JUXTAGLOMERULAR APPARATUS
The juxtaglomerular apparatus is a general term for specifically differentiated groups of cells at the vascular pole of the renal corpuscle. The apparatus contains the following components: macula densa, juxtaglomerular cells and juxtaglomerular mesangium.
The macula densa (macula densa), distal convoluted tubule, is a clearly demarcated zone of 15-40 specialized epithelial cells lying on a dense basement membrane (BM). The cells are cubic or prismatic in shape, have several lateral processes and a variable number of short microvilli at the apical pole. The nuclei of the macula densa cells lie much closer together (“tightly”) than in the neighboring unspecialized cells of the distal tubules, the star-shaped outline of which is visible around the macula densa cells. The nuclei are relatively voluminous and contain prominent nucleoli. The cytoplasm includes short mitochondria, mainly scattered at the apical pole of the cell; the Golgi complex is small and most often localized in the upper third of the cell body, and the cisterns of the granular endoplasmic reticulum are short and flattened. In the basal part of the cell there is a moderately developed basal labyrinth. Through the loose basement membrane, some macula densa cells come into contact with juxta- and extraglomerular mesangial cells.
The function of the macula densa is unclear; it is assumed that it functions as an osmoreceptor, and all changes in sodium concentration in the distal tubules are transmitted to the juxtaglomerular cells, which respond by increasing or decreasing renin production.
Juxtaglomerular cells (JC) form a group of specially differentiated smooth muscle cells located among normal smooth muscle cells (MSCs) in the tunica media of the afferent arteriole (TA) at its entry into the glomerulus. Like macula densa cells, juxtaglomerular cells are in contact with the endothelium (E) of the arteriole. These are large spindle-shaped cells with an eccentric nucleus, a large number of small mitochondria, a well-developed Golgi complex, short cisternae of granular endoplasmic reticulum, a small number of glycogen particles and actin myofilaments adjacent to the cell membrane. A significant number of renin or juxtaglomerular granules (JGs) arise from the Golgi complex and fill the cytoplasm. Juxtaglomerular cells have been shown to produce and secrete renin or its precursor.
Renin is a proteolytic enzyme that converts angiotensinogen to angiotensin I. The latter is converted in the lungs to angiotensin II, which is a powerful stimulator of the formation and release of aldosterone and the most powerful known vasoconstrictor.
The extraglomerular mesangium (EM) is a group of cone-shaped cells, also called Gurmagtig cells, that lie just below the macula densa. The extraglomerular mesangium is laterally bounded by the afferent (AfA) and efferent arterioles (the latter not shown) and continues into the intraglomerular mesangium (M).
The extraglomerular mesangium is formed by flattened stellate cells with an ellipsoid nucleus in the center containing condensed chromatin. The cytoplasm contains a few organelles, a few small lysosomes and rare secretory granules. Narrow cellular processes form an irregular network that is devoid of blood and lymphatic vessels, but contains rare adrenergic nerve endings (NA). Each cell is surrounded by a distinct basal lamina (partially removed for better understanding). Some extraglomerular cells contact juxtaglomerular cells.
The function of extraglomerular cells is unknown. It is currently assumed that the juxtaglomerular apparatus is a neuroendocrine formation that exercises local control of glomerular hemodynamics.
Note the circumpolar epithelial cell (PEC) with clear granules and the glomerular capillaries (Cap) surrounded by podocytes (P). The function of the circumpolar cells is unknown.
Outside the distal convoluted tubule, stellate fibrocytes (S) and a fenestrated capillary (FC) of renal interstitial tissue can be seen.
Albuminuria - what is it?
Protein detected in urine indicates a pathological process that occurs in the human body and is associated with impaired kidney function. This disease is called albuminuria (proteinuria).
What is albuminuria?
Albumin is a type of protein that is found in the blood in a significant amount (almost 60% of the total amount of proteins). The disease is named after this protein. In a healthy person, the amount of albumin in the urine does not exceed 50 mg. A general urine test cannot provide such information, so sulfosalicylic acid or boiling in an acidic acetic environment is used to detect elevated protein. If the study reveals traces of protein reaching a level of 150-200 mg, the patient is diagnosed with albuminuria.
In some cases, there is a short-term increase in albumin levels. For example, after heavy physical activity, competition, marching, active play, strong emotional experience, hypothermia, or before the onset of the menstrual cycle. In this case, they speak of the occurrence of physiological albuminuria.
Attention! With physiological albuminuria, protein loss can be up to 1 mg/g. This type of disease does not require treatment, as it does not pose a threat to the functioning of the kidneys.
Constantly present albumin in a significant amount indicates kidney disease or a complication of another concomitant disease. The risk category includes:
- diabetics;
- hypertensive patients;
- HIV-infected;
- people with lupus, anemia, rheumatoid arthritis.
Causes of pathological albuminuria
Pathological proteinuria occurs due to two types of disorders:
- Protein molecules (small and large sizes) leak into primary urine through a passage widened due to the disease, as the basement membrane becomes more permeable.
- The basement membrane has no deviations, but proteins, as a result of disruption of the reabsorption process, collect in the tubular apparatus. Albumin accumulates without having time to be absorbed and returned to the blood.
Types of pathological albuminuria
The pathological form of the disease is distinguished not only by an increased amount of albumin in the urine, but also by a high content of leukocytes, erythrocytes, and the presence of bacteria, salts, and casts. This form has two types:
- extrarenal proteinuria (false);
- renal proteinuria (true).
With false albuminuria, an increase in protein is caused by:
- inflammatory diseases associated with dysfunction of the digestive system;
- the process of cell destruction with low hemoglobin;
- burns over most of the body;
- frostbite;
- prolonged exposure to low temperatures.
True albuminuria is always associated with inflammatory diseases in the kidneys. Inflammation causes deformation of the basement membrane and an increase in the permeability of protein molecules. These diseases include:
- glomerulonephritis;
- amyloidosis;
- nephrosclerosis;
- nephropathy during pregnancy;
- circulatory disorders in the kidneys.
Types of pathology
The classification of albuminuria is based on several factors that provoke it:
- Increased body temperature during viral infections not accompanied by inflammatory processes in the organs of the urinary system.
- Emotional stress, stress.
- Flick.
- Staying in a monotonous position for a long time.
- Dehydration in hot weather.
- Allergy.
- Obesity.
In children, the disease can develop against the background of:
- Severe diarrhea, vomiting, drinking disorders. This is dehydration albuminuria.
- Increased irritability of the kidneys that occurs after swimming in cool water, overfeeding, palpating the kidneys, physical fatigue, and a feeling of fear. This is stroke albuminuria.
How to diagnose albuminuria?
Diagnosis of albuminuria is complicated by the absence of symptoms in TAM. The disease is usually suspected if the following signs are present:
- swelling of the legs, area around the eyes, reproductive organs;
- foamy, red urine;
- feverish condition;
- heavy sweating at night;
- loss of appetite;
- weight loss.
The doctor prescribes an extended test, during which a special paper strip is used to detect the amount of albumin in the urine.
In order to simplify the process of diagnosing the disease, 9 years ago, during the London International Conference, the stages of proteinuria were determined. They depend on the amount of protein per 1 g of creatinine in urine:
- Stage I - less than 30 mg/g.
- Stage II – 30 – 299 mg/g.
- Stage III - above 300 mg/g.
Attention! In a healthy person, the excretion level in the tubular epithelium is less than 10 mg/g. If the readings reach 29 mg/g, an average level of excretion is diagnosed. For high levels, urinary protein losses range from 30 to 299 mg/g. In particularly severe cases, losses of 300-1999 mg/g and more than 2000 mg/g are observed.
Laboratory tests for detecting protein in urine
Laboratory studies are based on three methods:
- quality;
- semi-quantitative;
- quantitative.
The qualitative method allows you to detect the presence of proteins, but does not make it possible to count them quantitatively. If proteins are present in the tests, the patient is sent for a secondary examination with a detailed quantitative analysis.
The quantitative method is based on numerous techniques (there are more than 100 of them). Any quantitative method is based on a chemical effect on protein in urine or a heating process. For analysis, a single morning portion of urine or a daily volume is taken.
Patients with chronic renal failure
Excretion of protein in the urine causes dysfunction of the kidneys and ultimately leads to chronic renal failure. Therefore, in such patients, constant examinations of albumin in the blood and urine are carried out.
Based on the data obtained, you can:
- verify the presence or absence of albuminuria;
- predict the development of the disease;
- establish possible risks of complications in the functioning of the cardiovascular system;
- decide on the method of therapy.
Treatment
There is no specific treatment for proteinuria. Therapy is carried out on the basis of pathogenetic mechanisms of organ failure. The positive result of treatment can be judged by the disappearance of protein in the urine. The patient is prescribed:
- A diet excluding protein, salty, fatty foods.
- Maintaining bed rest.
- Hospitalization during an exacerbation.
- A course of antibiotics.
- Hemodez.
- Alkaline solution.
- Hemodialysis.
Albuminuria is a disease associated with the appearance of albumin in the urine. The reasons for its occurrence are different: physiological, pathological. The physiological form of the disease goes away on its own after eliminating the factors that provoked it. The pathological form requires a thorough quantitative examination.
What else does an ultrasound image record?
A perinephric dark highlight of a regular contour is a possible consequence of a hematoma, in which an area of hypoechoic parenchyma is indicated. When bleeding occurs, its area increases. When blood clots, the shape does not reflect the sound wave.
Dark contours revealed by ultrasound may be the result of a long inflammatory process, accompanied by the accumulation of purulent fluid, which over time leads to such undesirable consequences as:
- Rupture of the cyst with major bleeding.
- Compression of the renal parenchyma, which contributes to disruption of stable functioning.
- Development of nephropathy.
The location of the spots in the image may indicate a disease in other organs. So, according to doctors, a spot above the urinary and excretory system diagnoses a benign tumor on the spleen or liver.
An anechoic cavity on ultrasound as a dark spot
Only a specialist can determine the exact anechoic pathology based on the results of a comprehensive examination. To do this, the doctor may additionally prescribe: a general and biochemical analysis of blood, urine, fluoroscopy, computed tomography or magnetic resonance imaging. In exceptional cases - cytological examination.
A comprehensive examination is a guarantee of proper treatment.
In Efremova's dictionary
Emphasis: apparatus
- m. Device, device, technical device.
- trans. Notes, indexes and other additional materials for scientific work, collected works, etc.
- A system of organs of a person, animal or plant that performs. a certain function.
NEPHRON TUBULES IN THE MEDULA ELECTRON MICROPHOTOS
b) Collecting duct and thin tubules
(according to D. Pann and R. Noltke)
1 - thin tubule;
2A - microvilli on the apical surface of epithelial cells.
Compared to the proximal tubule, microvilli are located much less frequently and therefore do not form a brush border.
a) Thin tubules (according to A.B. Rodin)
1A - nuclear-containing area of the epithelial cell protruding into the lumen,
https://www.youtube.com/watch?v=ytadvertiseru
1B - underlying basement membrane.
2A - nuclear-containing area of the endothelial cell protruding into the lumen;
2B - basement membrane.
In the anucleate region, the capillary wall is noticeably thinner than the wall of the thin tubule.
3 - connective tissue cell in the space between thin tubules and capillaries.
What to pay attention to
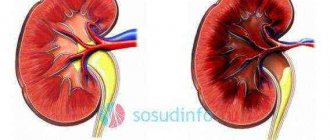
This diagnosis can be made when there is a kidney abnormality caused by intracystic hemorrhage, tumor or cyst.
These formations in the kidneys are a fairly common pathology, characterized by:
- dull pain in the lumbar or hypochondrium areas, aggravated by physical activity;
- the appearance of blood streaks in the urine (hematuria);
- increased blood pressure;
- nausea;
- general malaise.
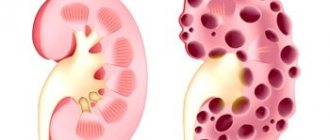
This is what multiple kidney cysts look like on an ultrasound
The cyst can be single, multiple, primary or secondary, congenital or acquired.
The cause of the appearance of the latter type is infection of the kidneys or urinary system.
The ultrasound result for this disease appears in the form of round, thin-walled spots of various sizes with clear outlines. In the early stages of the disease they are small. In the later stages, it can exceed 3 cm, which is dangerous to health.
Clinical significance
Excess secretion of renin by juxtaglomerular cells can lead to excess activity of the renin-angiotensin system, hypertension, and increased blood volume. It does not respond to conventional treatment for hypertension, namely medications and lifestyle changes.
One reason for this may be increased renin production due to narrowing of the renal artery or tumor of the juxtaglomerular cells, which produces renin. This will lead to secondary hyperaldosteronism, which will lead to hypertension, high blood sodium, low blood potassium, and metabolic alkalosis.
Morphology of YUGA
The juxtaglomerular apparatus consists of three types of cells located in close proximity to the nephron and forming a functional system with positive feedback with it. The first type of cells is epithelioid (or granular), which are modified smooth myocytes of the muscular wall of the arteriole. They are located in large numbers in the muscle layer of the afferent arteriole and in smaller numbers in the efferent arteriole. This indicates their involvement in determining the difference in hydrostatic pressure in these vessels.
The granule cells contain baroreceptors that transmit information to the juxtavascular cells of the JGA. Granule cells are also the main producers of renin, an enzyme that regulates blood pressure in the circulatory system. This enzyme is also partially capable of synthesizing juxtavascular cells (second type) of the juxtaglomerular apparatus. The functions of these cells are that they are a link between epithelial cells and the dense spot of the urinary tubule. Juxtavascular cells are located in the space between the afferent and efferent arterioles of the JGA.
In the dictionary Synonyms 4
automatic, unit, antenna, apparatus, bathyplane, bathyscaphe, bathysphere, runner, block apparatus, bodo, vacuum apparatus, cradle, rectifier, germinator, hydraulic apparatus, hydraulic monitor, hydraulic elevator, glazer, state apparatus, graphapparatus, defecator, jigger, iron separator, eraser, kaliapparat, klopfer, colosha, copier, kotrelle, cracker, copier, machine, mimeograph, moviola, monju, undulator, tester, party apparatus, pneumatic apparatus, polyapparatus, semi-automatic, pulmotor, pulp thickener, dust concentrator, radio apparatus, X-ray apparatus, rotator, sovapparat, telegamma apparatus, telegram apparatus, teletype, heat exchanger, shotcrete apparatus, tribapparat, turbodrill, installation, folding apparatus, filmophone, photostat, utility apparatus, shaft phone, yuz
In the Encyclopedia Dictionary
(from lat. apparatus - equipment),..1) device, technical device, device...2) A set of institutions, organizations serving any area of management, economy, etc...3) A set of employees of an institution, organization ; the totality of employees ensuring the functioning of any elected body...4) Notes, indexes and other auxiliary materials for scientific work, printed publications, etc. (critical apparatus, scientific reference apparatus)...5) The totality of human, animal or plants that perform any special function of the body (digestive apparatus, respiratory apparatus).
Sources
- https://siberian-health.ru/yukstaglomerulyarnyy-apparat-pochek
- https://glosum.ru/%D0%97%D0%BD%D0%B0%D1%87%D0%B5%D0%BD%D0%B8%D0%B5-%D1%81%D0%BB% D0%BE%D0%B2%D0%B0-%D0%90%D0%BF%D0%BF%D0%B0%D1%80%D0%B0%D1%82
- https://fb.ru/article/360733/yukstaglomerulyarnyiy-apparat-pochek-stroenie-i-funktsii
[collapse]