the ligature or suturing the defect in the ureteral wall. It is necessary to perform an inspection of the ureter, the purpose of which is to identify signs of devascularization, after which it is necessary to install a ureteral stent.
Injuries of the lower third of the ureter
Ureterocystoneostomy
The most optimal method for treating injuries of the lower third of the ureter is submucosal reimplantation of the ureter into the bladder, which is usually performed using a combination of intra- and extravesical approaches. In this case, the ureter is passed through the posterior wall of the bladder medial to the mouth of this ureter. If possible, a submucosal tunnel is created based on the standard 3:1 ratio (submucosal tunnel length to ureteral diameter).
Creation of a tension-free anastomosis is an alternative to submucosal ureteral reimplantation, since vesicoureteral reflux in adult patients is usually minor.
Psoas-hitch technique
The best treatment for injuries to the lower third of the ureter is Psoas-hitch surgery with ureteral reimplantation. The bottom of the bladder is separated from the peritoneum, after which ligation of the contralateral upper vascular pedicle of the bladder is performed. If necessary (for adequate mobilization of the bladder), bilateral ligation of the upper vascular pedicles of the bladder is possible.
Next, an oblique incision is made in the bladder wall perpendicular to the affected ureter. The dome of the bladder is pulled towards the iliac vessels and fixed to the tendon of the psoas muscle with interrupted sutures, avoiding damage to the genital femoral nerve. Reimplantation of the ureter is performed according to the technique described above. The bladder wall is sutured with a double-row suture perpendicular to the incision, after which I install! suprapubic cystostomy drainage.
Injuries of the middle and upper third of the ureter
Ureteroureterostomy
The most optimal treatment method for grade II-IV ureteral injuries in the middle and upper third is ureteroureterostomy. The proximal and distal ends of the ureter are carefully isolated and dead tissue removed. Then they are spatulated (longitudinal dissection). Next, the ureteral wall defect is tightly sutured without tension with absorbable suture material (4-0) against the background of an installed ureteral stent.
Transureteroureterostomy
If half of the distal ureter is affected and there is insufficient mobility of the bladder or severe scarring in the pelvic area, transureteroureterostomy can be performed. After opening the posterior wall of the peritoneum, both ureters are isolated. Next, the damaged ureter is passed through the retroperitoneal window to the contralateral side, avoiding kinks. A 1.5 cm longitudinal incision is used to open the lumen of the intact ureter. Then an end-to-side anastomosis is performed using interrupted sutures made of absorbable suture material. To prevent conflict, the transplanted ureter should be positioned over the inferior mesenteric artery. Because this operation traumatizes the healthy ureter, it should only be performed in carefully selected patients.
Ureterocalicostomy
Ureterocalicostomy can be performed in cases of extensive injury to the ureteropelvic segment and proximal ureter. The first step is amputation of the lower pole of the ipsilateral kidney to the lower group of calyces, after which a wide spatulation of the ureter is performed, sufficient to perform an end-to-end ureterocalicoanastomosis. This operation is associated with extensive mobilization of the kidney and a high incidence of stricture formation in the anastomosis area.
Total ureteral injury
In case of total damage to the ureter, it can be replaced with a segment of the ileum. However, this operation cannot be performed immediately, since it is necessary to carry out mechanical bowel preparation. In addition, it cannot be performed in patients with severe renal impairment (serum creatinine >2 mg/dL) due to possible metabolic complications (eg, hyperchloremic acidosis due to urine absorption). Additional contraindications to intestinal ureteroplasty are radiation enteritis, inflammatory bowel disease and bladder dysfunction.
The surgical steps include medial mobilization of the ipsilateral colon, isolation of the ureter, and resection of 20–25 cm of the ileum 15 cm proximal to the ileocecal junction. After restoration of intestinal patency, the resected segment of intestine is placed in the direction of peristalsis (isoperistaltically) behind the intestine. Next, a proximal pyeloileal anastomosis is applied “end to end”, and a distal ileovesical anastomosis is “end to side” (without tunneling).
In patients with a solitary kidney or a significant decrease in renal function with complete ureteral avulsion, autotransplantation can be performed. In this case, the kidney on the affected side is transplanted into the area of the iliac fossa, applying vascular anastomoses between the renal and iliac vessels, as well as an ileovesical anastomosis for adequate urine drainage.
Drainage
- All ureteral injuries require the installation of a ureteral stent for adequate urine drainage; an internal ureteral stent is used for this purpose. Depending on the volume of reconstructive surgery, kidney drainage with a ureteral stent is continued for 2-6 weeks.
- In order to prevent the formation of retroperitoneal urinoma, drainage is installed in the reconstruction area of the ureter. The duration of drainage of the retroperitoneal space is at least 48 hours or until urine flow through the drainage stops.
- Bladder decompression is achieved by installing a urethral catheter and/or cystostomy drainage. In most cases, the urethral catheter is removed after a week, although sometimes, in order to prevent vesicoureteral reflux, it is possible to increase the duration of drainage.
Symptoms of the disease
Symptoms of a violation of the integrity of an organ never appear clearly. As a rule, this is only pain in the pelvis, back, under the ribs. The presence of blood in the urine will be indicative. In the vast majority of cases (about 80%), a sick person is initially unaware of the illness that has befallen him. After the disease develops, with the appearance of complications, the picture becomes clearer.
Treatment of the pathology requires serious treatment. Closed penetrating injuries of the ureter are detected when:
- increased body temperature;
- pain and swelling in the lumbar region;
- nausea and vomiting.
Postoperative disturbances in the functioning of the tubular organ are detected by urine excreted through installed drainages. If the catheter was not inserted into the patient, and the ureter has wounds, signs of urinary leakage develop, including manifestations of intoxication, delirium, hyperemia of the skin, and an increased content of metabolic products is found in the blood. Wounds inflicted by cold steel and firearms, which affect the functioning of the urinary system, cause shock in the victim and provoke urination through the wound.
Manifestation of the clinical picture
The occurrence of ureteral stricture does not have symptoms that are characteristic of this disease.
Obvious signs of obstruction of the urinary canal are determined only with the development of complications caused by impaired urine excretion.
Depending on the etiology of the disease, symptoms may indicate the development of chronic renal failure, urolithiasis or inflammatory processes.
As a rule, the following signs occur:
- dull aching pain in the lumbar region;
- renal colic (acute pain radiating to the side);
- decreased amount of urine with adequate fluid intake;
- signs of intoxication of the body (nausea, vomiting, convulsions);
- increased blood pressure;
- cloudy urine or unpleasant odor;
- increase in body temperature.
An important factor influencing the appearance of symptoms is one or two-sided damage to the renal apparatus.
As a rule, with unilateral damage, a redistribution of the load occurs on the healthy kidney with a gradual loss of functional activity of the affected one.
In the latter case, symptoms may be absent for a long time.
An acute course with severe pain is observed when the ureter is ligated during surgery or with urolithiasis.
- Ureteral cancer: symptoms, treatment of ureteral cancer, metastases in the ureter
Inflammation of the ureter in men
Inflammatory processes associated with the activity of the genitourinary system can bring not only discomfort to a person’s life, but also cause many diseases.
The main organ of the urinary system is the kidneys, which filter a huge amount of blood during the day, resulting in urine. Further along the ureters it enters the bladder, and from it, as it fills, it is discharged out through the urethra, called the urethra.
The ureters are the link between the kidneys and the bladder, and their inflammation can be of several types. Among them, it is worth noting septic, associated with ascending infection by various types of microorganisms. The causes of this inflammation can be:
- Cystitis is inflammation of the bladder.
- Urethritis is inflammation of the urethra.
As well as aseptic inflammation of the ureters, which is a descending path of the disease. In this case, the pathology may develop due to kidney problems, these are:
- Urolithiasis disease.
- Pyelonephritis.
Since urine is a good source for the development of pathological microelements, when it is poor or stagnant, septic complications can often develop against this background.
- 1 Reasons
- 2 Symptoms
- 3 Diagnostics
- 4 Treatment
- 5 Editor
Causes
As a rule, inflammation of the ureter in men is associated with complications after diseases of the genitourinary system. First, the kidneys or bladder become inflamed, and as a result, the ureters suffer. Both female and male populations are susceptible to this disease. The main factors causing pathology in the ureters are the following:
- Kidney disease, that is, pyelonephritis.
- Inflammation of the bladder, cystitis.
- Often the cause of this disease in men is prostatitis and urethritis.
- Oncological diseases of the genitourinary system can also cause pathology.
However, in the first place among all sources of the inflammatory process is urolithiasis of the kidneys. Since the stones formed in them with their sharp sides damage the delicate walls of the ureters.
Stone in the ureter. Source: ProMoiPochki.ru
Sometimes large stones can lead to complete blockage of the lumen, which prevents the outflow of urine, and as a result, an inflammatory process occurs.
Symptoms
When pain in the ureter appears in men, the symptoms can be expressed in varying degrees of intensity. If the pathology is associated with complications of urolithiasis, then they may look like this:
- The primary symptom is the occurrence of colic, which can be accompanied by quite severe pain in the lumbar region.
- Accompanied by fever and pain in the side of the abdomen.
- Frequent urge to go to the toilet, with small and painful urine output.
If the pathological process is associated with inflammation of the bladder, then the pain syndrome can be quite severe. It may be accompanied by surges in blood pressure, headaches, nausea, and sometimes vomiting.
Inflammation of the ureter associated with pyelonephritis is most often accompanied by general weakness, dull pain in the lumbar region, most often on both sides, in some cases there are signs of intoxication.
The first signs of inflammation of the ureters in men, for which you need to immediately seek medical help, are delayed urine output, problems with urination, acute pain in the groin area and genitals.
Diagnostics
To make a correct diagnosis, the patient is prescribed a series of biochemical and instrumental studies. These include:
- General analysis of urine and blood to determine the levels of proteins, leukocytes and seromucoids. This allows us to determine the stage of the inflammatory disease process.
- Blood from a vein to confirm or absence of infection in the genitourinary system.
- Cystoscopy and catheterization of the urinary canal are performed.
- Mandatory examination is urography, urethroscopy and ultrasound of the pelvic organs.
Treatment
Once diagnosed and prescribed adequate treatment, it helps to get rid of the inflammatory process in the ureter in a relatively short time. Conservative therapy consists of taking antibacterial drugs, physiotherapy, washing the ureter using a catheter and antimicrobial drugs.
The patient is credited with drinking plenty of fluids, which can help quickly remove pathogenic microbes from the body. Since inflammation is accompanied by a painful syndrome, the use of antispasmodics and painkillers is mandatory.
A good addition to treatment is the use of folk remedies that, together with medications, accelerate the patient’s recovery.
In the most severe and life-threatening situations, such as sudden urinary retention, surgical intervention is required.
To prevent inflammation of the ureters, patients are advised to have proper nutrition, excluding from the diet: sour, salty and spicy foods, drinks that cause irritation in the urinary system, to lead a healthy lifestyle, to use protected sexual intercourse, and to protect themselves from hypothermia.
Source: https://uran.help/diseases/vospalenie-mochetochnika-u-muzhchin.html
Basic information about pathology
Unlike the process of vascular sclerosis, where the pathological process can last for many years without any signs of impairment, narrowing of the lumen of the ureter (ureter), in a relatively short period of time, leads to the development of an acute condition caused by acute or chronic renal failure.
Since the ureter is a tube consisting of smooth muscle fibers covered on the outside with connective tissue and on the inside with mucous membrane, it has a certain reserve of mobility and elasticity.
The location and structure of the ureter is determined by the need to remove liquid human waste products (urine) from the kidneys to the bladder.
The length of the ureters depends on the location of the kidneys and the height of the person and on average ranges from 20-35 cm.
The width of a healthy ureter is about 5-8 mm and has several natural (physiological) narrowings. The most pronounced narrowings are the ureterotpelvic one, which forms during the transition of the ureter from the peritoneum to the small pelvis, and the pyeloureteral one, which forms a connection with the renal pelvis.
Like any other organ, the ureter has its own blood supply, provided by the renal, iliac artery and aorta.
Total information
The ureter is “hidden” deep enough, so injuries to it occur less frequently than damage to other parts of the urinary system. But in comparison with injuries to other urinary structures, this is a more problematic pathology, since it leads to disruption of the outflow of urine and secondary pathology of the kidneys, the pelvis of which is literally overflowing with urine. Also problematic is the fairly common confusion in diagnosis and differential diagnosis (in particular, in women with pathologies of the reproductive system).
Males and females suffer with approximately the same frequency, but the causes of their pathology may be different. In women, ureteral injury is often associated with various obstetric and gynecological procedures, but the described injury in men more often occurs when exposed to external traumatic factors.
note
In every tenth patient with a ureteral injury, it occurred during an endoscopic examination.
Forecast
The prognosis for ureteral injury depends on the degree of damage, timely detection, timeliness and adequacy of medical care. If the injury is detected on time, this helps to avoid complications.
The prognosis worsens in cases such as:
- transporting the victim to the clinic late;
- late development of symptoms (with reduced patient reactivity), which entails late diagnosis and treatment;
- incorrect treatment tactics - in particular, wait-and-see;
- traumatic shock and other complications of ureteral injury.
A critical condition may develop due to complications of the described disorder.
Kovtonyuk Oksana Vladimirovna, medical observer, surgeon, consultant doctor
1, total, today
( 50 votes, average: 4.54 out of 5)
Urolithiasis in children: symptoms and treatment
Spongy kidney: causes, signs, treatment