STD
The abbreviation ICD (ICD) is an abbreviation for the International Classification of Diseases. Its main purpose is to provide statistics on diseases, health-related problems and causes of mortality throughout the world. The number 1 0 indicates the serial number of revisions (amendments and additions), which periodically, usually once every 10 years, occur at the initiative of WHO. Encoding diseases with codes, including Urethritis according to ICD 10, converts verbal diagnoses into combinations of letters and numbers, which simplifies the collection and storage of data, their analysis and comparison.
The headquarters of the WHO, where ICD codes are transmitted from all countries of the world, is located in Geneva
The information that is collected by the statistical departments of clinics and hospitals and then transmitted vertically to WHO is not personalized. It does not contain the person’s passport data and place of residence. For a patient diagnosed with Gonorrheal Urethritis, the ICD code will not be entered on the sick leave. But the instructions oblige you to put the number 2 on line 11 – Cause of the disease, since this disease is sexually transmitted and is included in the list of diseases dangerous to others.
- Basic ternary ICD codes
- Encodings specifying infectious agents
Short description
Urethritis is inflammation of the urethra. The most common pathogen is Chlamydia trachomatis. Frequency . Worldwide, 250 million cases are recorded annually.
Code according to the international classification of diseases ICD-10:
- N34 Urethritis and urethral syndrome
Classification • Infectious •• Nonspecific (bacterial, viral, caused by mycoplasmas, caused by chlamydia, mycotic) •• Specific (gonorrheal, trichomonas) • Noninfectious •• Traumatic - urethritis is caused by the introduction of foreign bodies into the urethra, most often masturbation •• Allergic •• Caused by the presence of diseases of the urethra - strictures, cancer, etc. •• Metabolic - phosphaturia, oxaluria, uraturia •• Congestive - caused by venous stagnation of blood in the mucous membrane of the urethra. Occurs with frequent sexual intercourse, masturbation, chronic constipation, hemorrhoids, etc. • Along the course •• Acute •• Torpid •• Chronic • By localization •• Anterior •• Total.
Traditional methods of treatment
Traditional medicine is an auxiliary aid in the treatment of the disease. It has a diuretic and anti-inflammatory effect. Plants are used not only for decoctions, but also in the regular diet. The herbal treatment method should not exceed 1 month. To treat urethritis, the following herbal mixtures are used:
- sage, St. John's wort, horsetail, caraway fruits, wheatgrass;
- knotweed, shepherd's purse, ivy-shaped budra, watch, tansy flowers;
- motherwort, black poplar buds, madder rhizomes, heather grass, fennel fruits;
- celandine, black tea shoots, hop fruits, coriander, steelberry roots.
There are several recipes:
- Pour 80 grams of chopped parsley with milk. Place the contents in the oven and heat the milk, then strain. Take 100 grams every hour throughout the day.
- Pour 200 g of boiling water into 25 grams of dried cornflower flower. Wait for it to brew and take 100 grams.
- Grind 150 grams of currant leaves and pour 400 grams of boiling water. Leave for 2 hours. Take 100 g. It helps pregnant women and children well.
- Brew one teaspoon of yellow green chickweed in one glass of boiling water. Wait until it brews and drink. Take one glass of infusion in the morning, afternoon and evening.
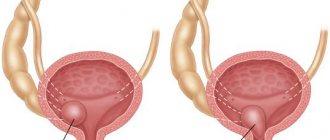
Symptoms (signs)
Clinical picture • Acute urethritis - severe subjective disorders: burning and pain when urinating, copious discharge from the urethra, urethral sponges are bright red, swollen • Torpid urethritis - subjective disorders are mild, may be absent: paresthesia, itching in the urethra, scanty discharge • Chronic urethritis - with a duration of torpid urethritis for more than 2 months. The clinical picture is similar to that of torpid urethritis • Anterior urethritis - inflammation of the anterior part of the urethra (up to the membranous part) • Total urethritis - inflammation of the entire urethra. Dysuric disorders characteristic of prostatitis are added.
Encodings specifying infectious agents
Coding of bacteria and viruses that can cause inflammation of the urethral walls
If gonococci are to blame for the inflammatory process, then the code A54 is added to the main encoding, the combination A56 is allocated for chlamydia, and A59 is allocated for trichomonas.
In conclusion, we offer a video in which the doctor will talk about the causes, symptoms and effective methods of drug treatment for the disease Urethritis, ICD10 code N34. It definitely needs to be treated. The cost of chronic infection is diseases of the genitourinary organs, which can lead to both male and female infertility.
Diagnostics
Research methods • Microscopy of discharge from the urethra. If there is no discharge - scraping. The presence of more than 5 leukocytes in the field of view indicates the presence of urethritis • Sowing the discharge or scraping on nutrient media to determine the pathogen and its sensitivity to antibacterial therapy • If chlamydial urethritis is suspected, serodiagnosis is carried out • Urethroscopy (contraindicated in acute urethritis): soft and hard infiltrates, morganitis, littreitis • Two-glass test •• With anterior urethritis, the first portion is cloudy, the second is transparent •• With total - the urine is cloudy in both portions • Urethrography is necessary for cicatricial strictures of the urethra.
How to eat properly with urethritis?
It is necessary to exclude sour, spicy, salty foods from meals, and add alkaline ones.
- Eat fresh fruits, vegetables and berries, they contain a lot of antioxidants (cherries, tomatoes, blueberries).
- Avoid allergens. If you don't know what you might be allergic to, take a food sensitivity test.
- It is better to eat lean meats and avoid red meats. It is better to eat fish and beans during treatment.
- Consume refined foods (sugar, flour products) as little as possible.
- Try to limit your consumption of alcohol and cigarettes.
- Take healthy oils (like olive oil).
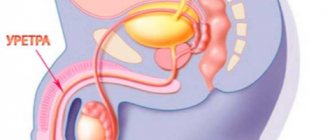
Urethra - what is it? How does it work in men?
In men, the urethra, also called the urethra, is part of the urinary as well as the reproductive system.
It performs several vital functions:
- Excretion of urine accumulated in the bladder.
- During the process of ejaculation, it ensures the release of sperm to the outside.
- Takes part in the mechanism of retention of urine in the bladder for some time.
The length of the male urethra is twenty centimeters. Its location is the pelvis, as well as the penis, from the head of which it opens with a small external opening.
It consists of several departments:
- Distal area.
- Proximal area.
- Membranous.
- Bulbozny.
- Penile.
- Scaphoid fossa.
- External hole.
Almost the entire internal surface of all sections has a mucous membrane, which is formed from transitional epithelium. The exception is a small area located directly next to the external opening - this part is covered with flat non-keratinizing epithelium.
Kidney nephrectomy
Kidneys are one of the vital organs in the human body, thanks to which it gets rid of unnecessary and harmful metabolic products. If the filtration mechanisms are disrupted, then a chain of pathological processes is launched, as a result of which not only the urinary organs suffer, but also the entire body as a whole.
Despite the fact that in the human body the kidneys are presented as symmetrical organs, malfunctions in one of them lead to an increased load on the other. And when we are talking about the complete loss of the kidney’s functions, the consequences of such a condition for the patient’s body can be the most unfavorable.
Considering the entire range of possible causes that most often lead to surgical intervention on the kidneys, it is worth highlighting a group of oncological processes that are listed under code C64-C65 in the ICD 10 heading. Unfortunately, most often radical nephrectomy is performed in patients with a malignant nature of the disease.
Who is the operation indicated for?
Surgeons resort to removing the entire kidney only in emergency situations, when the patient’s condition does not require delay; in all other cases, they always try to preserve it as much as possible (that is, if possible, only the affected tissue is excised).
Radical nephrectomy is always a complex and lengthy procedure that requires the doctor to be highly trained, special skills and good knowledge of anatomy and surgery.
The main indications for complete kidney removal are as follows:
- Severe damage to the kidney tissue, violating its structural integrity, in which it is not possible to restore functional abilities, and there is also massive bleeding from the destroyed vessels.
- Multiple large stones in different structures of the organ with frequent relapses of renal colic.
- Tumor growth of large sizes, when it is not possible to completely remove it from the kidney tissue (more than 6-8 cm).
- Tumor growth into the lumen of large blood vessels (renal and inferior vena cava), into the surrounding adipose tissue, regional lymph nodes, or involvement of adrenal tissue in the pathological process.
- Diagnostically proven single metastases in the tissues of only one kidney, while the second kidney functions normally.
- Severe polycystic disease (most often acquired), which threatens the development of renal failure (ineffectiveness of adequate drug therapy).
- Severe anomalies in the development of the kidneys, when the organ is completely deprived of its functions, and at the same time there are violations that threaten the life and health of the patient.
- Purulent melting of kidney tissue, lack of effect from antibacterial therapy (threat of septic condition).
- Hydronephrosis with an increase in the size of the organ by more than 20% of its original volume, when conservative treatment does not restore the outflow of urine.
Partial nephrectomy is performed in the following categories of patients:
- The presence of a tumor or pathological focus of another origin, the size of which does not exceed 7 cm. It should not extend beyond the kidney and be located in anatomical areas convenient for surgical access (upper or lower pole). In this case, the process does not involve regional vessels and lymph nodes.
- In diseases of both kidneys, when the patient has signs of renal failure, and removing one of them will sharply worsen the patient’s well-being.
There is also a category of patients for whom even complete removal of an organ will improve their condition only temporarily and will not lead to a complete recovery. We are talking about patients with multiple metastases in the kidney tissues and other structures of the body. In this case, they resort to palliative nephrectomy, that is, the “non-functioning” kidney is removed. But at the same time, all metastatic foci remain in the patient’s body.
Contraindications
Radical nephrectomy has a number of limitations, which include:
- A single functioning kidney or severe damage to the second (decompensated disease).
- Diseases of the coagulation system in which there is a risk of bleeding.
- Surgery is not performed on patients who receive large doses of anticoagulants. In this case, surgical intervention is carried out no earlier than 7-10 days after their complete cancellation.
- Decompensated diseases of the cardiovascular system, liver or lungs.
Preparing for surgery
If we are talking about the planned preparation of a patient for surgery, then there is an algorithm of measures that must be completed before the patient goes to the operating table.
The necessary research varies in each specific case, but the basic list is as follows:
- General blood and urine tests.
- Blood chemistry. It is mandatory to determine the level of creatinine, urea, and protein fractions.
- A coagulogram is necessary to assess blood clotting ability.
- Blood for the presence of HIV infection, hepatitis and syphilis.
- In laboratory conditions, the glomerular filtration rate is determined (the filtration capacity of the kidneys is assessed).
- All patients undergo an ECG, and if there are concomitant heart diseases, they are referred for an Echo-CG.
- The functional capabilities of the kidneys are assessed using various instrumental diagnostic methods: ultrasound of the urinary organs; excretory urography; CT or MRI of the kidneys.
- Additional procedures are mandatory to assess the extent of the process and the presence of distant foci of metastasis (chest X-ray, ultrasound and CT of the abdominal and pelvic organs, FGDS, irrigoscopy and others).
Main surgical approaches and types of interventions
Removal of an organ or resection of its part occurs in two available ways:
- open (laparotomy) nephrectomy;
- closed (laparoscopic) nephrectomy.
Each of these approaches has its own advantages and disadvantages, and the preference in choosing each of them depends on the underlying disease, the severity of the patient’s condition and the extent of the process.
If we are talking about emergency surgical intervention, then patients are unconditionally referred to open surgery, thanks to which the doctor can assess the extent of the problem as much as possible and conduct a complete inspection of the lesion.
Open nephrectomy
The site of surgical access and the technique of the operation are no different for left-sided or right-sided nephrectomy.
Radical nephrectomy and partial removal of the organ is performed only under general anesthesia. The patient is fixed on the operating table in order to prevent any displacement of the body.
The incision is made from the front side (left or right) under the costal arch or from the side between the X and XI ribs. Having secured the abdominal organs, the doctor begins to isolate the affected kidney, separating the fascia and fatty component from its surface.
Laparoscopic nephrectomy
The patient is under general anesthesia at the time of the operation. Several punctures are made on its abdominal wall, through which the necessary endoscopic equipment is inserted.
After air is pumped into the lumen of the abdominal cavity and instruments are inserted, it is turned over onto the desired side and fixed in this position.
The affected kidney is removed through the lumen of a large trocar, after which all equipment is removed, and the tissue is sutured layer by layer with absorbable threads.
Considering the progress of the operation during laparoscopy, it becomes clear that this type of surgical intervention is less traumatic and allows the patient to undergo a course of postoperative rehabilitation much earlier, which reduces his time in the hospital.
Possible complications
Like any surgical intervention, kidney nephrectomy can lead to a number of postoperative complications:
- bleeding from a large vessel (if the sutures fail or in a situation where the bleeding vessel went unnoticed by the surgeon);
- the formation of blood clots and their spread through the bloodstream, which threatens thromboembolism and necrosis of those organs where the blood clot is directed;
- suppuration of the area of postoperative sutures (as a result of secondary infection);
- deterioration in the functioning of the heart, lungs or intestines, as an adverse effect of general anesthesia;
- damage to certain nerve trunks, with disruption of the innervation of these areas;
- With laparoscopic access, the development of hernia formations is possible in those places where the trocar was inserted.
Rehabilitation period
The patient's condition after surgery always requires a certain rehabilitation and postoperative recovery, the timing of which directly depends on the underlying disease, surgical approach, the severity of the patient's condition and concomitant pathology.
During this period, patients wear compression stockings, do breathing exercises and smoothly move their limbs (this is necessary to prevent the formation of blood clots in the lumen of the blood vessels).
Eating light food is allowed only on the second day after the patient has undergone surgery. In this case, food should be according to the rules of a special diet, which excludes the intake of fatty and fried foods, spicy and spicy foods. Food is prepared only by steaming or boiling. The diet is expanded only when the patient has a full-fledged stool, without the use of enemas or laxatives.
On the second day after surgery, all patients are seated in bed (with the exception of severely ill patients). Sutures are usually removed on days 10-12, after which the patient is prepared for discharge. Those patients who underwent laparoscopic surgery are sent home after 5-6 days.
For 10 days, treatment with antibacterial drugs and painkillers is prescribed as needed (if the patient suffers from severe pain at the surgical site).
It must be remembered that complete recovery of the body occurs within a period of 12 to 18 months.
If there are any complications or disturbances in the activity of the remaining kidney, the patient is referred to a special commission (ITU), where the issue of establishing a disability group is decided.
The period after surgery requires the patient to comply with a number of requirements, thanks to which the risk of possible complications is minimized and the recovery process is accelerated. Such events include:
- daily walks, which can be combined with light exercise;
- adherence to the principles of proper nutrition and optimal drinking regimen;
- dose the level of physical activity;
- regular visits to the attending physician and timely completion of the necessary tests;
- taking necessary medications.
Possible complications and consequences
When the gland becomes inflamed, a process of scarring of the organ tissue occurs. That is, cells that perform a certain functional load stop doing their job.
As a result, the patient is faced with:
- impotence;
- infertility;
- abscess;
- disturbance of urine outflow;
- spread of inflammation to other organs and systems;
- changes in immune status, development of allergies and autoimmune processes.
Violation of the production of the hormone testosterone leads to a change in the balance in the endocrine system, and the concentration of female hormones estrogen in the blood begins to increase. This leads to changes in the behavior and appearance of a man. His libido decreases, emotionality increases, the location of the fat layer on the body changes, and the size of the mammary glands may increase.
Most of the consequences of the disease are reversible: even if the prostate gland is removed, a man can live a full life. However, he will have to take hormone replacement therapy.
Causes of bleeding from the urethra
Urethrorrhagia occurs solely due to pathologies or damage to the urethra. The degree of urethrorrhagia does not always indicate the severity of the pathological process. Sometimes, when the urethra is ruptured, the bleeding is minor, and with minor damage it becomes life-threatening. Quite rarely, bleeding from the urethra occurs due to tumor processes such as polyposis, angioma or even cancer. Even less often, such conditions occur with chronic urethritis, when the inner layer of the urethra becomes bleeding and loose.
Preventive actions
Preventing the development of the disease involves following various recommendations:
- refusal of promiscuity;
- timely treatment of infectious diseases;
- avoiding hypothermia;
- compliance with personal hygiene rules;
- use of barrier methods of contraception during sexual intercourse;
- timely emptying of the bladder;
- regular exercise in old age;
- refusal to abuse alcoholic beverages;
- balanced diet.
Urethritis in men has a variety of symptoms; treatment of the disease must be comprehensive. Otherwise, the likelihood of developing balanoposthitis, prostatitis, and cystitis increases.