If in an adult patient the amount of urine per day does not exceed 400 ml, this is designated by the term “oliguria”; if no more than 100 ml of urine is excreted per day, the term “anuria” is used. Oliguria often occurs during acute inflammatory processes in the kidneys, acute renal failure or end-stage chronic renal failure; anuria - with obstruction of the urinary tract. Since the blood flow of the kidneys is influenced by nervous and hormonal factors, a decrease in diuresis can sometimes be observed in healthy people, for example, during fear or injury. In kidney diseases accompanied by a decrease in GFR, substances may accumulate in the blood, the excretion of which is due to glomerular filtration. These are primarily urea and creatinine (nitrogenous waste). An increase in the level of nitrogenous waste in the blood is referred to as “azotemia”. With a sharp decrease in functioning nephrons, substances called “uremic toxins” accumulate in the blood. The consequence of a decrease in GFR may also be a disturbance in the composition of the extracellular fluid, with sodium and water retention, accumulation of hydrogen ions and the development of hyperkalemia. At the same time, the severity of homeostasis disorders does not always correlate with the degree of decrease in GFR. For example, with acute damage to the glomerular filter (acute nephritic syndrome), an increase in nitrogenous wastes in the blood is often observed, as well as a significant sodium retention, although a noticeable decrease in GFR is not detected. In slowly progressive forms of kidney damage over a long period, only a moderate decrease in GFR may be detected and homeostasis may remain constant, despite a significant decrease in the mass of functioning nephrons. The absence of consistent patterns between the degree of reduction in GFR and the severity of nephron damage is explained by the individual characteristics of the adaptive capabilities of the kidneys.
An increase in the glomerular filtration rate is possible during pregnancy, a decrease in plasma oncotic pressure, the administration of saline solutions, as well as an increase in the tone of the efferent arteriole and relaxation of the afferent arteriole (for example, in diabetes mellitus). Glomerular filtration rate in the clinic is determined by the clearance of substances. Clearance (C) is the volume of plasma cleared by the kidneys from any substance per unit time, calculated by the formula: where and and P are the concentration of the test substance in urine and plasma, respectively, V is the value of minute diuresis. For these purposes, you can use substances specially introduced into the blood (for example, inulin), or determine clearance by the removal of endogenous substances circulating in the blood (creatinine). In healthy people, the average glomerular filtration rate after correction for body surface area is 130±18 ml/min in men and 120±14 ml/min in women.
Glomerular filtration rate is considered one of the most important indicators of kidney function. This characteristic is necessary to assess kidney function and determine the degree of glomerular damage. Based on the interpretation of the results of the GFR study, it is possible to determine the functionality of this organ.
Glomerular filtration rate, or GFR, is usually assessed by two main characteristics:
- creatinine clearance;
- serum level indicator;
Clearance is the volume of plasma that the kidneys can clear of foreign substances within one minute.
It should be recalled that the kidneys are a kind of filter through which many substances pass. Consequently, the main task of this organ is to ensure the removal of harmful substances and liquids from the body. This filters out useful substances that should remain in the body.
What is SCF
First of all, it is worth noting that glomerular filtration is a process as a result of which fluid with substances dissolved in it is filtered through the renal membrane.
Glomerular filtration rate is a quantitative characteristic of the process of formation of primary urine. The indicators are influenced by the following factors:
- number of functioning nephrons;
- the volume of blood passing through the vessels of the organ for a specific period;
- the total area of capillaries involved in the filtration process.
GFR is usually used to assess such an indicator as the total filtration function of the kidneys. GFR measures how much blood volume can be cleared of creatinine in one minute.
A decrease in GFR levels will indicate a decrease in the number of active nephrons. Moreover, the rate of decline of this indicator is almost always constant. To calculate this indicator, a blood test for GFR is taken.
By comparing the data obtained with normal values, it is possible to determine the ability of the kidneys to cope with the function of cleaning the blood from waste products.
GFR can be measured by units such as inulin clearance. Normally, this substance is not excreted, metabolized, reabsorbed, or produced in the kidneys. In addition, it can be filtered without problems in the glomeruli.
To analyze clearance, all daily urine is needed. The only exception is the morning portion. To evaluate the results obtained, the amount of the substance in the urine is taken into account.
In men, the normal value is 18-21 mg/kg, in women – 15-18 mg/kg. If the analysis reveals a lower value, this indicates either the presence of kidney disease or incorrect urine collection.
GFR is actively used to diagnose kidney diseases. Thus, a decrease in this indicator may indicate the occurrence of a chronic form of renal failure.
In turn, an increase in filtration rate will be a reason to suspect the presence of diabetes mellitus, lupus erythematosus, hypertension and other diseases. Detection of pathologies will indicate damage to the nephrons.
As a result, some of the nephrons die, which leads to the loss of useful substances. In addition, the cessation of the functioning of part of the nephrons causes the retention of water and toxins in the body.
Tubular secretion in the kidneys
The release of some end products of metabolism and foreign substances is ensured, in addition to filtration in the glomeruli, through the process of secretion.
Substances secreted by the cells of the proximal tubule include phenolrot, para-aminohippurate (PAH), diodrast, penicillins, sulfonamides, salicylates, etc. This process is due to the functioning of special active transport systems. Organic substances secreted by cells of the proximal nephron segment
| Substance class | Substance of endogenous origin | Substance of exogenous origin |
| Organic acids | Bile acids | Diodrastus |
| Uric acid | Indomethacin | |
| Oxalic acid | PAG | |
| cAMP | Salicylic acid | |
| Furosemide | ||
| Ethacrynic acid | ||
| Organic bases | Adrenalin | Amiloride |
| Acetylcholine | Atropine | |
| Histamine | Morphine | |
| Serotonin | Quinine | |
| Thiamine |
All sections of the tubules and vessels of the renal medulla, functioning as a countercurrent rotary multiplying system (CMS), participate in the process of concentrating and diluting urine. The countercurrent mechanism is that the movement of tubular fluid in the descending and ascending limbs of the loop of Henle occurs in the opposite direction. The turning mechanism occurs at the limb of the loop of Henle, where the movement of tubular fluid is reversed. The multiplying effect of this system is due to the increase in osmotic pressure towards the top of the pyramids.
Normally, about 65% of the filtered fluid is reabsorbed at the end of the proximal tubule. The descending section of the loop of Henle receives fluid that is isotonic to the plasma, since osmotic substances (sodium, urea, etc.) are also reabsorbed in the proximal section of the nephron. The wall of this section of the loop is permeable to water, but not permeable to salts. As a result, the osmolar concentration increases towards the top of the loop of Henle (vertical concentration gradient).
Osmotic concentration can reach 1500 mosmol/l.
In the ascending limb of the loop of Henle, cells actively reabsorb sodium, potassium, and chlorine without water, since the nephron wall is impermeable to water. As a result, hypotonic fluid (200 mOsmol/L) enters the distal segment of the tubule.
In the collecting ducts of the renal cortex and medulla, under the influence of ADH, facultative reabsorption of water occurs and the concentration of urine increases, so that hyperosmotic urine (1500 mOsmol/L) is ultimately formed and excreted.
Urea plays a special role in the mechanism of osmotic concentration of urine. Unlike the outer medulla, where the increase in osmolarity is caused mainly by sodium, in the inner medulla, along with sodium, urea is of great importance. There is a special system that ensures the circulation of urea. Urea, passing through the distal tubules, the upper parts of the collecting ducts, is not absorbed. When urine reaches the collecting ducts of the medulla, urea, under the influence of ADH, begins to be intensively reabsorbed, increasing the osmotic pressure in the interstitium and thereby promoting abundant reabsorption of water. Urea diffuses through the intercellular substance, penetrates the lumen of the ascending limb of the loop of Henle and moves along the tubule. This is how urea circulates in the kidneys.
Using special methods, it is possible to obtain a quantitative characteristic of the function in various parts of the nephron (filtration in the glomeruli, reabsorption and secretion in the tubules) and, based on the data obtained, form an indirect idea of the severity of structural changes in each of these parts. These methods are based on the principle of determining clearance, or the coefficient of purification of blood plasma from various substances.
Study of renal secretory function
To study the secretory function of the kidneys, the renal clearance of those substances that are excreted from the body only by secretion is studied. Phenolrot meets this requirement, 94% of which is excreted from the body by tubular secretion.
Test method: in the morning on an empty stomach, the patient drinks 400 ml of water or tea and after 15-20 minutes urinates in the toilet. Then he is injected intravenously with 1 ml of 0.6% phenolphthalein solution and two hourly portions of urine are collected. The concentration of phenolrot is determined in each portion. Normally, 40-60% of the drug is excreted in the first portion, and 20-25% in the second. Thus, in 2 hours, about 60-85% of phenolrot is removed from the body.
With kidney diseases and a decrease in the secretory function of the renal tubules, the removal of dye slows down and a larger percentage of it is detected in the second portion of urine.
Study of partial kidney functions
Reasons for changes in glomerular filtration rate
Glomerular filtration rate depends on the following factors:
- blood flow speed in the kidneys. This indicator indicates the volume of plasma flowing through the nephrons over a certain time and filtering in the glomeruli of the kidneys. A result of 600 ml/min indicates normal kidney health. An indicator below this value may indicate the presence of pathological processes;
- blood pressure levels in the kidneys. If the pressure in the incoming vessel is higher than in the outgoing vessel, then this fact will indicate the absence of any diseases;
- number of functioning nephrons. A decrease in the number of functioning nephrons means the presence of pathological processes that can affect the structure of kidney cells. This deviation from the norm causes a decrease in the filtration surface, the size of which affects the rate of glomerular filtration of the kidneys.
- medications that affect creatinine levels. Taking medications such as cephalosporins can increase creatinine levels, resulting in an increase in GFR.
How to improve filtering
It is extremely necessary to restore kidney filtration, especially if there is persistent hypertension. Along with urine, excess electrolytes and fluids are washed out of the body. It is their delay that causes an increase in blood pressure.
To improve renal activity, in particular glomerular filtration, specialists may prescribe medications such as:
Theobromine is a weak diuretic that, by increasing renal blood flow, increases filtration activity; Euphylline is also a diuretic containing theophylline (an alkaloid) and ethylene diamide.
In addition to taking medications, it is necessary to normalize the patient’s general well-being, restore immunity, normalize blood pressure, etc.
To restore kidney function, you also need to eat a balanced diet and follow a daily routine. Only an integrated approach will help normalize the filtration activity of the kidneys.
Folk methods such as the watermelon diet, rosehip infusion, diuretic infusions and herbal infusions, teas, etc. also help a lot in increasing renal activity. But before doing anything, you need to consult a nephrologist.
Glomerular filtration rate is one of the main characteristics reflecting the activity of the kidneys. The filtration function of the kidneys helps doctors diagnose diseases. The glomerular filtration rate indicates whether there is damage to the glomeruli of the kidneys and the degree of their damage, determines their functionality. In medical practice, there are many methods for determining this indicator. Let's figure out what they are and which of them are the most effective.
How to determine GFR
Glomerular filtration rate is usually determined by calculations that take into account the ratio of creatinine in urine and blood.
The glomerular filtration rate can be calculated using special formulas. For this, calculators or computer programs are most often used. Given these possibilities, calculating the GFR does not pose any particular problems.
In order to determine the glomerular filtration rate, the Cockcroft-Gold test is often used. When taking this test, the patient should drink 1.5-2 glasses of water or tea on an empty stomach. Due to this, urine production is activated.
After 20 minutes, the patient needs to completely empty the bladder. Over the next hour, the patient can be at rest. Next, the first collection of all urine is carried out. In this case, it is necessary to note the time of collection.
The next portion of urine is collected to determine GFR after another hour. Between procedures, the patient must undergo a blood test. Based on the data obtained, it is determined whether creatine clearance is falling.
The glomerular filtration rate of the kidneys can also be determined using the MDRD formula. In practice, 2 versions of this formula are used - full and abbreviated.
In the first case, data from biochemical studies will be required to carry out calculations. The abbreviated formula uses only data on sex, age, race, and serum creatinine level.
Determining the glomerular filtration rate makes it possible to draw conclusions regarding the functioning of the kidneys and the stage of renal failure. It is this indicator that is the basis for making a prognosis of the course of the disease. Based on this, treatment regimens are developed.
Filtration violations
Nephrons filter up to 180 liters of primary urine per day. All the blood in the body can be cleansed by the kidneys 60 times per day.
But some factors can provoke disruption of the filtration process:
Reduced pressure; Urinary outflow disorders; Narrowing of the kidney artery; Trauma or damage to the membrane that performs filtering functions; Increased oncotic pressure; Reducing the number of “working” glomeruli.
Such conditions most often cause filtration disorders.
How to determine a violation
Violation of filtration activity is determined by calculating its speed. You can determine how limited filtration is in the kidneys using various formulas. In general, the process of determining the rate comes down to comparing the level of a certain control substance in the patient’s urine and blood.
Typically, inulin, which is a fructose polysaccharide, is used as a comparative standard. Its concentration in the urine is compared with the content in the blood, and then the insulin content is calculated.
The more inulin in urine in relation to its level in the blood, the greater the volume of filtered blood. This indicator is also called inulin clearance and is considered as a value of purified blood. But how to calculate the filtration rate?
The formula for calculating the glomerular filtration rate of the kidneys is as follows:
= GFR (ml/min),
where Min is the amount of inulin in the urine, Pin is the content of inulin in plasma, Vurine is the volume of final urine, and GFR is the glomerular filtration rate.
Renal activity can also be calculated using the Cockcroft-Gault formula, which looks like this:
When measuring filtration in women, the result obtained must be multiplied by 0.85.
Quite often in clinical settings, creatinine clearance is used to measure GFR. Such a study is also called the Rehberg test. In the early morning, the patient drinks 0.5 liters of water and immediately empties the bladder. After this, you need to urinate every hour, collecting urine in different containers and noting the duration of each urination.
Then the venous blood is examined and glomerular filtration is calculated using a special formula:
Fi = (U1/p) x V1,
where Fi is glomerular filtration, U1 is the content of the control component, p is the level of creatinine in the blood, and V1 is the duration of the test urination. Using this formula, a calculation is made every hour throughout the day.
Symptoms
Signs of impaired glomerular filtration are usually reduced to changes of a quantitative (increase or decrease in filtration) and qualitative (proteinuria) nature.
Additional signs include:
Decreased pressure; Renal congestion; Hyperswelling, especially in the area of the limbs and face; Urinary disorders such as decreased or increased urge, the appearance of uncharacteristic sediment or color changes; Pain in the lumbar area Accumulation of various kinds of metabolites in the blood, etc.
A drop in pressure usually occurs during shock or myocardial failure.
Symptoms of glomerular filtration disorder in the kidneys
Norm and deviations
The normal glomerular filtration rate is:
- 95-145 ml/min in men;
- 75-115 ml/min in women.
In children, the norm directly depends on age:
- 2-8 days – 39-60 ml/min;
- 4-28 days – 47-68 ml/min;
- 1-3 months – 58-86 ml/min;
- 3-6 months – 77-114 ml/min;
- 6-12 months – 103-157 ml/min;
- from 1 year – 127-165 ml/min.
Deviation from normal GFR values is explained by many factors. In particular, a decrease in glomerular filtration can occur as a result of the following reasons:
- heart failure;
- insufficiency of thyroid hormones;
- excessive vomiting or diarrhea;
- liver problems;
- malignant prostate tumor;
A steady drop in this indicator in chronic kidney disease is evidence of pronounced chronic renal failure. If the GFR drops to 5 ml/min, this will indicate a problem such as the development of end-stage renal failure.
Decoding the data from the conducted research allows us to obtain the following results:
- reliable. The patient has a reduced GFR, but it is exceeded in patients whose renal function is normal;
- unreliable. These results are observed in patients with unstable serum creatinine levels;
- doubtful. This result is typical for patients with limiting values of such characteristics as age, as well as body weight and volume.
GFR values for disease diagnosis
Glomerular filtration rate is a characteristic on which health status directly depends. This indicator characterizes the filtration function of the kidneys. In addition, it can indicate the possible development of various diseases.
The doctor can draw such a conclusion if the test results deviate from the generally accepted norm. Diagnostic methods used in modern medicine make it possible to determine GFR in the kidneys as accurately as possible.
Due to this, a specialist can give the patient an accurate diagnosis and prescribe dialysis or other procedures that can eliminate existing problems.
Note!
The action of renal and extrarenal factors does not always lead to a pronounced decrease in GFR and vice versa. For example, in case of acute damage to the renal filter (FF), a noticeable increase in nitrogenous wastes in the blood is observed without a pronounced decrease in GFR.
Or, in slowly progressing diseases, GFR does not decrease for a long time, and the number of functioning nephrons has already sharply decreased.
Reason: individual characteristics of the adaptive capabilities of the kidneys.
Increased GFR
– pregnancy, decreased oncotic blood pressure, administration of saline solutions, increased tone of the efferent artery and decreased tone of the afferent vessel.
Determination of GFR
- by ground clearance
Clearance (C) is the volume of plasma cleared by the kidneys from the amount of substance per unit time.
Normal: men 130 ± 18 ml/min, women 120 ± 14 ml/min
V
– the value of minute diuresis.
Test substance:
a) specially introduced into the blood (inulin);
Leave a comment 16,892
Glomerular filtration rate is one of the main characteristics reflecting the activity of the kidneys. The filtration function of the kidneys helps doctors diagnose diseases. The glomerular filtration rate indicates whether there is damage to the glomeruli of the kidneys and the degree of their damage, determines their functionality. In medical practice, there are many methods for determining this indicator. Let's figure out what they are and which of them are the most effective.
Nephron structure
Urine is a concentrate of substances, the removal of which from the body is necessary to maintain a constant internal environment. This is a kind of “waste” from life, including toxic ones, the further transformation of which is impossible, and the accumulation is harmful. The function of removing these substances is performed by the urinary system, the main part of which is the kidneys - biological filters. Blood passes through them, freeing itself from excess fluid and toxins.
A nephron is an integral part of the kidney, thanks to which it performs its function. Normally, the kidney has about 1 million nephrons, and each produces a certain amount of urine. All nephrons are connected by tubules through which urine is collected in the pyelocaliceal system and removed from the body through the urinary tract.
In Fig. Figure 1 schematically shows the structure of the nephron. A – renal corpuscle: 1 – afferent artery; 2– efferent artery; 3 – epithelial layers of the capsule (external and internal); 4 – beginning of the nephron tubule; 5 – vascular glomerulus. B – nephron itself: 1 – glomerular capsule; 2 – nephron tubule; 3 – collecting duct. Blood vessels of the nephron: a – afferent artery; b – efferent artery; c – tubular capillaries; d – nephron vein.
Rice. 1
In various pathological processes, reversible or irreversible damage to the nephrons occurs, as a result of which some of them may cease to perform their functions. The result is a change in urine production (retention of toxins and water, loss of nutrients through the kidneys and other syndromes).
What it is?
In a healthy state, the kidney structure contains 1-1.2 million nephrons (the components of kidney tissue), which communicate with the bloodstream through blood vessels. In the nephron there is a glomerular accumulation of capillaries and tubules that are directly involved in the formation of urine - they cleanse the blood of metabolic products and adjust its composition, that is, they filter primary urine. This process is called glomerular filtration (GF). 100-120 liters of blood are filtered per day.
Scheme of glomerular filtration of the kidneys.
To assess kidney function, glomerular filtration rate (GFR) is very often used. It characterizes the amount of primary urine produced per unit of time. The normal rate of filtration rates ranges from 80 to 125 ml/min (women - up to 110 ml/min, men - up to 125 ml/min). In older people the rate is lower. If an adult has a GFR below 60 ml/min, this is the body’s first signal about the onset of chronic renal failure.
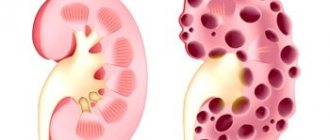
Kidneys and their glomeruli: from normal to pathological
The kidneys are an important organ responsible for homeostasis, or simply put, the physiological balance of the human body. Their main function is to filter urine and remove it from the body. The renal glomeruli are responsible for this process, each of which is a kind of bundle consisting of 50 capillaries. An adult has about 1.5 million such glomeruli and they filter from 120 to 180 liters of fluid daily.
The process of renal filtration is passive in nature and occurs under the influence of the hydrostatic pressure created by the work of the heart. The glomerulus filters the blood plasma, purifying and straining it from defective proteins. As a result, so-called primary urine is formed.
The most important characteristic of glomerular filtration of the kidneys is its rate of flow. It depends both on the general condition of the human body and on the factors that determine the functioning of this organ:
- the value of filtration pressure, which normally should be 20 mm. Hg This is the main factor determining the filtration rate. It acts as the difference between the pressure that occurs in the glomerular capillaries and that which resists the filtration process;
- permeability of the basement membrane, which is the base part of the filter;
- capillary surface area in each glomerulus.
The average normal filtration rate of 125 ml/min for men and 110 ml/min for women is a certain guideline that can be adjusted based on individual characteristics, taking into account not only the person’s gender, but his age, body weight, blood counts and other factors . The glomerular filtration rate of the kidneys is thus established during the diagnostic examination.
Pathological changes are most often associated with a decrease in the filtration rate, less often with its acceleration. But both processes represent a violation of the normal functioning of the body and must be treated.
Factors that change the kidney's glomerular filtration rate
Glomerular filtration rate is determined by several factors:
- The rate of plasma flow in the kidneys is the amount of blood that flows per unit time through the afferent arteriole in the glomerulus. The normal value, if a person is healthy, is 600 ml/min (calculation based on data on an average person weighing 70 kg).
- Pressure level in blood vessels. Normally, when the body is healthy, the pressure in the afferent vessel is higher than in the efferent vessel. Otherwise, the filtration process does not occur.
- Number of functional nephrons. There are pathologies that affect the cellular structure of the kidney, as a result of which the number of capable nephrons is reduced. Such a violation subsequently causes a reduction in the filtration surface area, the size of which directly affects the GFR.
Return to contents
Renal (Malpighian) corpuscles and glomerular filtration
Along with the circulatory system, the kidney has a system of tubules and tubules.
The structural and functional unit of the kidney is the nephron, which consists of the renal (Malpighian) corpuscle connecting to the renal tubule. In the cortex of two kidneys there are about 2.4 million renal corpuscles; each of them contains a glomerular filter, with the help of which the blood is converted into glomerular filtrate. Before urine is produced in the renal tubules, approximately 90% of the glomerular filtrate is reabsorbed. Final concentration occurs in the collecting ducts, which direct urine to the renal pelvis. Each renal corpuscle has a vascular pole and a urinary pole. The vascular pole is where the proximal end of the renal tubule forms a blind sac to which approximately 30 capillary loops (constituting the glomerulus) are attached; a capsule (Bowman's capsule) with a double wall is obtained. The glomerular filtrate emerges into the space between the two walls; it flows into the efferent (efferent) renal tubule, the beginning of which is the urinary pole. The glomerular filtration barrier (its total area reaches approximately 1 m2) includes three layers:
• capillary endothelium; • cells of the visceral (inner) layer of Bowman's capsule (podocytes); • basement membrane, common to endothelial cells and podocytes.
Of these three layers, the basement membrane and podocytes play a particularly important role. The basement membrane is a dense weave of collagen and glycoproteins. As for podocytes with their numerous intertwined processes (“legs”), between these cells there are so-called filtration pores that allow particles of a limited radius to pass through. The glomerular filter is cleaned by podocytes and mesangial cells, which are located between the capillaries and remove the spent basement membrane by phagocytosis. Apparently, podocytes and endothelial cells provide constant renewal of the basement membrane.
Diagram of the structure of the renal glomerulus
Reberg-Tareev test
The Reberg-Tareev test examines the level of clearance of creatinine produced by the body - the volume of blood from which the kidneys can filter 1 mg of creatinine in 1 minute. The amount of creatinine can be measured in clotted plasma and urine. The validity of a study depends on the time at which the analysis was collected. The study is often carried out like this: urine is collected for 2 hours. It measures creatinine levels and minute diuresis (the volume of urine produced per minute). GFR is calculated based on the obtained values of these two indicators. Less commonly used are 24-hour urine collection and 6-hour samples. Regardless of what technique the doctor uses, the patient’s blood is taken from a vein the next morning, before he has had breakfast, to conduct a creatinine clearance test.
A creatinine clearance test is prescribed in the following cases:
- pain in the kidney area, swelling of the eyelids and ankles;
- impaired urination, dark-colored urine with blood;
- it is necessary to establish the correct dose of medications for the treatment of kidney diseases;
- diabetes type 1 and 2;
- hypertension;
- abdominal obesity, insulin resistance syndrome;
- smoking abuse;
- cardiovascular diseases;
- before surgery;
- chronic kidney disease.
Return to contents
Cockcroft-Gold test
The Cockcroft-Gold test also determines the concentration of creatinine in the blood serum, but differs from the method described above for collecting materials for analysis. The test is carried out as follows: in the morning on an empty stomach, the patient drinks 1.5-2 glasses of liquid (water, tea) to activate urine production. After 15 minutes, the patient relieves a small need in the toilet to cleanse the bladder of residual formations during sleep. Next comes peace. An hour later, the first urine sample is taken and its time is recorded. The second portion is collected in the next hour. Between this, 6-8 ml of blood is taken from the patient from a vein. Next, based on the results obtained, the creatinine clearance and the amount of urine that is formed per minute are determined.
Glomerular filtration rate according to MDRD formula
This formula takes into account the gender and age of the patient, so with its help it is very easy to observe how the kidneys change with age. It is very often used to diagnose renal dysfunction in pregnant women. The formula itself looks like this: GFR = 11.33 * Crk - 1.154 * age - 0.203 * K, where Crk is the amount of creatinine in the blood (mmol/l), K is a coefficient depending on gender (in women - 0.742). If this indicator is given in micromoles (µmol/l) at the conclusion of the analysis, then its value must be divided by 1000. The main disadvantage of this calculation method is incorrect results with increased EF.
Reasons for the decrease and increase in the indicator
There are physiological reasons for changes in GFR. During pregnancy, the level increases, and as the body ages, it decreases. Foods high in protein can also provoke an increase in speed. If a person has a pathology of renal function, then EF can either increase or decrease, it all depends on the specific disease. GFR is the earliest indicator of renal dysfunction. The intensity of CF decreases much faster than the ability of the kidneys to concentrate urine is lost and nitrogenous waste accumulates in the blood.
When the kidneys are sick, reduced blood filtration in the kidneys is provoked by disturbances in the structure of the organ: the number of active structural units of the kidney, the ultrafiltration coefficient decreases, changes occur in the renal blood flow, the filtering surface decreases, and obstruction of the kidney tubules occurs. It is caused by chronic diffuse, systemic kidney diseases, nephrosclerosis against the background of arterial hypertension, acute liver failure, severe heart and liver diseases. In addition to kidney disease, extrarenal factors influence GFR. A decrease in speed is observed along with heart and vascular failure, after an attack of severe diarrhea and vomiting, with hypothyroidism, and prostate cancer.
An increase in GFR is a rarer phenomenon, but manifests itself in early stages of diabetes mellitus, hypertension, systemic development of lupus erythematosus, and at the beginning of the development of nephrotic syndrome. Medicines that affect creatinine levels (cephalosporin and similar effects on the body) can also increase the rate of CF. The medicine increases its concentration in the blood, so when taking a test, falsely elevated results are detected.
Load tests
Load tests are based on the ability of the kidneys to accelerate glomerular filtration under the influence of certain substances. With the help of such a study, the CF reserve or renal functional reserve (RFR) is determined. To recognize it, a one-time (acute) load of protein or amino acids is applied, or they are replaced with a small amount of dopamine.
Protein loading involves changing your diet. You need to consume 70-90 grams of protein from meat (1.5 grams of protein per 1 kilogram of body weight), 100 grams of plant proteins, or administer an amino acid set intravenously. People without health problems experience an increase in GFR by 20−65% within 1−2.5 hours after receiving a dose of protein. The average PFR value is 20−35 ml per minute. If there is no increase, then most likely the person’s renal filter permeability is impaired or vascular pathologies develop.
The Importance of Research
It is important to monitor GFR for people with the following conditions:
- chronic and acute course of glomerulonephritis, as well as its secondary appearance;
- renal failure;
- inflammatory processes provoked by bacteria;
- kidney damage due to systemic lupus erythematosus;
- nephrotic syndrome;
- glomerulosclerosis;
- renal amyloidosis;
- nephropathy in diabetes, etc.
These diseases cause a decrease in GFR long before the manifestation of any functional disorders of the kidneys or an increase in the level of creatinine and urea in the patient’s blood. In an advanced state, the disease provokes the need for a kidney transplant. Therefore, in order to prevent the development of any kidney pathologies, it is necessary to regularly conduct studies of their condition.
Glomerular filtration rate is one of the main indicators of kidney health. At the initial stage of its formation, urine is filtered as a liquid contained in the blood plasma into the renal glomerulus, through the small vessels located here into the capsule cavity. This happens as follows:
The capillaries of the kidneys are lined from the inside with flat epithelium, between the cells of which there are tiny holes, the diameter of which does not exceed 100 nanometers. Blood cells cannot pass through them, they are too large for this, while the water contained in the plasma and the substances dissolved in it pass freely through this filter,
the next stage is the basement membrane located inside the renal glomerulus. Its pore size is no more than 3 nm, and the surface is negatively charged. The main task of the basement membrane is to separate protein formations present in the blood plasma from the primary urine. Complete renewal of basement membrane cells occurs at least once a year,
and finally, the primary urine reaches the podocytes, the processes of the epithelium lining the glomerulus capsule. The size of the pores that are located between them is about 10 nm, and the myofibrils present here act as a pump, redirecting primary urine into the glomerular capsule.
The glomerular filtration rate, which is the main quantitative characteristic of this process, refers to the volume of initial urine formed in the kidneys in 1 minute.
Physiological mechanisms of glomerular filtration, tubular reabsorption and secretion.
Back in 1842, the German physiologist K. Ludwig suggested that urine formation consists of 3 processes. In the 20s of the twentieth century, the American physiologist A. Richards confirmed this assumption.
The formation of final urine is the result of three sequential processes:
I. The initial stage of urine formation occurs in the renal glomeruli - glomerular, or glomerular ultrafiltration of protein-free fluid from blood plasma into the capsule of the renal glomerulus, resulting in the formation of primary urine.
II. Tubular reabsorption is the process of reabsorption of filtered substances and water.
III. Secretion. The cells of some sections of the tubule transfer (secrete) a number of organic and inorganic substances from the extracellular fluid into the lumen of the nephron or secrete molecules synthesized in the tubule cell into the lumen of the tubule.
Urine formation begins with glomerular filtration, i.e. transfer of fluid from the glomerular capillaries to Bowman's capsule, while the fluid passes through the glomerular filter.
Filter membrane . The filtration barrier in the renal corpuscle consists of three layers: the endothelium of the glomerular capillaries, the basement membrane and a single layer of epithelial cells lining Bowman's capsule. The first layer, the endothelial cells of the capillaries, is perforated by many openings (“windows” or “fenestrae”) (d pores 40 – 100 nm). The basement membrane is a gel-like, acellular cellular structure consisting of glycoproteins and proteoglycans. Capsular epithelial cells that rest on the basement membrane are called podocytes. Podocytes have an unusual octopus-like structure, resulting in many finger-like processes pressed into the basement membrane. The slit-like spaces between the adjacent finger-like processes are passages through which the filtrate, having passed endothelial cells and the basement membrane, penetrates into Bowman's space (d gaps between the pedicles of podocytes are 24-30 nm)
The basement membrane has pores (d pores 2.9 - 3.7 nm), which limit the passage of blood cells, as well as large molecules more than 5-6 mm (molecular weight more than 70,000). Therefore, large proteins such as globulins (mol. weight 160,000) and caseins (mol. weight 100,000) do not enter the filtrate. Blood plasma albumins (mol. weight about 70,000) pass into the filtrate in negligible quantities. Inulin penetrates into the lumen of the nephron capsule, about 22% of egg albumin, 3% of hemoglobin and less than 0.01% of serum albumin (in the case of hemolysis), thus filtration occurs. The free passage of proteins through the glomerular filter is prevented by negatively charged molecules in the substance of the basement membrane and the lining lying on the surface of podocytes, since the vast majority of plasma proteins carry almost only negative electrical charges. With a certain form of pathology, the kidneys, when the negative charge on the membranes disappears, become “permeable” to proteins.
The permeability of the glomerular filter is determined by the minimum size of molecules that can be filtered. Depends on:
1) pore size
2) pore charge (basal membrane - anion exchanger)
3) hemodynamic conditions
4) the work of pedicles of podocytes (they contain actomyosin filaments) and mesangial cells.
The composition of primary urine is isotonic to blood plasma. Inorganic salts and low molecular weight organic compounds (urea, uric acid, glucose, amino acids, creatinine) freely pass through the glomerular filter and enter the cavity of Bowman's capsule. The main force providing the possibility of ultrafiltration in the renal glomeruli is the hydrostatic pressure of the blood in the vessels. Its value is due to the fact that the afferent arteriole is larger in diameter than the efferent arteriole, as well as the fact that the renal arteries arise from the abdominal aorta.
The filtration area in two kidneys is 1.5 m2 per 100 g of tissue (body S 1.73 m2). Depends on: 1) surface area of the capillaries; 2) the number of pores (more than in any other organ; they account for up to 30% of the surface of endothelial cells); 3) the number of functioning nephrons.
The effective filtration pressure, on which the glomerular filtration rate depends, is determined by the difference between the GBP (hydrostatic blood pressure) in the capillaries of the glomerulus (in humans from 60-90 mm Hg) and the factors counteracting it - the oncotic pressure of blood plasma proteins (TPC is equal to 30 mmHg) and the hydrostatic pressure of the fluid (or ultrafiltrate) or in the glomerular capsule is about 20 mmHg.
EFP (effective filtration pressure). EPD = 70 mmHg. — (30 mm.Hg. + 20 mm.Hg.) 3= 20 mm.Hg.
EPD can vary from 20 to 30 mmHg. Filtration occurs only if the blood pressure in the glomerular capillaries exceeds the sum of the oncotic pressure of proteins in the plasma and the fluid pressure in the glomerular capsule. When filtration pressure increases, diuresis increases, and when it decreases, it decreases. The blood pressure in the capillaries of the glomeruli and the blood flow through them almost do not change, since with an increase in systemic arterial pressure the tone of the afferent arteriole increases, and with a decrease in systemic pressure its tone decreases (Ostroumov-Beilis effect).
The amount of primary urine is 150-180 l/day. 1,700 liters of blood flow through the kidneys per day.
The total surface of the walls of the glomerular capillaries through which filtration occurs is 1.5-2 m2/100 g of kidney, i.e. equal to the surface of the body.
Glomerular filtration rate is 125 ml/min in men and 110 ml/min in women. Thus, about 180 liters per day. The average total volume of plasma in the human body is approximately 3 liters, which means that all plasma is filtered by the kidneys about 60 times per day. The ability of the kidneys to filter such a huge volume of plasma allows them to excrete a significant amount of metabolic end products and very accurately regulate the elemental composition of the internal fluids of the body. In the human kidneys, up to 170 liters of filtrate are formed in one day, and 1-1.5 liters of final urine are released, the rest of the liquid is absorbed in the tubules. Primary urine is isotonic with blood plasma (i.e. it is blood plasma without proteins). Reabsorption of substances in the tubules is to return all vital substances in the required quantities from primary urine.
The molecular mechanisms involved in the implementation of reabsorption processes are the same as the mechanisms operating during the transfer of molecules across plasma membranes in other parts of the body: diffusion, active and passive transport, endocytosis, etc. There are two ways for the movement of reabsorbed substances from the lumen to the interstitial space .
The first is movement between cells, i.e. through the tight junction of two neighboring cells - this is the paracellular pathway . Paracellular reabsorption can occur by diffusion or by transport of the substance along with the solvent. The second route of reabsorption is transcellular (“through” the cell). In this case, the reabsorbed substance must cross two plasma membranes on its way from the lumen of the tubule to the interstitial fluid - the luminal (or apical) membrane, which separates the fluid in the lumen of the tubule from the cytoplasm of the cells, and the basolateral (or counterluminal) membrane, which separates the cytoplasm from the interstitial fluid. Transcellular transport is termed active for short, although the crossing of at least one of two membranes is accomplished by a primary or secondary active process. If a substance is reabsorbed against electrochemical and concentration gradients, the process is called active transport . There are two types of transport - primary active and secondary active . Primary active transport is called when a substance is transferred against an electrochemical gradient due to the energy of cellular metabolism. This transport is provided by the energy obtained directly from the breakdown of ATP molecules. An example is the transport of Na ions, which occurs with the participation of Na+,K+ ATPase, which uses the energy of ATP. Currently, the following primary active transport systems are known: Na+, K+ - ATPase; H+-ATPase; H+,K+-ATPase and Ca+ ATPase.
Secondary active is the transfer of a substance against a concentration gradient, but without the cell expending energy directly on this process, so glucose and amino acids are reabsorbed. From the lumen of the tubule, these organic substances enter the cells of the proximal tubule with the help of a special transporter, which must attach the Na+ ion. This complex (carrier + organic matter + Na+) promotes the movement of the substance through the brush border membrane and its entry into the cell. The driving force for the transfer of these substances through the apical plasma membrane is the sodium concentration in the cell cytoplasm, which is lower than in the lumen of the tubule. The sodium concentration gradient is caused by the direct active removal of sodium from the cell into the extracellular fluid using Na +, K + -ATPase, localized in the lateral and basal membranes of the cell. Reabsorption of Na+ Cl- is the most significant process in terms of volume and energy consumption.
Different parts of the renal tubules differ in their ability to absorb substances. By analyzing fluids from various parts of the nephron, the composition of the fluid and the characteristics of the functioning of all parts of the nephron were established.
Proximal tubule. In the proximal convoluted tubules, most of the components of primary urine are reabsorbed with an equivalent amount of water (the volume of primary urine is reduced by approximately 2/3). In the proximal nephron, amino acids, glucose, vitamins, the required amount of protein, trace elements, and a significant amount of Na+, K+, Ca+, Mg+, Cl_, HCO2 are completely reabsorbed. The proximal tubule plays a major role in returning all these filtered substances to the blood through efficient reabsorption. Filtered glucose is almost completely reabsorbed by the cells of the proximal tubule, and normally a small amount (no more than 130 mg) can be excreted in the urine per day. Glucose moves against the gradient from the tubular lumen through the luminal membrane into the cytoplasm via a sodium cotransport system. This movement of glucose is mediated by a transporter and is a secondary active transport, since the energy required to carry out the movement of glucose across the luminal membrane is generated by the movement of sodium along its electrochemical gradient, i.e. via cotransport. This cotransport mechanism is so powerful that it allows complete absorption of all glucose from the lumen of the tubule. After entering the cell, glucose must cross the basolateral membrane, which occurs through sodium-independent facilitated diffusion; this movement along the gradient is supported by the high concentration of glucose accumulating in the cell due to the activity of the luminal cotransport process. To ensure active transcellular reabsorption, the system operates: with the presence of 2 membranes that are asymmetric with respect to the presence of glucose transporters; energy is released only when it overcomes one membrane, in this case the luminal one. The decisive factor is that the entire process of glucose reabsorption ultimately depends on the primary active transport of sodium. Secondary to active reabsorption, when cotransported with sodium across the luminal membrane, amino acids, inorganic phosphate, sulfate and some organic nutrients are reabsorbed in the same way as glucose. It is necessary to pay attention to the fact that the path of protein reabsorption is significantly different from the methods of absorption of nutrients discussed above. Low molecular weight proteins are reabsorbed by pinocytosis in the proximal segment. Protein reabsorption begins with endocytosis (pinocytosis) at the luminal membrane. This energy-dependent process is initiated by the binding of filtered protein molecules to specific receptors on the luminal membrane. Isolated intracellular vesicles, which appear during endocytosis, merge inside the cell with lysosomes, whose enzymes break down proteins into low molecular weight fragments - dipeptides and amino acids, which are removed into the blood through the basolateral membrane. The excretion of proteins in the urine is normally no more than 20 - 75 mg per day, and with kidney disease it can increase to 50 g per day (proteinuria ).
An increase in the excretion of proteins in the urine (proteinuria) may be due to a violation of their reabsorption or filtration.
Nonionic diffusion - weak organic acids and bases dissociate poorly. They dissolve in the lipid matrix of membranes and are reabsorbed along a concentration gradient. The degree of their dissociation depends on the pH in the tubules: when it decreases, the dissociation of acids decreases and bases increase. Reabsorption of acids increases, bases decreases. As pH increases, the opposite is true. This is used clinically to speed up the elimination of toxic substances - in case of barbiturate poisoning, the blood is alkalized. This increases their content in the urine.
Loop of Henle. In general, the loop of Henle always reabsorbs more sodium and chlorine (about 25% of the amount filtered) than water (10% of the volume of filtered water). This is an important difference between the loop of Henle and the proximal tubule, where water and sodium are reabsorbed in almost equal proportions. The descending portion of the loop does not reabsorb sodium or chloride, but it is very permeable to water and will reabsorb it. The ascending part (both its thin and thick sections) reabsorbs sodium and chlorine and practically does not reabsorb water, since it is completely impermeable to it. The reabsorption of sodium chloride by the ascending part of the loop is responsible for the reabsorption of water in its descending part, i.e. The passage of sodium chloride from the ascending limb into the interstitial fluid increases the osmolarity of this fluid, and this entails greater reabsorption of water through diffusion from the water-permeable descending limb. Therefore, this section of the tubule is called the distributing segment.
As a result, the fluid, already hypoosmotic in the ascending thick part of the loop of Henle (due to the release of sodium), enters the distal convoluted tubule, where the dilution process continues and it becomes even more hypoosmotic, since in subsequent parts of the nephron organic substances are not absorbed into them, only ions are reabsorbed and H2O.
Thus, it can be argued that the distal convoluted tubule and the ascending limb of the loop of Henle function as segments where urine dilution occurs. As it moves along the medullary collecting duct, the tubular fluid becomes more and more hyperosmotic, because reabsorption of sodium and water continues in the collecting ducts, where the final urine is formed (concentrated, due to the regulated reabsorption of water and urea. H2O passes into the interstitial substance according to the laws of osmosis, since there is a higher concentration of substances. The percentage of water reabsorption can vary widely depending on the water balance of a given organism.
Distal reabsorption. Optional, adjustable.
Peculiarities:
1. The walls of the distal segment are poorly permeable to water.
2. Sodium is actively reabsorbed here.
3. Wall permeability is regulated : for water - by antidiuretic hormone, for sodium - by aldosterone.
4. The process of secretion of inorganic substances occurs.
In the distal segment, the final concentration of urine occurs using a special mechanism - rotary-countercurrent-multiplying .
Widely distributed in nature: in the limbs of Arctic animals, blood flows in parallel arteries and veins in such a way that warm arterial blood warms cold venous blood returning to the heart (countercurrent heat exchanger). The entry of low-temperature arterial blood into the foot limits heat transfer.
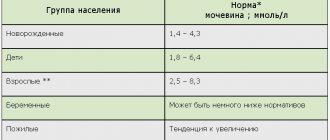
Normal glomerular filtration rate. Explanation of the result (table)
Glomerular filtration rate depends on the age and gender of a person. It is usually measured as follows: after the patient wakes up in the morning, he is given approximately 2 glasses of water to drink. After 15 minutes, he urinates normally, marking the time when urination ends. The patient goes to bed and exactly an hour after finishing urination, he urinates again, collecting urine. Half an hour after the end of urination, blood is drawn from a vein - 6-8 ml. An hour after urination, the patient urinates again and again collects a portion of urine in a separate container. Glomerular filtration rate is determined by the volume of urine collected in each portion and by the clearance of endogenous creatinine in the serum and in the collected urine.
In a normal, healthy, middle-aged person, the normal GFR is:
- in men – 85-140 ml/min,
- in women - 75-128 ml/min.
Then the glomerular filtration rate begins to decrease - over 10 years by approximately 6.5 ml/min.
Glomerular filtration rate is determined when a number of kidney diseases are suspected - it is this that allows you to quickly determine the problem even before the level of urea and creatinine in the blood increases.
The initial stage of chronic renal failure is considered to be a decrease in glomerular filtration rate to 60 ml/min. Renal failure can be compensated - 50-30 ml/min and decompensated when GFR drops to 15 ml/min and below. Intermediate GFR values are called subcompensated renal failure.
If the glomerular filtration rate decreases significantly, then additional examination of the patient is required to find out whether he has kidney damage. If the examination results show nothing, the patient is diagnosed with a decrease in glomerular filtration rate.
Glomerular filtration rate is normal for ordinary people and for pregnant women:
If the glomerular filtration rate is increased, what does this mean?
If the glomerular filtration rate differs from the norm in the direction of increase, this may indicate the development of the following diseases in the patient’s body:
- systemic lupus erythematosus,
- hypertension,
- nephrotic syndrome,
- diabetes.
If the glomerular filtration rate is calculated by creatinine clearance, then you need to remember that taking certain medications can lead to an increase in its concentration in blood tests.
Relevance
The glomerular filtration rate is precisely the amount of fluid processed. It is by measuring the glomerular filtration rate, or GFR, that we can find out how efficiently the kidneys are doing their job and whether they need help. The thing is that with kidney disease, nephrons begin to die. The more of them die, the greater the burden falls on those remaining and the faster they die. As a result, the kidneys begin to cope with their work much worse and soon you will be able to feel the presence of a disease that urgently needs to be gotten rid of.
If the glomerular filtration rate is reduced, what does this mean?
The following pathologies can lead to a decrease in the glomerular filtration rate:
- cardiovascular failure,
- dehydration due to vomiting and diarrhea,
- decreased thyroid function,
- liver diseases,
- acute and chronic glomerulonephritis,
- prostate tumors in men.
A sustained decrease in glomerular filtration rate to 40 ml/min is usually called severe renal failure; a decrease to 5 ml/min or less is the end stage of chronic renal failure.
Glomerular filtration rate (GFR) is a sensitive indicator of the functional state of the kidneys; its decrease is considered one of the early symptoms of renal dysfunction. A decrease in GFR, as a rule, occurs much earlier than a decrease in the concentration function of the kidneys and the accumulation of nitrogenous waste in the blood. In case of primary glomerular lesions, insufficiency of renal concentrating function is detected with a sharp decrease in GFR (by approximately 40-50%). In chronic pyelonephritis, the distal part of the tubules is predominantly affected, and filtration decreases later than the concentration function of the tubules. Impairment of the concentration function of the kidneys and sometimes even a slight increase in the content of nitrogenous waste in the blood in patients with chronic pyelonephritis is possible in the absence of a decrease in GFR.
GFR is influenced by extrarenal factors. Thus, GFR decreases with heart and vascular failure, profuse diarrhea and vomiting, hypothyroidism, mechanical obstruction of urine outflow (prostate tumors), and liver damage. In the initial stage of acute glomerulonephritis, a decrease in GFR occurs not only as a result of impaired patency of the glomerular membrane, but also as a result of hemodynamic disorders. In chronic glomerulonephritis, a decrease in GFR may be due to azotemic vomiting and diarrhea.
A persistent drop in GFR to 40 ml/min in chronic renal pathology indicates severe renal failure, a drop to 15-5 ml/min indicates the development of terminal chronic renal failure.
Some drugs (for example, cimetidine, trimethoprim) reduce tubular secretion of creatinine, increasing its concentration in the blood serum. Antibiotics of the cephalosporin group, due to interference, lead to falsely elevated results in determining creatinine concentration.
Laboratory criteria for the stages of chronic renal failure
Blood creatinine, mmol/l
GFR, % of predicted
An increase in GFR is observed in chronic glomerulonephritis with nephrotic syndrome, in the early stages of hypertension. It should be remembered that in nephrotic syndrome, the clearance of endogenous creatinine does not always correspond to the true state of GFR. This is due to the fact that in nephrotic syndrome, creatinine is secreted not only by the glomeruli, but is also secreted by the altered tubular epithelium, and therefore Koch. endogenous creatinine can be up to 30% higher than the true volume of glomerular filtrate.
The clearance of endogenous creatinine is influenced by the secretion of creatinine by renal tubular cells, so its clearance may significantly exceed the true value of GFR, especially in patients with kidney disease. To obtain accurate results, it is extremely important to completely collect urine within a precisely specified period of time; incorrect collection of urine will lead to false results.
In some cases, to increase the accuracy of determining endogenous creatinine clearance, H2-histamine receptor antagonists (usually cimetidine at a dose of 1200 mg 2 hours before the start of 24-hour urine collection) are prescribed, which block tubular secretion of creatinine. Endogenous creatinine clearance measured after taking cimetidine is almost equal to the true GFR (even in patients with moderate to severe renal impairment).
To do this, it is necessary to know the patient’s body weight (kg), age (years) and serum creatinine concentration (mg%). Initially, a straight line connects the patient’s age and his body weight and marks a point on line A. Then mark the concentration of creatinine in the blood serum on the scale and connect it with a straight line to a point on line A, continuing it until it intersects with the endogenous creatinine clearance scale. The point of intersection of the straight line with the endogenous creatinine clearance scale corresponds to GFR.
Tubular reabsorption. Tubular reabsorption (CR) is calculated from the difference between glomerular filtration and minute diuresis (D) and is calculated as a percentage of glomerular filtration using the formula: CR = [(GFR-D)/GFR]×100. Normal tubular reabsorption ranges from 95 to 99% of the glomerular filtrate.
Tubular reabsorption can vary significantly under physiological conditions, decreasing by up to 90% with water loading. A marked decrease in reabsorption occurs with forced diuresis caused by diuretics. The greatest decrease in tubular reabsorption is observed in patients with diabetes insipidus. A persistent decrease in water reabsorption below 97-95% is observed with primary and secondary wrinkled kidneys and chronic pyelonephritis. Water reabsorption may also decrease in acute pyelonephritis. In pyelonephritis, reabsorption decreases before the GFR decreases. In glomerulonephritis, reabsorption decreases later than GFR. Usually, along with a decrease in water reabsorption, insufficiency of the concentration function of the kidneys is detected. In this regard, a decrease in water reabsorption in the functional diagnosis of the kidneys does not have much clinical significance.
An increase in tubular reabsorption is possible with nephritis and nephrotic syndrome.
Every day, 70-75% of all fluid consumed during the day is excreted from the human body. This work is done by the kidneys. The functioning of this system depends on factors, one of which remains glomerular filtration.
Reasons for the decline
Glomerular filtration is a process of processing blood entering the kidneys that occurs in the nephrons. The blood is purified 60 times per day. Normal blood pressure is 20 mmHg. The filtration rate depends on the area occupied by the nephron capillaries, pressure and membrane permeability.
When glomerular filtration is impaired, two processes can occur: a decrease and an increase in function.
A decrease in glomerular activity can be caused by factors both related to the kidneys and extrarenal:
- hypotension;
- narrowed renal artery;
- high oncotic pressure;
- membrane damage;
- decrease in the number of glomeruli;
- impaired urinary outflow.
Factors that stimulate the development of glomerular filtration disorders cause further development of diseases:
- a decrease in pressure occurs under stressful conditions, with severe pain, leading to cardiac decompensation;
- narrowing of the arteries leads to hypertension, lack of urine with severe pain;
- anuria leads to a complete cessation of filtration.
A reduction in the area of the glomeruli may be associated with inflammatory processes and sclerosis of blood vessels.
With hypertension and cardiac decompensation, the permeability of the membrane increases, but filtration is reduced: some of the glomeruli are switched off from performing their function.
If glomerular permeability is increased, protein yield may increase. This causes proteinuria.
The concept of glomerular filtration
The process of urine formation consists of several stages. At each stage, a failure may occur, leading to dysfunction of the entire organ. The first stage of urine formation is called glomerular filtration.
It is carried out by the renal corpuscle. It consists of a network of small arteries formed in the form of a glomerulus surrounded by a two-layer capsule. The inner layer of the capsule fits tightly to the walls of the arteries, forming a renal membrane (glomerular filter, from the Latin glomerulus - glomerulus).
It consists of the following elements:
- endothelial cells (the inner “lining” of arteries);
- epithelial capsule cells forming its inner layer;
- layer of connective tissue (basal membrane).
It is through the renal membrane that water and various substances are released, and its condition determines how fully the kidneys perform their function.
Large (protein) molecules and cellular elements of the blood do not pass through the kidney membrane. In some diseases, they can still pass through it due to its increased permeability and end up in the urine.
The solution of ions and small molecules in the filtered liquid is called primary urine. The content of substances in its composition is very low. It is similar to plasma from which the protein has been removed. The kidneys filter from 150 to 190 liters of primary urine in one day. During the further transformation that primary urine undergoes in the nephron tubules, its final volume decreases by approximately 100 times, to 1.5 liters (secondary urine).
Increased filtration
Impairment of glomerular filtration can be observed both in a decrease and in an increase in the growth rate. This dysfunction is unsafe. The reasons may be:
- reduced oncotic pressure;
- changes in pressure in the outgoing and incoming arterioles.
Such spasms can be observed in diseases:
- nephritis;
- hypertension;
- administration of a small dose of adrenaline;
- impaired blood circulation in peripheral vessels;
- blood thinning;
- copious introduction of fluid into the body.
Any abnormalities associated with glomerular filtration should be under the attention of a physician. An analysis to identify them is usually prescribed for existing suspicions of kidney disease, heart disease and other pathologies that indirectly lead to renal dysfunction.
How to determine?
A test is prescribed to determine the rate of filtration in the kidneys. It consists in determining the clearance rate, i.e. substances that are filtered in the blood plasma and do not undergo reabsorption or secretion. One of these substances is creatinine.
Normal glomerular filtration rate is 120 ml per minute. However, fluctuations in the range from 80 to 180 ml per minute are acceptable. If the volume goes beyond these limits, you need to look for the reason.
Previously, other tests were carried out in medicine to determine disorders of glomerular functioning. The basis was taken on substances that were administered intravenously. It takes several hours to observe how they are filtered. Blood plasma was taken for research, and the concentration of administered substances was determined. But this process is difficult, so today they resort to a simplified version of tests that measure creatinine levels.
How does urine filtration occur?
To understand the process of urine filtration in the kidneys, it is necessary to take a brief excursion into the structure and functions of this paired organ.
The following main functions of the kidneys are distinguished:
- Urination;
- Removing various substances and purifying the blood;
- Blood circulation control;
- Control of electrolyte balance;
- Control of homeostasis.
The buds look like beans due to their shape. On each of the kidneys there is a small recess (the so-called “gate”) through which you can enter the area filled with fat. Also in this sinus are located blood vessels, nerves and the collecting apparatus. The ureters and large vessels depart from the hilum.
The kidneys consist of approximately 1 million nephrons (the so-called structural and functional unit of the kidney) - a set of glomeruli and tubules. It is in the tubule that filtration occurs - urine is separated from the blood and accumulates in the bladder.
Glomerular filtration is quite simple:
- This is a passive process. Under the pressure of fluids exerted by the work of the heart, fluid is squeezed out and filtered from the glomerular membranes.
- Next, the nephrons filter the liquid, while useful substances go back into the blood, and everything unnecessary, in the form of urine, accumulates in the bladder.
- Urine is produced at an average rate of 1 ml per minute.